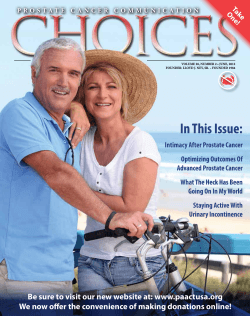
Queensland Prostate Cancer News The magazine is a publication of the Queensland Chapter, Prostate Cancer Foundation of Australia. December 2011 In this issue Guest Editorial, Do women really care? Christmas is approaching and usually we take the time to send our best wishes to family and friends whom we haven’t caught up with a lot throughout the year. An act of kindness most of us do because we care. No doubt for many who have received the diagnosis of Prostate Cancer in 2011 it will have been momentous for you as an individual and as a couple. Moving into 2012 may be filled with apprehension, fear and anxiety for what the future holds for you both. As a woman you will now be termed a carer if you have a spouse with Prostate Cancer. It’s a strange, unwelcome and not very comfortable title to have. At least that was my experience. But this role we assume, adopt and run with at the time because of necessity and the circumstance even though it’s very unfamiliar territory to us. Post operatively as a carer our lives seem to take on a whole new dimension. It is determined by how we best support, care for and attend to the needs of our spouse. It then moves into another stage as he recovers: of follow up care, encouragement and understanding despite being on our own emotional roller coaster. It is no surprise then that men with Prostate Cancer become more dependent on their partners to act as their primary communicator and caregiver. Duty of care is an aspect of the professional and medical world we hear so much about, though not something written into our traditional marriage vows. It’s more along the lines of �love, honour and cherish’. As a couple you don’t sit down together and work out your own personal duty of care statements. It becomes an automatic response in your relationship, motivated by your depth of feeling and concern for each other, based on each other’s needs. When your spouse has Prostate Cancer and he is in need of care, that’s exactly what you do, to the very best of your ability. Being a carer is an inbuilt and unique quality that women have. It emerges when our loved one is faced with a disease that is potentially life threatening. Do women care out of duty or is it our duty to care? No, neither! It’s something women do because we genuinely do care, but more importantly because we love. But who cares for the carer? Other carers of course! Those who are in a similar situation to your own! Women do really care. Maggie Fincham Angus, Coordinator of the Gold Coast Prostate Cancer Partners Support Group. Phone 0427 359 375 or email: goodworthideas@bigpond.com Calendar of Events 2011/12 Resources: Web Links, Associated and Affiliated Groups. 3 SPOTLIGHT ON North West Queensland (Mt Isa). 4 New “Wonder Drug”. Diet & Cancer. 5 Prostate Cancer Update. 9 Gympie Member’s Final Project. MMRI Research. 10 Convener a Proud Australian. 11 News Roundup. 12 Mummys Get Prostate Cancer. Vacuum Erection device aids recovery after surgery. 13Hypofractionated Radiotherapy Report. 14 Cancer Etiquette. 15 Combination Therapies for High-Risk Disease. QOL After Brachytherapy. 16 Brisbane Program: Prostate Cancer Foundation of Australia www.prostate.org.au Cancer Council Queensland www.cancerqld.org.au Dec 01 World AIDS Day www.worldaidsday.org.au Jan 30 Medicine Wise Week www.nps.org.au Anytime C-vivor (free sessions) www.cancerqld.org.au Anytime Barbeque for Prostate Cancer www.pcfa.org.au www.pcfa.org.au 2 T 1800 22 00 99 T 1300 65 65 85 Privacy: Contact Us: Disclaimer. qpcn@cancerqld.org.au The Queensland Chapter of the Prostate Cancer Foundation of Australia is grateful for the generous support of Cancer Council Queensland, in the printing of this magazine. The content of this magazine is selected by the Queensland Chapter of the PCFA. Cancer Council Queensland does not necessarily endorse, or otherwise, any content contained within this publication. Resources Andrology Australia www.andrologyaustralia.org Ph 1300 303 878 Andrology Australia is the Australian Centre of Excellence in Male Reproductive Health. APCC Bio-Resource www.apccbioresource.org.au The national tissue resource underpinning continuing research into prostate cancer. Australian Prostate Research Centre – Queensland www.australianprostatecentre.org Research, collaborative opportunities, clinical trials, industry news. Cancer Council Helpline Ph 13 11 20 8am-6pm Monday to Friday. www.cancerqld.org.au/cancerHelpline Cancer Council Queensland www.cancerqld.org.au Research to beat cancer and comprehensive community support services. Cochrane Library www.cochrane.org Australians now have free access to the best available evidence to aid decision-making. HealthInsite www.healthinsite.gov.au Your gateway to a range of reliable, up-to-date information on important health topics. Lions Australian Prostate Cancer www.prostatehealth.org.au The first stop for newly diagnosed men seeking information on the disease. Mater Prostate Cancer Research Centre www.mmri.mater.org.au Comprehensive information for those affected by prostate cancer, including the latest research news. Prostate Cancer Foundation of Australia www.prostate.org.au Phone 1800 22 00 99 Assistance with the experience of diagnosis and treatment for prostate cancer. Queensland Chapter www.prostate.org.au Information, patient support materials, and contacts for advice on living with prostate cancer in Queensland. Prostate Cancer Support Groups in the Queensland Chapter There are 23 PCSGs in the Chapter with a total membership of approximately 3,300 men. Peer Support Group Contact Phone Peer Support Group Contact Phone Beenleigh Peter Keech 0407 070 194 Mackay John Clinton 07 4942 0132 Brisbane Peter Dornan 07 3371 9155 Maryborough Leoll Barron 07 4123 1190 Bundaberg Rob McCulloch 07 4159 9419 Mount Isa Tony McGrady 07 4743 2740 Capricorn Coast (Yeppoon) Jack Dallachy 07 4933 6466 North Burnett Russell Tyler 07 4161 1306 Central Qld. (Rockhampton) Lloyd Younger 07 4928 6655 Northern Rivers (Alstonville) Pat Coughlan 02 6622 1545 02 6684 2201 Jim Hope 07 4039 0335 Northen Rivers (Lismore) Warren Rose Far North Qld. (Cairns) 07 5446 1318 Geoff Lester 07 4979 2725 Sunshine Coast (Maroochydore) Rob Tonge Gladstone Gold Coast North John Caldwell 07 5594 7317 Toowoomba David Abrahams 07 4613 6974 Gold Coast Partners Maggie Angus 07 5577 5507 Bob O’Sullivan 0405 274 222 Gold Coast Central (Evening Group) Peter Jamieson 07 5570 1903 North Queensland (Townsville) Ross Davis 07 5599 7576 Gympie and District Robert Griffin 07 5482 4659 Twin Towns & Tweed Coast Hervey Bay (Pialba) Ros Male 07 4125 6701 Whitsunday (Proserpine) Dave Roberts 07 4945 4886 Ipswich Terry Carter 07 3281 2894 The news sheet for any group should have the meeting details for its neighbouring groups. Associated Support Groups 2 Group Contact Phone Sponsor Beaudesert Carmen O’Neill RN 07 5541 9231 Beaudesert Health/Gold Coast Kingaroy Robert Horn 07 4162 5552 Toowoomba/Sunshine Coast SPOTLIGHT on North West Queensland (Mt Isa) Our inaugural Convener, George Apps, passed away in June 2010. George’s passing was a great loss to our Group and indeed to the Mt Isa community in general as he was involved in many community activities through Lions, Rotary and other organisations. Writing in “Queensland Prostate Cancer News” a few months prior to his death George wrote, “Our fledgling Group shares the dedication of other Groups to be part of the fight against prostate cancer and all cancer generally. We have just begun but we intend to succeed in our endeavours.” The North West Queensland Prostate Cancer Support Group has honoured George’s vision under the stewardship of Yvonne McCoy and Tony McGrady, by increasing community awareness of the toll this disease wreaks on Australian men and raising funds for prostate cancer research. Our region covers some 30,000 square kilometres and, apart from Mt Isa, encompasses eleven other communities. Whilst the area’s health care is administered by North West Queensland Primary Health Care, the nearest treatment centres for prostate cancer are 1,000 kilometres plus away to the East. The demographics of the region include a high proportion of males and the remoteness of some of the communities present us with a real challenge when it comes to spreading the (prostate cancer) word. We currently have around 60 Support Group members on our mailing list and this number is constantly increasing. One of our members, Kyle Small, has sought and obtained sponsorship from a number of local businesses and Kyle has used their support to set up a “buggy” which has been a drawcard at a number of local events. Towards the end of last month the Mt Isa Civic Centre held “Carols by Candlelight” which concluded with a fireworks display. The event attracted a large number of men and their families, a good mix for promoting the need for men to check for prostate cancer as they reach middle age (if they forget to follow up their partners will be there to remind them!). We set up an awareness booth which drew plenty of attention and requests for literature. All proceeds from the night were donated to our Support Group; a very rewarding evening. We are currently involved in the establishment of a “Men’s Shed” in Mt Isa which we see as an ideal venue to promote our cause. Our Support Group have applied to the local Council for a lease over part of the Frank Ashton Underground Museum to set up the “Shed”. Mt Isa Mayor, Cr John Molony, has appointed Cr Robbie Katter as his liaison officer with our Group. Cr Katter has stated that “I fully support the concept of a Men’s Shed and will be doing all in my power to ensure that this brilliant idea becomes a reality. I have spoken to a number of Mt Isa families and the support in the community is there in abundance. This is what community is all about, the people working with their Council to achieve things. I am right behind this concept and working together we can make it happen.” The Support Group Chairman, Tony McGrady, said that the Mayor had informed him that there were other venues which could be available if the Frank Ashton site was not mutually acceptable. Earlier in the year we had an awareness booth set up at the Mt Isa Mining Expo. Many national and international companies participated in this exhibition of mining machinery, techniques, trends and research and attendance was as diverse as the exhibitors. Our booth got plenty of attention from the mostly male attendees. “The Buggy” – Getting the Awareness Message to the Community. Last August the “buggy”, with Kyle in the driver’s seat and ably assisted by his trusty steed Wally in the shafts, undertook an awareness drive from Mt Isa to Camooweal. At around 20 kilometres per day the trip took ten days and Kyle and Wally’s arrival in Camooweal coincided with the town’s Drovers’ Festival. Kyle’s family and a number of local men organised a back-up team for the trip and the group “rattled the tin” and handed out prostate cancer literature along the way. The “Horse & Buggy Drive” was a great success as both an awareness event and fundraiser. In the annual street parade, which forms part of the Festival, Kyle and Wally were awarded first place. Kyle Small is Presented With His Trophy by Yvonne McCoy for First Place in the Camooweal Drovers’ Festival Street Parade. Support Group Member Terry McCoy at the Mining Expo Booth. It’s too early to know the awareness and fundraising results as yet but one of Mt Isa’s premier sporting teams from the Euros Rugby Union Football Club put the spotlight on men’s health when they agreed to participate in MOvember. Club secretary, Amber Liddle, said “I came up with the idea of the team donating to a charity each season and at the last meeting we held one of the players suggested taking part in MOvember. Participating in MOvember this year will help raise funds and awareness to the two most common health problems men tend to face, prostate cancer and depression.” If you’re in Mt Isa, on business, holidays or a grey nomad passing through, we’d love to see you and have you attend one of our meetings if the timing is appropriate. Yvonne McCoy Tony McGrady 07-4743 2054 0400 798 315 3 THE NEW “WONDER DRUG” FOR CANCER Professor Sanchia Aranda, director of cancer services and information at the Cancer Institute NSW talks about the importance of exercise in improving survival from cancer. With Australians failing to take on the exercise message, how much harder is it to sell exercise to someone undergoing treatment for cancer? For most of us, the natural instinct when we are sick is to rest, especially if the sickness is cancer and fatigue its most common complication. But, evidence suggests that one of the best ways to prevent or minimise cancer fatigue is to maintain as much normal activity as possible during and after treatment. The advice that people with cancer should rest and take it easy is outdated and health professionals have an obligation to promote evidence of the clinical benefits of exercise, such as the reduced risk of infection, deep vein thrombosis and loss of muscle mass should resonate. And, yes, that means exercise. What better opportunity for clinicians to encourage an active lifestyle than at a time when patients are receptive to new ideas and motivated to make changes? People with cancer regularly ask what they can do to keep themselves well, while health professionals struggle with the response to this question. Clearly, promoting a healthy diet and increased activity are ideal self-care messages. MOVE MORE: A new study by British advocacy group Macmillan Cancer Support, is calling exercise a 'wonder drug', with evidence that it not only combats fatigue, depression and anxiety, but that twoand-half-hours per week significantly reduces the risk of people with breast, prostate and bowel cancers dying from their disease. The group is calling for exercise to be incorporated into standard cancer care, as part of clinical guidelines and quality standards, supported by subsidised gym programs and facilities specifically for people with cancer. The advice that people with cancer should rest and take it easy is outdated and health professionals have an obligation to promote evidence of the clinical benefits of exercise. How would this work in the Australian setting? Australians are leading increasingly sedentary lives and obesity rates are alarming, despite the rapidly growing fitness industry. It's important patients feel encouraged and supported to talk to their doctor, nurse or physiotherapist about what exercise is suitable for them during and after cancer treatment. In general, the person with cancer is the best guide on the level of exercise that feels right for them. They should be encouraged to increase their exercise, but not to the point of exhaustion. Friends and family members are also an important help and are often looking for things they can do to help their loved one get well. Families are in an ideal position to go for a walk with the person being treated for cancer, to help them maintain independence and keep active, rather than always rushing to do things for them that reduce the amount of exercise and activity severely. A family exercise prescription will have benefits for everyone! EATING EGGS, DAIRY, RED MEAT AND POULTRY MAY INCREASE YOUR RISK OF PROSTATE CANCER How do you like your eggs? Over easy? Scrambled? How about switching to oatmeal? A new US study found that eating eggs may increase your risk of developing advanced prostate cancer. This is on top of the other evidence over recent years that link dairy and prostate cancer and meat and prostate cancer. Researchers from the University of California, San Francisco, and Harvard School of Public Health evaluated data from 27,607 men who had been followed from 1994 to 2008 and who were prostate cancer-free at the beginning of the period. They discovered that healthy men who ate 2.5 eggs or more each per week had an 81% higher risk of developing advanced prostate cancer compared with men who ate fewer than 0.5 eggs per week on average. As an aside, they also noted a “suggestion” that eating poultry and processed red meat after a diagnosis of localised prostate cancer was linked to progression to advanced prostate cancer. Previous research, however, has indicated a more significant association. 4 In a study conducted by the National Cancer Institute of more than 175,000 men and spanning the years 1995 to 2003, the investigators found that men who ate the most red meat were 12% more likely to develop prostate cancer and 33% more likely to develop advanced cancer than men who ate the least amount of red meat. It appears eating eggs can do more than raise your cholesterol level. If you want to improve your chances of avoiding advanced prostate cancer, skip the steak and eggs and scrambled eggs and bacon. Sources: Richman EL et al. Egg, red meat, and poultry intake and risk of lethal prostate cancer in the prostate specific antigen-era: incidence and survival. Cancer Prev Res 2011 Sep; DOI: 10.1158/1940-6207 Sinha R et al. Meat and meat-related compounds and risk of prostate cancer in a large prospective cohort study in the United States. Am J Epidemiol 2009 Nov 1; 179(9): 1165-77. PROSTATE CANCER UPDATE At the Brisbane Group’s annual prostate cancer awareness evening Urological Surgeon, Dr Roger Watson and Radiation Oncologist, Dr Tiffany Daly gave a prostate cancer update covering the scale of the problem, management of the disease and the current treatment regimes generally used for cure or control. The value of screening for prostate cancer has been widely debated for many years. Prostate Cancer Foundation of Australia recommends that men should be tested from age 50 or earlier if there’s a family history of the disease. Ideally screening should consist of a PSA (prostate-specific antigen) blood test plus a DRE (digital rectal examination) followed by a prostate biopsy if the initial testing shows any irregularities. The advantage of screening allows men an opportunity to detect early cancer and successfully treat it, hence reducing the burden of advanced prostate cancer and/or reducing the death rate from the disease. Dr Tiffany Daly Dr Roger Watson The prostate gland is situated at the base of the bladder in men. At puberty male hormones secreted by the testes stimulate prostate growth until it becomes about the size of a walnut. The urethra, the tube that carries urine from the bladder to the penis, runs through its centre. Ejaculatory ducts that carry mature sperm also run through the gland and during ejaculation the prostate secretes a milky alkaline fluid which then becomes a constituent of sperm. The disadvantages include the fact that the cancer may be slowgrowing and not become dangerous (particularly in older men who may die “with the disease rather than of it”), the test is not 100% accurate so it may give false positives or false negatives and unnecessary treatment of slow-growing cancers can produce side effects, particularly altered sexual function, which can significantly impair quality of life. Unfortunately there’s currently no way of distinguishing aggressive cancers from those which are slow growing. Whilst early prostate cancer is generally symptomless, once the tumour grows symptoms may arise including bladder plumbing problems (difficulty and/or pain when voiding and blood in the urine) and it may spread to the lymph nodes and bones causing the bones to become brittle and painful. Once this occurs the cancer is advanced or metastatic and control may be possible but a cure unlikely. Even when a man exhibits “plumbing problems”, prostate cancer may not be the culprit. BPH (benign prostatic hyperplasia or benign enlargement) is common as men age and may cause difficulties when urinating. Prostatitis can cause the prostate to become inflamed and swell causing discomfort and pain. Both these conditions are generally easily treatable, the first with a TURP (trans urethral resection of the prostate, commonly called a “re-bore”) and the second with a course of antibiotics. Whilst lung cancer is still the largest killer of Australian men, prostate cancer is the most commonly diagnosed cancer excluding nonmelanoma skin cancers. Diagnoses this year are expected to exceed 20,000 and this figure will grow alarmingly over the next decade as the Australian population ages and the “baby-boomers” and early “Gen X-ers” reach the 55 – 75 age group, the most common ages for prostate cancer to be diagnosed. Because of the possibility of these other prostate problems, symptoms alone are not a reliable indication for diagnosing prostate cancer. The PSA test has been improved since its adoption in the late 1980s. Age related allowances, patterns over time with regular testing and the total versus free-PSA levels all assist with more accurate diagnostic predictions. In conjunction with a DRE by which a trained professional may detect any prostate irregularities, the PSA gives a reasonable indication of the presence of cancer or otherwise. However if there are positive indications or if doubts remain the only definitive test is a prostate biopsy. This is generally a TRUS (transrectal ultrasound guided needle biopsy of the prostate although it can be carried out through the perineum rather than the rectum). It’s an outpatient procedure carried out in a hospital’s endoscopy unit. The patient is lightly sedated for comfort and antibiotics are given to prevent infection. There is a low but defined risk of infection but this rarely requires in-hospital care. Continued... 5 When the biopsy is carried out via the perineum (a transperineal ultrasound guided biopsy) there is less risk of infection and its more likely to be able to diagnose anterior and smaller tumours however the procedure requires a general anaesthetic in a hospital operating theatre and there’s an increased chance of increased urinary symptoms and bleeding. During the biopsy 12 – 20 cores will be taken for analysis by a pathologist. The subsequent pathology report may rule out cancer, the prostate problems may be due to BPH or inflammation, or indicate that cancerous cells are present or that there are PIN (prostatic intraepithelial neoplasia) and atypia cells present. PIN is a condition between normal and cancerous, cells that are likely to evolve into cancer cells, and atypia cells are not cancerous but not typical either. Once the cancer has spread beyond the prostate into the surrounding tissue or spread further afield (metastatic), a cure may not be possible and the treatment options for localised disease may no longer be suitable. However androgen deprivation therapy may be recommended to control the tumour growth. Other factors to be taken into account when deciding on the way ahead are the age and health of a patient. A 70 year old man who has been diagnosed with early localised prostate cancer but is overweight, has diabetes and a history of cardiovascular problems will most likely die long before the prostate cancer is cause for concern whereas, if the 70 year old was in good physical condition with no other health issues, he could have another 20 years of productive life ahead of him and treatment may be in order. Problems with anaesthetics may rule out surgery for some and the time taken to complete a course of radiotherapy versus a short hospital stay for surgery may sway some men towards surgery where both types of treatment could be considered. If you’re not completely happy or confused about the way ahead following the discussion with your doctor about treatment options, it’s always worthwhile getting a second opinion. From the biopsy results the prostate tumour will be assigned a Gleason score. The cancer cells are numerically graded from 1 to 5 (the lower the grade the less potential for aggressive cancer) and the Gleason score is arrived at by adding the two most common grades from the biopsy giving a figure of between 2 and 10. For example the most common grade may be 3 and the next may be grade 4 so the Gleason score will be 7 (3+4). Gleason scores of 4 or less indicate a tumour of low aggressiveness, 5-6 is moderate, 7 intermediate and 8-10 is high. Once prostate cancer has been confirmed your doctor will probably want further tests carried out such as a CT/CT PET (computerised tomography) scan, MRI (magnetic resonance imaging) scan and bone scan to check if there’s been any spread of the tumour beyond the prostate. With the information now available the cancer can be assigned a “stage”. Tumours are “staged” from T1 to T4 are there are sub-groups within these divisions. T1 is where the tumour is small, confined to the prostate and cannot be felt during a DRE. It will be picked up on biopsy. With T2 the tumour is confined to the prostate but can be felt. T3 means the tumour has spread from the prostate into areas such as the seminal vesicles and with T4 the tumour has spread into the pelvis and pelvic organs (bladder and rectum). Now armed with PSA test results (better if it’s a number of readings over several years), Gleason score, stage and scan outcomes, the patient and his doctor are in a position to look at the way ahead in terms of treating or managing the disease. Assuming the cancer is still confined to the prostate (localised disease) the treatment options include surgery (radical prostatectomy), external beam radiotherapy, brachytherapy (either low-dose [seeds] or highdose), androgen deprivation (hormone) therapy, active surveillance (watchful waiting) or a combination of some of these. Other options less often used are cryotherapy and HIFU (high-intensity focused ultrasound). 6 The PSA test has led to prostate cancers being detected earlier, meaning more are being diagnosed before the cancer has spread outside the prostatic capsule. For this reason more men who decide to have treatment are opting for surgery to remove the prostate (radical prostatectomy) and, hopefully, the tumour along with it. Traditionally open surgery has been used but laparoscopic and robot-assisted laparoscopic are becoming more common. Regardless of which method is used the surgeon will try to preserve the nerve bundles running alongside the prostate (nerve sparing radical prostatectomy) which affect continence and erectile functions however if there is significant tumour volume existing near or on the outer parts of the gland this may not be possible and some or all of the nerves may have to be sacrificed. The surgeon’s first priority will be preservation of life, then preservation of continence and then preservation of erectile function. Long-term, the outcomes from open versus robotic surgery are about the same. The overall cure rate for open surgery is around 80-85% at 15 years and it’s unlikely that this will be improved upon by the robotic assisted procedure. Compared to open, robotic surgery causes less blood loss, has a shorter hospital stay (often just overnight), a quicker return to general activities and shorter catheterisation and urinary recovery. However urinary function following either open or robotic surgery can be assisted by following a pelvic floor exercise regime (and losing weight if applicable) before and following the prostatectomy. Continued... Regardless of which method is used, the skill and experience of the surgeon is an important consideration. Recovery of erections may depend on a man’s age, general health and sexual function prior to surgery but can be helped along with the use of pharmaceuticals or other devices. If erectile dysfunction persists following surgery it’s best not to let too much time pass before seeking medical advice about the problem if this is causing relationship difficulties. The other mainstream treatment for prostate cancer is radiotherapy (radiation therapy). Radiotherapy uses various types of ionising radiation to treat the cancer. The ionising radiation damages a cell’s DNA causing irreversible damage which leads to cell death. The treatment aims to achieve maximum tumour cell kill with minimal damage to normal tissue. As normal tissue is better at repairing radiation damage than cancerous tissue, if the treatment doses are small enough the cancer cells can be eliminated. Consequently external beam radiotherapy, the most common form of radiotherapy for treating localised prostate cancer, is given in small doses (fractions), daily Monday to Friday, over a period of 7-8 weeks. Radiotherapy can be given externally (external beam radiotherapy or EBRT) or internally (brachytherapy). Whilst the aim of this treatment is to eliminate the prostate cancer, radiotherapy can also be used for palliative purposes in cases where the cancer has metastasised. External beam radiotherapy is delivered via a machine called a linear accelerator, a typical example of which is shown in the slide below. Unfortunately the radiation beams don’t just stop at the prostate. Other organs, the bladder, urethra and bowel, can be affected leading to both immediate and longterm side effects. The early side effects could include altered bowel and bladder function (urgency, diarrhoea, incontinence, frequency, pain and bleeding) but these mostly settle down once treatment is finished. However, in a few men, side effects remain with scar tissue (strictures) from radiation damage forming in the bowel, bladder and/or urethra and adding to the problems. In severe cases the bleeding problems (proctitis) could be treated with formalin (bowel) or hyperbaric oxygen therapy (bowel and bladder) or surgery to remove the strictures. In the past decade these side effects have been greatly reduced with the advent of image guided radiotherapy (IGRT) and intensity modulated radiotherapy (IMRT). Unfortunately the prostate is continuously on the move depending on the fullness or otherwise of the bladder, the amount of wind or solid matter in the bowel and pressure from other organs. IGRT is the placement of small markers (gold seeds or fiducial markers), normally three, within the prostate to ensure its location can be accurately assessed and the radiation beam appropriately aimed to avoid other organs. The three markers can be seen in the above slide. They are inserted in a procedure similar to a prostate biopsy. IMRT allows the intensity of the radiation beam to be altered. When the angle of the beam is such that it may affect organs other than the prostate the beam’s intensity is modulated so that the dose to normal tissue is reduced whilst the dose to the tumour can be increased when the beam is appropriately positioned. Results of long-term trials in Australia and overseas have shown that up to six months of hormone blockade (androgen deprivation or hormone therapy) used in conjunction with EBRT and beginning five months prior to EBRT greatly assists disease control and survival. Brachytherapy is a form of radiotherapy where the radiation is delivered to the prostate from an internal source. It can take two forms. Low dose (LDR) brachytherapy where radioactive “seeds” are permanently implanted in the prostate to kill the cancer cells and high dose (HDR) brachytherapy where hollow needles or catheters are temporarily placed into the prostate and a radioactive source is introduced through the needles. Once treatment is complete the catheters are removed. Advantages of brachytherapy are the ability to deliver a high dose of radiation directly to the tumour with minimal exposure to surrounding tissue and organs and, because of this, the dose of radiation can be higher than may be safe using EBRT. The procedures for inserting the “seeds” or the catheters are similar for both LDR and HDR. Diagram showing the position of the implant X-ray showing the position of the seeds in the prostate after the implant LDR is normally used for patients who have been diagnosed with prostate cancer in the low to moderate range or, for various reasons, may not be suitable for other treatments. Up to 80-100 radioactive “seeds”, each about the size of a small grain of rice, are implanted in the prostate through hollow needles which are inserted through the perineum and guided to their destination with ultrasound and other guidance systems. The operation is carried out under a general anaesthetic in a hospital operating theatre. Continued... 7 PROSTATE CANCER UPDATE Continued... Radiation emitted from the “seeds” decreases rapidly within a couple of millimetres from each “seed” and the positioning of the “seeds” can be planned prior to insertion to give most benefit in terms of killing tumour cells and not causing damage to other organs. The following slide shows a CT scan slice showing the implanted “seeds”. The procedure normally requires an overnight stay in hospital after which the patient returns home and the “seeds” get on with the job of eliminating the cancer cells. The patient is not radioactive (although bouncing grandchildren on your lap is not advised for a couple of months!) and the implants will gradually lose their radioactive potency over time with most gone in the first 10-13 weeks. Early side effects may include some tenderness and urinary symptoms such as pain on urinating, or urination difficulties if the prostate has swollen. Ejaculate may be discoloured from blood in the seminal fluid. Rectal complications are rare. These side effects will generally settle down. Erectile function will depend on a patient’s situation prior to the implantation but compares well to other procedures. Urethral strictures could be a problem in a small number of patients but these can be surgically corrected if the problem is severe. HDR may be used as a monotherapy but it’s mostly used in conjunction with EBRT to increase the dose of radiation without affecting surrounding organs. Normally about one-third of the radiation dose is delivered via HDR and the balance by EBRT. Because higher radiation doses (dose escalation) can be delivered it is often used for higher-risk cancers. The catheters are positioned in the prostate in a similar operation to the LDR procedure and are left in place for around 36 hours. During this time the catheters will be connected to an “afterloader” and a radioactive source will be briefly introduced into each one. The amount of radioactivity delivered to the prostate can be controlled by the time the radioactive source remains in the catheter. This process is repeated 3 times (3 is the norm but it could be less) at intervals over the next day and a half at which time the needles are removed and the patient can be discharged from the hospital. Side effects are similar to those of LDR although the chance of urethral strictures is slightly greater. Active surveillance or watchful waiting is a system for monitoring the tumour whilst not using any interventionist treatments. It’s a serious option for men with early, low-grade cancers, taking into account their expected life-span, co-morbidities and general health or who, for various reasons, may not want or be able to undergo a surgical procedure or radiotherapy. 8 Many prostate cancers are slow growing or even indolent and if they’re not causing any problems it may be a better option to leave them well alone rather than attempt to treat them and possibly suffer ongoing side effects. The cancer can be regularly monitored for change with PSA testing and a DRE and/or biopsy if it appears the tumour is growing and the man should be aware of the possible prostate cancer symptoms mentioned earlier. This won’t be for everyone. On discovering they have prostate cancer many men will seek the soonest possible curative treatment to rid themselves of the disease and give themselves peace-of-mind. For these men watchful waiting would be akin to what Dr Prem Rashid calls in his book “Your Guide to Prostate Cancer”, watchful worrying. As mentioned above, hormone therapy or androgen deprivation therapy (ADT) has proven to improve the results of radiotherapy when used prior to and during the start of the radiotherapy. Androgens are the male sex hormones, including the hormone testosterone. Prostate cancer “feeds” on testosterone and the cancer will shrink or even die in its absence. If a man is diagnosed with advanced or metastatic prostate cancer (it’s spread beyond the prostatic capsule into surrounding tissue, organs and bones), surgery is not going to be able to remove the tumour and radiotherapy, unless the tumour cells remain in the tissue immediately around and close to the prostate, will be similarly ineffective. Or if a man has had surgery or radiotherapy but has a rising PSA, it may indicate that some cancer cells may still be present. In these cases ADT can be used to weaken and shrink the cancer cells by reducing or eliminating a man’s testosterone production. This can be achieved via pharmaceuticals (taken orally or injected) known as chemical castration or by surgical castration (orchidectomy or removal of the testicles). The drugs can be used alone or in combination or used intermittently. Whilst men will react differently to these drugs they can extend life for many years. Unfortunately the withdrawal of testosterone does have an almost immediate downside. Tiredness, reduced libido, mood swings and hot flushes are some of the early side effects. Longer-term users may suffer from loss of mental function, erectile dysfunction, muscle weakening, osteoporosis and breast tenderness and possible enlargement. Some of these problems can be countered with exercise (physical and mental) and with other drugs and some men will experience other problems so it’s very much horses-for-courses. Regardless of diagnosis or treatment recommendations, make your own enquiries (a good place to start is with the sources listed on Page 2 of this magazine), get second or other opinions, talk to others who have been there (Prostate Cancer Support Groups can assist here) and don’t rush, prostate cancers are generally slow growing and a couple of months won’t alter your situation. RAY GIVES HIS LAST WEEKS TO OTHERS Story: Arthur Gorrie – GYMPIE TIMES 06AUG11 Photo: Renee Pilcher Ray Cheasley is the exception to many rules, giving an impression of effortless courage in the face of the end he knows is coming, probably before Christmas. He has dedicated his last months on earth to an unusual project to help others see the way forward when they are diagnosed with a terminal illness. He also wants to leave behind a real life story “for the grandkids,” and to help publicise the good work of Gympie’s Little Haven Palliative Care service. The video movie he will star in will show the positives of the inevitable end that waits for us all and he hopes it will help others deal with it when it happens to them. Friend Luke Mancell is making the movie, which will be entered in Gympie’s famous Heart of Gold Film Festival. There will also be a “director’s cut” version which will be his biography, something to leave behind “for the, grandkids”. He is determined not to spend his last months “moping around” and has agreed to be the “star” in a movie where he will have no trouble “acting naturally”. He hopes the final scene, in which he will die, will be videoed in his own bed. “I want to show the way for others,” he said yesterday. “I don’t know what’s ahead of me, because no-one talks about it. You’ve got no idea. Even now I know where I’ve been, but I don’t know where I’m going” Luke is open in his admiration for a man who wants to help others as he dies. “Ray will be a mentor for people following in his footsteps,” he said. Helping others is a focus that probably helps Ray cope as he deals with the prostate cancer which has got into his bones and blood. Radiation treatment, a torment in itself, has dealt with the outbreaks which occur from time to time. “Luke and I filmed the treatment and the doctor let us behind the scenes.” Ray was convenor and president of the Gympie and District Prostate Cancer Support Group. He even got to interview his doctor for the film. Now he is equally dedicated to helping people like Klara, the spouses of people facing inevitable death. “Little Haven does that too. They look after the patients but also help the family for as long as it takes” FOR THE RECORD: Luke Mancell filming Ray Cheasley, as he prepares for the inevitable and tries to help others. “I’ve got terminal cancer he said yesterday “They don’t know how long. They forecast November originally, but they don’t really know. “When someone tells you you’re, terminally ill it takes some sinking in. But at the end of the day I’m okay with it,” he said at the home he still lives in with the help of his wife Klara and the support of the Little Haven service. “It’s a long and lonely road for spouses too,” Klara said. “Then the penny dropped ,” Ray said, “and I realised how the partners suffer, so we started up a group for the partners of people with cancer. People suffer in different ways.” (Ray has been part of the Gympie & District Prostate Cancer Support Group since its inception in 2006. He was Treasurer for four years and Convener for one year prior to resigning because of ill health - Ed). PROSTATE CANCER RESEARCH AT THE MATER MEDICAL RESEARCH INSTITUTE During October Support Group members from Brisbane and the Gold Coast were given the opportunity to visit the Mater Medical Research Institute (MMRI) at South Brisbane to hear about and discuss their research work being carried out in relation to prostate cancer followed by a tour of their research laboratories. The visit was hosted by Assoc. Professor John Hooper from MMRI’s Cancer Cell Biology Laboratory. John Hooper, along with researchers from other laboratories within the complex, gave a brief overview of the work being carried out by the Institute within the various laboratories. Continued... 9 PROSTATE CANCER UPDATE Continued... Nutritionist, Dr Olivia Wright from the MMRI Nutrition Laboratory and who also lectures on nutrition and dietetics at the University of Queensland, spoke about adjunctive nutritional therapy in prostate cancer, its role during cancer treatment and the assistance it can offer with quality of life issues post-treatment or during ongoing treatment for those with advanced cancer. FOR THE RECORD: “Researchers & Support Group Members at MMRI, Dr Hooper is Sixth from the Right”. In Assoc. Professor Hooper’s Cancer Cell Biology Lab they are looking to understand the molecular drivers of aggressive prostate cancer, whether DNA changes drive aggressive tumours, why do these tumours spread to bones and how does prostate cancer survive in bone. Dr David Munster from the Therapeutic Antibodies Laboratory spoke about MMRI’s research into producing and testing improved therapeutic antibody drugs for prostate cancer. The antibodies would bind tumour antigens to the prostate cancer cells, causing the death of the cancer cells. The Cancer Immunotherapy Laboratory is researching cell-based dendritic cell immunotherapy and Dr Kristen Radford detailed the problems in producing a “one-size-fits-all” immunotherapy vaccine for prostate and other cancers. To do this it is necessary to better understand human dendritic cell biology. The laboratory’s goal is to make immunotherapy more efficacious, cost effective and adaptable to treat a wide range of cancer patients and a variety of malignancies. Following on from this, Assoc, Professor Nigel Waterhouse from the Apoptosis & Cytotoxicity Laboratory continued the immune theme by detailing work being carried out to understand how immune cells kill prostate cancer cells. Much of MMRI’s work relies on assistance from individual and corporate sponsorship, details of which can be found on the website listed on Page 2. Some of the research equipment in the MMRI laboratories has been purchased from grants given by Prostate Cancer Foundation of Australia. PRIDE OF AUSTRALIA The annual Pride of Australia awards, now in their seventh year, recognise the contribution of Australians who have gone beyond usual limits to support the community and other Australians. The awards are spread over ten categories; Courage, Care & Compassion, Fair Go, Young Leader, Inspiration, Child of Courage, Community Spirit, Outstanding Bravery, Heroism and Environment. The Community Spirit award recognises an individual or a group whose selfless, tireless and largely unacknowledged actions have enriched the lives of those around them in their community. The Convener of the Maryborough Prostate Cancer Support Group, Leoll Barron, was one of three Queensland finalists in the “Community Spirit” division of the 2011 awards. committees at the local golf club, junior cricket and touch football. After retiring as the well-respected principal of Maryborough High School in 2005, he has continued to share his expertise with associate teachers at the University of Southern Queensland. “After fighting off prostate cancer, he has initiated and organised Relay For Life events, raising more than $100,000 and has started a local support group for other prostate cancer sufferers. And he does all this while maintaining a cheery nature and an unwavering attitude to live life to the fullest.” Queensland Prostate Cancer News, and I’m sure all of our readers, congratulate Leoll on this wonderful achievement. The citation accompanying this honour reads; Leoll Barron “Leoll Barron is an unsung hero whose selfless community work has enriched the lives of many in the Maryborough region. He volunteers with countless sporting clubs, coaching roles and 10 NEWS ROUND UP Roche bone drug eases pain in prostate cancer trial (Reuters) – Roche’s bone strengthening drug “Boniva” is as good for pain relief as single dose radiotherapy in patients whose prostate cancer has spread to their bones, according to data from a late-stage trial. Trial investigators said the level of side effects of “Boniva”, known generically as ibandronate (IB), were also comparable with radiotherapy suggesting it could offer an alternative option for advanced cancer patients suffering pain. Bone metastases, or secondary tumours in the bone, are common in many advanced cancers and “are a serious problem for men with prostate cancer” said Peter Hoskin, a professor of clinical oncology at University College, London, who presented the data at the European Multidisciplinary Cancer Congress (EMCC) in Stockholm on 25SEP11. Distinct Prognosis for Gleason Scores 4 + 3 and 3 + 4 (HealthDay News) – A Gleason Score of 4 + 3 = 7 is correlated with pathological stage and increased risk of biochemical recurrence after radical prostatectomy (RP). Ali Amin from the Johns Hopkins Institutions in Baltimore and colleagues investigated whether the breakdown of Gleason Score 7 into 3 + 4 versus 4 + 3 has prognostic significance in predicting the pathological stage and biochemical progression. A total of 1,791 cases with Gleason Score 7 on prostatic biopsy identified between 2004 and 2010 were analysed. The study was published in the October 2011 issue of The Journal of Urology. Link Between High Blood Pressure and an Increased Risk of Developing or Dying from Cancer – Raised blood pressure is linked to a higher risk of developing cancer or dying from the disease according to the findings of the largest study to date to investigate the association between the two conditions. Dr Mieke Van Hemelrijck told the European Multidisciplinary Cancer Congress in Stockholm on 27SEP11 that there had been contradictory results from previous smaller studies investigating the link between cancer and blood pressure. However her study, which included 289,454 men and 288,345 women, showed that higher than normal blood pressure was statistically significantly associated with a 10-20% higher risk of developing cancer in men and a higher risk of dying from the disease in both men and women. ASTRO: Fewer Side Effects With IMRT for Prostate Cancer (HealthDay News) – Treatment of localised prostate cancer using intensity modulated radiation therapy (IMRT) is associated with a considerable reduction in late bowel and rectal side effects and significantly decreased rectal and bladder toxicity compared to three-dimensional conformal radiation therapy (3D-CRT), according to a study presented to the annual meeting of the American Society for Radiation Oncology held at Miami Beach 02-06OCT11. Vitamin E May Hike Risk of Prostate Cancer – Men receiving vitamin E supplements in a large randomised trial showed a slight but statistically significant increase in prostate cancer diagnoses, researchers said. After being followed up to 10 years after randomisation, the hazard ratio for prostate cancer in SELECT trial participants assigned to vitamin E supplements was 1.17 (95% CI 1.004 to 1.36) relative to the study’s placebo group, reported Eric A. Klein MD of the Cleveland Clinic, and colleagues. The four-arm trial also included selenium supplements, given alone or in combination with vitamin E. Participants in those groups showed a smaller increase in prostate cancer risk that failed to reach statistical significance, Klein and colleagues indicated in the 12OCT11 issue of the Journal of the American Medical Association. Married People More Likely to Survive Cancer 14OCT11 – Some people think that unattached blokes have it made. But being a lifelong bachelor may not be all it’s cracked up to be, at least when it comes to a man’s odds of surviving cancer. A man without a mate is 35% more likely to die from cancer as a man who wears a wedding ring, a new study reveals. Researchers tracked the number of cancer deaths for thirteen common cancers, including breast, prostate, malignant melanoma, colon and lung in more than 440,000 Norwegian men and women over a 40-year period from 1970 to 2007. Overall, single men and single women fared the worst in their cancer outcomes. Never-married men and women were found to have a greater risk of losing their life to the disease compared to those who had tied the knot, divorced, or were widowed. The study was published online in the journal BMC Public Health. Age a Big Factor in Prostate Cancer Deaths, Study Finds 19OCT11 (ScienceDaily) – Contrary to common belief, men aged 75 and older are diagnosed with late-stage and more aggressive prostate cancer and thus die from the disease more often than younger men, according to a University of Rochester analysis published online in the journal Cancer. The study is particularly relevant in light of the recent controversy about prostate cancer screening. Earlier this month a government health panel said that healthy men aged 50 and older should no longer be routinely tested for prostate cancer because the screening test in its current form does not save lives and sometimes leads to needless suffering and over-treatment. Measuring Quality of Life Important in Cancer Survival Research – Cancer survival studies should treat questions about how well people are surviving with the same importance as how long; putting quality of life on an equal footing with survival years, say researchers writing in a scientific journal this month. Effective and reliable quality of life measures offer increasingly valuable information for cancer patients and their doctors when they discuss treatment options, their potential consequences and the likely rehabilitation needs, write Drs Paul B. Jacobsen and Heather S. Jim, of the Department of Health Outcomes and Behavior at the Moffitt Cancer Center in Tampa, Florida, in the OCT11 issue of Cancer Epidemiology, Biomarkers and Prevention. Above Information Sourced from Cancer Daily News 11 PROSTATE CANCER FOUND IN 2,000 YEAR OLD EGYPTIAN MUMMY By Simon Tomlinson – 03NOV11 www.dailymail.co.uk were several post-mortem fractures, possibly produced when the mummy was transported to Europe. Scientists believe they have discovered the oldest case of prostate cancer in Egypt after scans on a 2,250-year-old mummy showed the man died a slow and painful death from the disease. But they also found a variety of tumors, measuring between 0.03inches and 0.59inches, interspersed along M1’s pelvis and lumbar spine. The unnamed Ptolemaic mummy, which is kept at the National Archaeology Museum of Lisbon, had a pattern of round and dense tumours between its pelvis and lumbar spine - giveaway signs of man’s modern-day killer. The mummy was that of a 5ft 5ins adult male who lived between 285 and 230 BC and was between 51 and 60 years old when he died, researchers said. �The bone lesions were considered very suggestive of metastatic prostate cancer,’ wrote the researchers in the International Journal of Paleopathology. They subjected the mummy, known as M1, to powerful Multi Detector Computerized Tomography (MDCT) scans, which produced �really unusual high quality images’, Carlos Prates, a radiologist at Imagens Médicas Integradas in Lisbon, told Discovery News. Digital X-rays showed that M1 had been buried with crossed arms - a common pose in Ptolemaic mummies, although in the New Kingdom it was often associated with royals. He was adorned with a cartonnage mask and bib, and boasted an elaborately painted shroud. Prostatic carcinoma begins in the walnut-sized prostate gland and typically spreads to the pelvic region, the lumbar spine, the upper arm and leg bones, and the ribs, ultimately reaching most of the skeleton. Dr Prates and colleagues considered other diseases as alternatives. But M1’s sex, age, the distribution pattern of the lesions, their shape and density, strongly argued for prostate cancer. �It is the oldest known case of prostate cancer in ancient Egypt and the second oldest case in history,’ Dr Prates said. The earliest diagnosis of metastasising prostate carcinoma came in 2007 when researchers investigated the skeleton of a 2,700-yearold Scythian king who died, aged 40 to 50, in the steppe of Southern Siberia, Russia. �This study shows that cancer did exist in antiquity, for sure in ancient Egypt. The main reason for the scarcity of examples found today might be the lower prevalence of carcinogens and the shorter life expectancy,’ Paula Veiga, a researcher in Egyptology, told Discovery News. Moreover, high-resolution CT scanners, able to detect tiny tumors became available only in 2005, which suggests earlier researchers may have missed them. The images showed he suffered from lumbosacral osteoarthritis, which was probably related to a lower lumbar scoliosis and there VACUUM ERECTION DEVICE AIDS RECOVERY AFTER SURGERY This study aimed to examine the effect of the early use of the vacuum erection device (VED) on erectile dysfunction (ED) and penile shortening after radical retropubic prostatectomy (RP) for prostate cancer. These devices fit over the penis and create a vacuum (by hand pumping) to encourage blood flow into the penis. A constriction ring prevents it from flowing out. 28 men who had nerves controlling erections spared during their surgery took part in the early (1 month after RP) group. Patients followed a daily rehabilitation program of 10 minutes/day using the VED with no constriction ring for 5 months. The control group used it starting 6 months after surgery. Both groups were evaluated for erectile function and length and girth of their penises after 9 months. 12 Erectile function scores were higher in the group with early use of the VED compared with the control group during the recovery period. Stretched penile length was significantly decreased in the control group at 3 and 6 months by approximately 2cm. By contrast, stretched penile length was preserved in the early intervention group at all sample times. The study authors conclude the use of a VED program 1 month after RP promotes return of sexual function and helps to preserve penile length. http://www.phoenix5.org/glossary/vacuum_erection_device.html 5 YEAR DATA: HYPOFRACTIONATED RADIATION FOR PROSTATE CANCER BLADDER TOXICITY A PROBLEM Nick Mulcahy September 26, 2011 — Hypofractionated radiation reduces the treatment time of prostate cancer by 2.5 weeks, compared with conventional radiation, but does not sacrifice efficacy, according to new 5-year data that will be presented at the upcoming annual meeting of the American Society for Radiation Oncology (ASTRO). However, persistent grade 2 or greater urinary adverse effects were significantly more common in patients treated with hypofractionated therapy at 5 years, according to the lead author Alan Pollack, MD, chair of radiation oncology at the University of Miami Miller School of Medicine in Florida. He spoke at press briefing held in advance of the meeting. When asked by Medscape Medical News if saving 2.5 weeks of treatment time was worth the potential risk of years of urinary problems for some men, Dr. Pollack replied that “there may be a trade-off with this particular regimen.” The rate of persistent urinary problems seen at 5 years in hypofractionation patients was “less than 10%,” compared with “less than 5%” for those treated with conventional radiation in the study, he said. The rate of late urinary problems was “still rather low” and “extremely favourable” in both study groups, compared with results from other radiotherapy studies, Dr. Pollack emphasized. The multicentre phase 3 trial of 303 men with intermediate- and highrisk prostate cancer compared a 5-week course of hypofractionated intensity-modulated radiotherapy (HIMRT) with a 7.5-week course of conventional intensity-modulated radiotherapy (CIMRT). The study hypothesis was that HIMRT would improve efficacy — the rate of prostate cancer biochemical failure — and not increase toxicities, compared with CIMRT. On both counts, the trial was not a success. The 5-year cumulative incidence rates of biochemical failure were similar — 14.4% for CIMRT (95% confidence interval [CI], 8.8% to 21.5%) and 13.9% for HIMRT (95% CI, 8.4% to 20.9%). Biochemical failure was defined as an increase in prostate-specific antigen (PSA) score using the nadir + 2 ng/mL definition. On the bright side, Dr. Pollock said that the long-term rates of bowel/ rectal adverse effects and erectile dysfunction were identical for the 2 radiation approaches. HIMRT is a work in progress, said Michael Steinberg, MD, ASTRO president elect, who moderated the press briefing. “We are learning more about how to do this and who this is best for,” explained Dr. Steinberg, who is from the University of California at Los Angeles Health System. HIMRT is likely to make its way into the treatment of prostate cancer. “We will see more places do this,” he said about hypofractionation, especially as these study results “get out there.” HIMRT represents a “change in how we were classically taught,” added Dr. Steinberg. The 5-year data are an update of results previously reported by Medscape Medical News, when the median follow-up was 39 months. Notably, there was no statistically significant difference in persistent urinary problems early in the study, said Dr. Pollack; the difference emerged only at the planned 5-year analysis. More Data The trial compared 76 Gy in conventional 2.0 Gy fractions (CIMRT) with 70.2 Gy in 2.7 Gy fractions (HIMRT), which was estimated to be equivalent to 84.4 Gy in 2.0 Gy fractions, said Dr. Pollack. The men received treatment from 2002 to 2006. No significant differences were seen between the treatment groups in terms of the distribution of patients by T-category, Gleason score, pretreatment initial PSA, use of androgen-deprivation therapy (ADT), or length of ADT, report Dr. Pollack and colleagues. There were 41 biochemical failures at 5 years — 20 in the CIMRT group and 21 in the HIMRT group. Six biochemical failures occurred within 6.5 months of either local-regional failure or distant metastasis. Rates for local-regional failure or distant metastasis were 1.0% for CIMRT and 1.3% for HIMRT at 5 years. The 5-year cumulative incidence rates for any failure, including 4 deaths, were 15.4% for CIMRT (95% CI, 9.5% to 22.7%) and 15.3% for HIMRT (95% CI, 9.5% to 22.4%). “The anticipated failure rate of 15% in the HIMRT arm was accurate, but fewer failures were seen in the CIMRT arm at the time of this planned analysis,” write Dr. Pollack and colleagues in the study abstract. Overall, there were no statistically significant differences in late toxicity between the groups, note the authors in the abstract. The grade 2 or higher toxicities for the CIMRT and HIMRT groups were 8.9% and 13.8% (P = .2), respectively, for the genitourinary tract, and 4.1% and 5.9% (P = .5), respectively, for the gastrointestinal tract. However, the genitourinary rates were for any event, including 1-time occurrences, said Dr. Pollack. The rates of persistent urinary problems were, as noted above, appreciably different for the 2 groups. American Society for Radiation Oncology (ASTRO) 53rd Annual Meeting: Abstract 1. Presented 03OCT11. 13 CANCER ETIQUETTE 79 Cancer Sucks... Cancer invaded my life many years ago. I’m not a personal victim of cancer but I feel I’ve been victimized witnessing the agony my loved ones have endured. I personally witnessed events and statements in their lives while they were fighting the beast. I feel compelled to share some common sense knowledge I’ve learned over the years. Possibly by me sharing this hub another cancer survivor or fighter won’t have to hear or deal with uncomfortable moments or questions. There are many people who never had to deal with cancer, to them it’s something that happens to others which is understandable. Those people might not know what to say or do when they hear someone is struggling to save their life. I hope this helps you learn what to say and what not to say when your encountered with an awkward situation. This is my opinion and the responses I’ve heard from victims over the last 11 years. Don’t ever, ever tell someone “You have the good cancer!” There is no such thing as a good cancer, cancer is cancer and all cancers are deadly but treatable if caught early. Early detection is of upmost importance but sometimes there are no symptoms. Either way there are NO GOOD CANCERS. Don’t be afraid to ask a cancer victim or their family member how they are feeling. How their treatments are going. Some people think they shouldn’t approach the subject because they don’t know if it’s the right time, there is no such thing as the right time...just ask...if they don’t want to discuss it they will tell you that. On the other hand, they might need to vent so ask only if you truly care and want to hear their response no matter how lengthy it might be. Don’t assume cancer is contagious and by discussing it you might catch it. That’s impossible but that question has been asked, oddly enough. Don’t say “You don’t look like you have cancer”! How is someone with cancer supposed to look? The monster is internally gnawing away at their organs, their hearts are heavy with sadness...that’s not always possible to see. Not all cancer patients are bed-ridden waiting to die. Medical technology has come a long way in treating cancer and victims can now live a lot longer and have more productive lives. Don’t say “I’ll pray for you” unless you truly intend to pray for them. Granted there are some people who keep a list of ones to pray for but I believe that most people say that because they feel it’s customary. If you intend to actually pray for that person then say it, if not something such as “I’ll be thinking of you”, “You’ll be in my thoughts” or “break a leg” will suffice. Don’t offer to chauffer a patient to an appointment or hold someone’s hand during a procedure unless you intend to. Many people out of the goodness of the hearts offer assistance and don’t come through when needed so please don’t offer and get their hopes up unless you are able to be there. Do call them. A phone call to say hello and share some memories or to simply talk about the weather are appreciated. Conversations don’t have to revolve around cancer. Trust me, patients want to forget they have the beast sometimes and escape into your world if even for a little while. 14 Don’t ignore them and assume by doing so there isn’t an issue. Cancer isn’t that easy to get rid of. Your loved one is ill and now is the time they need interaction from you. Your support is an important part of healthy healing. Without support a cancer victim might not have a purpose to fight as hard as they should. Do suggest to stop by for a visit, bring along a delicious cake and savour the moment. Your heart will be enlightened by your meaningful visit. Your loved one will cherish the time you spent together. Even if no words are spoken your presence alone could make their day. Do offer to cook a meal, mow the lawn, babysit the children etc... these deeds might seem small to you but will be huge in the mind of your loved one. Don’t preach to them...if they drink, smoke, eat a pizza...don’t tell them it’s unhealthy, don’t you think they already know that. It’s their bodies to do with what they please. We all make choices in life, show them the respect by allowing them to make theirs. Don’t suggest alternative forms of treatment, healthier lifestyles, vitamins or supplements...trust me they have been there and heard it and possibly tried it. That’s what their physician and Google are intended for. Do remember silence is deadly and so is cancer. One we have control over and one we don’t. Be the best you can be and show your support without being overly sympathetic which can actually make your loved one feel worse. Don’t forget humour is the best medicine. Laugh with them until you both can’t laugh anymore (and then laugh even more). Don’t ask “Are you cancer free now”? Ugh! There is no such thing as cancer free! We were all born with cancer cells in our bodies. These cells are inactive until they become active. So you get cancer when there are more factors that promote cancer growth than factors that inhibit cancer growth. It’s that simple. Added bonus: Do be your own advocate for your health. Doctors are human and they make mistakes. No one knows your body like you. Without thoroughly explaining all of your symptoms, no matter how trivial you think they might be, your physician won’t be able to effectively diagnose you. Keep in mind you made the choice to “hire” your physician for his abilities. So, unless you feel comfortable with his performance, you are free to speak your mind until you receive the answers that you are comfortable with. Disclaimer: I’m not judging anyone. I understand how it might be uncomfortable and you might be at a loss for words. I’m not a medical professional. I’m an advocate for victims of cancer. My terminology might offend someone and for that I apologize but my personal journey has brought me to this point. I lost my mother to a six-year battle with Colon Cancer. I’ve been by my husband’s side during his three-year battle with Prostate Cancer and the emotional roller coaster takes it’s toll at times. My heart goes out to all cancer fighters and their families. Be well, Anon. COMBINED ADJUVANT THERAPIES IMPROVE OUTCOME OF HIGH-RISK PROSTATE CANCER NEW YORK (Reuters Health) 12SEP11 - After radical prostatectomy for cancer involving the seminal vesicle, men fare best with adjuvant radiotherapy plus androgen deprivation therapy, a French study shows. Seminal vesicle invasion is associated with decreased survival, and radical prostatectomy alone is “probably insufficient” in this setting, note Dr. Cyrille Bastide, at Hopital Nord in Marseille, and colleagues in their report. Working with radical prostatectomy records on 4,090 patients from nine hospitals, they identified 310 with seminal vesicle involvement. After excluding men with lymph node metastases, detectable prostate specific antigen (PSA) after surgery, or less than 18 months’ follow-up, the research team had a study group of 199 patients. group, 48.4% in the ADT-only group, and 82.8% with combination therapy, according to a report in BJU International online August 18th. Estimated seven-year biochemical-failure-free survival rates in the four groups were 25.9%, 28.6%, 32.3% and 62.1%, respectively. Only the combination of radiotherapy and androgen deprivation was an independent prognostic factor, the team found. “The hazard ratio associated with adjuvant radiotherapy combined with hormonal therapy was 0.15 (p<0.001) for biochemical progression,” they calculated. Dr. Bastide and colleagues conclude, “The findings reported in the present study suggest that adjuvant ADT combined with radiotherapy after radical prostatectomy for patients with seminal vesicle invasion confers a substantial benefit.” Eighty-two men were monitored without further treatment, 41 received adjuvant radiotherapy alone, 26 received only androgen deprivation therapy (ADT), and 50 received ADT combined with radiotherapy. An editorial adds, “Continued investigation is needed to identify the accurate cohort of high risk prostate cancer patients at highest risk for cancer progression and therefore most likely to benefit from a multimodal treatment approach.” The estimated five-year survival rate free from biochemical failure was 32.6% in the monitored group, 44.4% in the radiotherapy-only British Journal of Urology International 2011. SURVEY FINDS GOOD LONG-TERM QOL AFTER PROSTATE CANCER BRACHYTHERAPY NEW YORK (Reuters Health) 08SEP11 - Long-term toxicity is low and quality of life (QOL) good or acceptable after low-dose rate brachytherapy for prostate cancer, UK researchers say. 20.7% had received hormones, brachytherapy, and external beam radiotherapy; and the remaining 2.3% received brachytherapy and external beam radiotherapy. Lead investigator Dr. Amr M. Emara from Royal Surrey County Hospital and colleagues sent questionnaires to 226 men whose cancer was successfully treated with low-dose brachytherapy (alone or with external beam radiotherapy and/or hormonal treatment) at least five years previously. Most of those who presented with mild or moderate urinary symptoms still had them at follow-up. Just under a third of men who started out with mild symptoms (31.2%) developed moderate symptoms, and 10.9% of men with moderate symptoms at baseline transitioned to severe symptoms. They received responses from 174 men (77%), according to a report August 19th in BJU International. More than a quarter (28.1%) of men with moderate baseline symptoms had only mild symptoms at follow-up, however. Just over a quarter (27.6%) had received brachytherapy alone; 49.4% had been treated with hormones and brachytherapy; Quality of life related to urinary symptoms was rated as good by 77%, acceptable by 21%, and poor by 2% of the survey respondents. Continued... 15 SURVEY FINDS GOOD LONG-TERM QOL AFTER PROSTATE CANCER BRACHYTHERAPY Continued... Of the 62 men who were potent before brachytherapy, 62.9% were still potent at follow-up, although the mean IIEF-5 score (a measure of erectile function) had worsened from 13.08 at baseline to 8.04. “The interpretation of data of bowel symptoms at follow-up is limited by the fact that we did not have baseline data available with which to make any comparison,” the investigators say. “The finding is more favourable than the potency outcomes reported in other studies,” the researchers note. They attribute the improvement to lower doses of brachytherapy to the penile bulb. “Overall, the results obtained in the present study confirm that brachytherapy has a favourable side effect profile over the longterm with regard to potency, urinary, and bowel toxicity,” the authors conclude. “Improvements in brachytherapy techniques should allow even better outcomes for patients treated with brachytherapy in the future,” they add. At follow-up, 51.7% of patients reported normal bowel function and 45.4% reported mild bowel symptoms. Only 2.9% had moderate symptoms, and none reported severe symptoms. British Journal of Urology 2011. Brisbane PCSG - 2011/12 meeting program - Cancer Council Queensland, 553 Gregory Terrace, Fortitude Valley. Evenings at 7.00am (Even months). Mornings at 9.30am (odd months) December 14 “Men’s Sheds - Graham Curnow, National President Men’s Sheds: Dermot Dorgon, Survivor: Christmas Function” January 11 TBA. Partners of Men with Prostate Cancer meet on the 4th Wednesday of each month between 6pm and 8pm at Cancer Council Queensland’s Gregory Terrace building. Members come together to share, learn and support each other in a warm open environment. Light refreshments are provided and there is parking underneath the building. For more information phone Karen Ward on (07) 3356 8106. Contact Details Queensland Prostate Cancer News Mail: PO Box 201, Spring Hill Qld 4004 Email: qpcn@cancerqld.org.au Phone: via Cancer Council Helpline 13 11 20 Prostate Cancer Foundation of Australia and Queensland Chapter Council Mail: (P.O. Box 10444) Adelaide Street, Brisbane, QLD 4000 Email: queensland@prostate.org.au Phone: 07 3166 2140. Disclaimer Council (ie. the Council of the Queensland Chapter) accepts no responsibility for information contained in this magazine. Whilst the information is presented in good faith, it may contain information beyond the knowledge of Council and therefore cannot be taken to be the opinion of Council. Important privacy information You have received this magazine because you have provided your contact details to Cancer Council Queensland or to a Prostate Cancer Support Group (PCSG). The primary purpose of collecting your contact details was to enable support, resources and information to be offered to you as a person affected by or interested in prostate cancer. Your contact details are held in th e local office of Cancer Council Queensland. Cancer Council Queensland ensures compliance with the Privacy Act, and does not use or disclose your details except as you might reasonably expect. You may access your details and you may request that we correct or amend (ie. update) or delete your details. 16 The information in this magazine is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read here. If you are a member of an affiliated PCSG you will initially receive by post or email your local group’s news-sheet, the monthly Queensland Prostate Cancer News (QPCN), and the national quarterly Prostate News. You may also receive other communications from time to time such as advice on upcoming symposia, news or surveys from research establishments, details of open clinical trials, and guidelines being reviewed. You may �opt-out’ of any of these services at any time, ie. you will no longer receive any material of that type, by letting us know your wishes. QPCN is available online at http://www.pcfa.org. au/qld/newsletter.htm. Should you receive multiple copies, please let us know which address(es) to remove from which mailing list(s).
© Copyright 2025 Paperzz