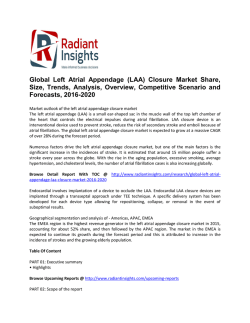
Delayed Administration of Human Umbilical Tissue-Derived Cells Improved Neurological Functional Recovery in a Rodent Model of Focal Ischemia Li Zhang, MD; Yi Li, MD; Chunling Zhang, MD; Michael Chopp, PhD; Anna Gosiewska, PhD; Klaudyne Hong, PhD Background and Purpose—The short time window required by neuroprotective strategies for successful treatment of patients with ischemic stroke precludes treatment for most. However, clinical therapies based on neuroregeneration might extend this therapeutic time window and thus address a significant unmet need. Human umbilical tissue-derived cells have shown great potential as neuroregenerative candidates for stroke treatment. Methods—The effectiveness of intravenous administration of human umbilical tissue-derived cells was tested in a rodent middle cerebral artery stroke model in a dose escalation study (doses tested: 3⫻105, 1⫻106, 3⫻x106, or 1⫻107 cells/injection) followed by a time-of-administration study (time after stroke: Day 1, Day 7, Day 30, and Day 90 at a dose of 5⫻106 cells/injection). Controls were phosphate-buffered saline injections and human bone marrow-derived mesenchymal stromal cell injections. Post-treatment outcome tools included the modified neurological severity score and the adhesive removal tests. Histology was performed on all cases to evaluate synaptogenesis, neurogenesis, angiogenesis, and cell apoptosis. Results—Statistically significant improvements of human umbilical tissue-derived cell treatment versus phosphatebuffered saline in modified neurological severity scores and adhesive test results were observed for doses ⱖ3⫻106 cells up to 30 days poststroke. At doses ⱖ3⫻106, histological evaluations confirmed enhanced synaptogenesis, vessel density, and reduced apoptosis in the ischemic boundary zone and increased proliferation of progenitor cells in the subventricular zone of human umbilical tissue-derived cell-treated animals versus phosphate-buffered saline controls. Conclusions—These results indicate effectiveness of intravenous administration of human umbilical tissue-derived cells in a rodent stroke model compared with phosphate-buffered saline control and warrant further investigation for possible use in humans. (Stroke. 2011;42:1437-1444.) Key Words: cerebral infarct 䡲 human umbilical cord 䡲 stroke recovery 䡲 synaptogenesis S troke is a leading cause of death and disability worldwide. Unfortunately, treatment of ischemic stroke remains 1 of the most challenging areas in medicine today. Over the last 20 years, cell-based therapies have emerged as a potential approach in the treatment of stroke.1–3 Transplantation of stem cells derived from fetal tissues as well as progenitor cells from bone marrow and human umbilical cord blood promoted neuronal survival, tissue repair, and, most importantly, recovery after experimental stroke.3– 6 However, limited stem and progenitor cell sources along with ethical and safety concerns associated with the use of embryonic stem cells have spurred significant interest in the search for alternative stem cell sources for stroke treatment. Human umbilical cord tissue contains stem cells and is a candidate source of cells for restorative therapy in stroke.7,8 Previous studies indicated that human umbilical tissue- derived cells (hUTC) secrete several neurotrophic factors such as brain-derived neurotrophic factor, fibroblast growth factor 2, and interleukin 6, all of which have the capacity to govern neurorestoration.9 –12 However, the efficacy of systemically-administered hUTC to restore brain function in rodent stroke models has not been evaluated. In the present study, we tested whether intravenous administration of hUTC improves neurological functional recovery in rats after stroke. The effect of hUTC was compared with that of human bone marrow-derived mesenchymal stromal cells (hMSCs), which, when administered intravenously, have been shown to improve functional outcomes in rats after stroke.13,14 Methods All experimental procedures were approved by the Institutional Animal Care and Use Committee of Henry Ford Hospital. All Received October 7, 2010; final revision received December 8, 2010; accepted December 23, 2010. From the Department of Neurology (L.Z., Y.L., C.Z., M.C.), Henry Ford Hospital, Detroit, MI; the Department of Physics (M.C.), Oakland University, Rochester, MI; and Advanced Technologies and Regenerative Medicine, LLC (A.G., K.H.), c/o Ethicon, Inc, Somerville, NJ. The online-only Data Supplement is available at http://stroke.ahajournals.org/cgi/content/full/STROKEAHA.110.593129/DC1. Correspondence to Michael Chopp, PhD, Henry Ford Hospital, 2799 W Grand Boulevard, Detroit, MI 48202. E-mail michael.chopp@gmail.com © 2011 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.110.593129 Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 1437 1438 Stroke May 2011 outcome measurements were performed by observers blinded to the treatments. Animal Model Male Wistar rats (n⫽8 per cohort) weighing 270 to 300 g were subjected to 2 hours transient focal ischemia.15 Briefly, rats were anesthetized with 3.5% isoflurane and maintained with 1.0% to 2.0% isoflurane in 70% N2O and 30% O2 using a face mask. Rectal temperature was maintained at 37°C throughout the surgical procedure using a feedback-regulated water heating system. The right common carotid artery, external carotid artery, and internal carotid artery were exposed. A 4-0 monofilament nylon suture (18.5 to 19.5 mm), determined by the animal weight, with its tip rounded by heating near a flame, was advanced from the external carotid artery into the lumen of the internal carotid artery until it blocked the origin of the middle cerebral artery (MCA). Two hours after MCA occlusion, animals were reanesthetized with isoflurane and reperfusion was achieved by withdrawal of the suture until the tip cleared the lumen of the internal carotid artery. Isolation and Preparation of hUTC and hMSCs Human umbilical tissue-derived cells were isolated and cultured as described elsewhere.16 These cells are derived from the umbilical cord of a single donor and do not exhibit key hematopoietic markers such as CD34. In addition, these cells express HLA-ABC but do not express HLA-DR, DP, DQ and do not express markers for antigenpresenting cells CD80 and CD86. Briefly, human umbilical cords were obtained with donor consent after live births from the National Disease Research Interchange (Philadelphia, PA). Tissues were minced and enzymatically digested in a cocktail of 50 U/mL collagenase containing 500 U/mL Dispase and 5 U/mL hyaluronidase (Sigma, St Louis, MO). After almost complete digestion, the cell suspension was passed through a 70-m filter and centrifuged at 350 g. The cell pellets were washed in Dulbecco minimal essential medium and seeded at 5000 cells/cm2 in T-flasks (Corning, Corning, NY) in Dulbecco minimal essential medium– high glucose, 15% (vol/vol) defined fetal bovine serum (HyClone, Logan, UT), -mercaptoethanol (Sigma)⫹100 U/mL penicillin, and 100 g/mL streptomycin (Invitrogen). Cells were expanded in culture under standard conditions in atmospheric oxygen with 5% carbon dioxide at 37°C. When cells reached approximately 70% confluence, they were passaged using trypsin/ethylenediaminetetraacetic acid (Gibco, Grand Island, NY) every 3 to 4 days and reseeded at a density of 5000 cells/cm2 onto gelatin-coated flasks. Cells were harvested after 10 passages (approximately 20 population doublings) and cryopreserved in growth medium containing 10% (vol/vol) dimethyl sulfoxide (Sigma) in a programmable rate freezer (Thermo Forma, Marietta, OH). Cells were stored in a unit maintaining a phase of nitrogen vapor with a small amount of liquid nitrogen at approximately ⫺120°C until thawing for cell characterization or for administration in the study. Cell viability was reconfirmed on thawing and only samples meeting viability requirements were injected into animals. Thawed cell samples were immunophenotyped before use to ensure similar immunophenotypes as reported elsewhere,16 and cells were characterized to ensure safety and identity. Identity was evaluated by flow cytometry for the expression of several cell surface markers. Antibodies were purchased from BD Biosciences (Franklin Lakes, NJ). Antibodies used in the analysis were IgG1-FITC, IgG-PE FITC, CD10, CD13, CD31, CD34, CD44, CD45, CD 73, CD117, CD141, HLA-DR, DP, DQ, HLA-ABC, and PDGF-Ra. Cell karyotype analysis was also performed to confirm that the cells contained the expected complement of human chromosomes. Cell pellets were evaluated by polymerase chain reaction for the presence of viral pathogens: HIV-1, HIV-2, cytomegalovirus, hepatitis B virus, hepatitis C virus, human T-lymphocytic virus, and Epstein-Barr virus. Cells were prepared for injection into the MCA-injured animals immediately before delivery. Cell vials were thawed in a 37°C water bath and then washed with phosphate-buffered saline (PBS). Aliquots of the cell suspension were removed and mixed with Trypan blue and counted with a hematocytometer. The cell concentration in the cell suspension was adjusted to the appropriate density with PBS (3⫻105, 1⫻106, 3⫻106, 5⫻106, or 1⫻107 in 2 mL PBS) for infusion. Human mesenchymal stem cells were cultured according to instructions provided by the supplier (Cambrex Corp, East Rutherford, NJ). Experimental Protocol Rats subjected to MCA occlusion were randomly allocated to the following groups. Dose Response Six groups of 8 animals each were included in the dose–response study. All treatments were performed intravenously in 2 mL PBS, 24 hours after MCA occlusion: Group 1, hUTC at 3⫻105 cells per injection; Group 2, hUTC at 1⫻106 cells per injection; Group 3, hUTC at 3⫻106 cells per injection; Group 4, hUTC at 1⫻107 cells per injection; Group 5, 2 mL of PBS control only; and Group 6, hMSC at 3⫻106 cells per injection. For identification of cell proliferation, rats received daily intraperitoneal injections of bromodeoxyuridine (BrdU, 100 mg/kg; Sigma), a thymidine analog, starting at 24 hours after stroke and subsequently for 14 consecutive days. All animals were euthanized at Day 60 poststroke. Timing of Administration Five groups of 8 animals each were included in this study based on the time of administration. Ideally, a PBS control group would have been needed for every time point evaluated. However, to limit as much as possible the number of animals euthanized in this study, the following experimental design was selected: Group 7, 5⫻106 hUTC cells administered on Day 1 poststroke; Group 8, 5⫻106 hUTC cells administered on Day 7 poststroke; Group 9, 5⫻106 hUTC cells administered on Day 30 poststroke; Group 10, 5⫻106 hUTC cells administered on Day 90 poststroke; and Group 11, 2 mL of PBS only administered on Day 30 poststroke, which served as a control group. Functional Outcome Modified Neurological Severity Score The modified neurological severity score is a composite of motor, sensory, reflex, and balance tests.17 Neurological function was graded on a scale of 0 to 18 (normal score, 0; maximal deficit score, 18). Animals were tested weekly for up to 60 days and biweekly thereafter. Adhesive Removal Test An adhesive removal test was used to measure somatosensory deficits.18 The mean time (seconds) required to remove stimuli from the left limb was recorded. Animals were tested 1 day before MCA occlusion and weekly thereafter starting 1 day after stroke onset. To increase the sensitivity of the test, rats were challenged with half-sized stimuli starting 70 days after stroke onset. The half-sized stimuli tests were conducted biweekly thereafter. Measurements of Infarct Volume Rats were euthanized 60 (dose–response study) or 140 days (timing of administration study) after stroke. Infarct volume was measured on 7 hematoxylin and eosin-stained coronal sections using a Global Laboratory Image analysis program (Data Translation, Marlboro, MA), as previously described.19 The infarct volume is presented as a percentage of total contralateral hemisphere volume.19 Immunohistochemistry Immunohistochemical studies were performed on coronal sections corresponding to bregma ⫺1.0 to 1.0 mm obtained from each experimental animal. To identify proliferating cells, monoclonal antibody against BrdU (Dako) was used at a titer of 1:100. Double stainings were performed to visualize cellular colocalization of BrdU with neuron-specific marker NeuN (Chemicon) at a dilution of 1:500 and with glial fibrillary acidic protein (Dako), an astrocyte marker at a dilution of 1:10 000. For a morphological analysis of vessels, a Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 Zhang et al polyclonal antibody against Von Willebrand factor (vWF; Dako) was used at a titer of 1:400. To detect presynaptic plasticity and synaptogenesis, a monoclonal antibody against synaptophysin (Chemicon) was used at a titer of 1:500. To detect human cells, a monoclonal antibody against human mitochondria (HM; Chemicon) was used at a titer of 1:100. To detect neuroblasts, a polyclonal antibody against doublecortin (DCX; Santa Cruz) was used at a titer of 1:200. For single labeling of BrdU, vWF, synaptophysin, HM, and DCX, adjacent sections were incubated with the primary antibodies at 4°C. Sections were sequentially incubated with the appropriate biotinylated secondary antibodies (goat antimouse IgG for BrdU, synaptophysin, and HM; goat antirabbit IgG for vWF; and horse antigoat IgG for DCX). The signal was detected by avidin– biotin complex (Vector Laboratories) before staining with diaminobenzidine and hydrogen peroxide. Double immunofluorescent labeling of BrdU with NeuN and BrdU with glial fibrillary acidic protein were done in sections that were incubated with secondary antibodies conjugated with fluorescein isothiocyanate (Calbiochem) or cyanine (Jackson Immunoresearch). The terminal deoxynucleotidyl transferase–mediated dUTP-biotinic end labeling method (in situ Apoptosis Detection Kit; Chemicon) was used to assess apoptotic cells according to the procedures provided by the manufacturer. The adult subventricular zone (SVZ) contains self-renewing multipotent neural progenitors, which are capable of generating all 3 neural lineages.20 –22 To examine whether administration of hUTC enhanced endogenous neurogenesis, proliferated SVZ cells identified by BrdU-positive cells and neuroblasts detected by DCXimmunoreactive cells were measured at 60 days after stroke onset. The numbers of BrdU-immunoreactive cells within the ipsilateral lateral ventricle wall were counted from each rat and divided by the ipsilateral lateral ventricle wall area to determine the cell density. The DCX-immunoreactive area within the ipsilateral lateral ventricle wall was measured and presented as percentage of area. Synaptic plasticity in the ischemic penumbra region contributes to functional recovery after stroke.23 To examine whether administration of hUTC enhanced synaptogenesis, synaptophysin immunoreactivity was measured 60 days after stroke onset. Specifically, 8 fields of view from the ischemic boundary zone were digitized using a 40⫻ objective from a MicroComputer Imaging Device (Imaging Research, St Catherines, Canada) system. The numbers of vWFimmunoreactive vessels and the positive area of synaptophysin in the ischemic boundary zone were measured throughout each field of view. Data are presented as density of vWF-immunoreactive vessels and percentage of synaptophysin-immunoreactive areas, respectively. To quantify apoptotic cells and human cells, numbers of terminal deoxynucleotidyl transferase–mediated dUTP-biotinic end labeling- and HM-positive cells throughout the ipsilateral hemisphere were counted. Data are presented as the total number of ipsilateral terminal deoxynucleotidyl transferase–mediated dUTPbiotinic end labeling- and HM-positive cells per section. Statistical Analyses Behavioral data were evaluated for normality and the nonparametric analysis was considered if data did not follow a normal distribution. A 1-way analysis of variance was conducted to test the treatment effect on each outcome between the control and all dose groups at each time point. Histology data were evaluated using Student t test. A treatment effect was detected if probability value was ⬍0.05. Results A total of 97 animals underwent MCA occlusion, of which 9 died before completion of the study and were therefore excluded from the analyses. Of these 9 animals, 6 died immediately poststroke and were not subjected to treatment. Two animals died at Day 8 poststroke from Group 2– dose– response study (treated with hUTC at a dose of 1⫻106 cells/injection) and 1 at Day 38 post stroke from Group 6 – dose–response study (treated with hMSC at a dose of Effectiveness of hUTC in a Rodent Stroke Model 1439 3⫻106 cells/injections). All animals that died during the study were replaced such that the final count of animals per group was 8. Neurological Functional Recovery The dose–response study indicated that treatment with hUTC at doses of 3⫻106 and 1⫻107 cells/injection, but not at doses of 3⫻105 and 1⫻106 cells/injection, significantly improved the performance on adhesive removal test and modified neurological severity score compared with the PBS-treated rats starting at Day 14. This statistically significant difference persisted up to Day 60 poststroke. Treatment with hMSC exhibited a similar effect on neurological functional improvement as compared with hUTC at doses of 3⫻106 and 1⫻107 cells/injection (Figure 1). The time of administration study indicated that hUTC administered 1 day after stroke onset significantly improved neurological function as measured by adhesive removal test and modified neurological severity score as compared with PBS treatment. This statistical significance was first seen at Day 7 and was maintained up to day 140 poststroke. Administration of hUTC at Day 7 or 30 significantly improved the performance on modified neurological severity score starting at Days 28 and 70, respectively, as compared with treatment with PBS. This statistical difference was maintained up to Day 140 poststroke. In addition, significant improvements on adhesive removal test were detected in rats treated with hUTC at Day 7 or 30, starting from Day 49 through 140, compared with PBS-treated rats. Administration of hUTC on Day 90 poststroke significantly improved performance on the adhesive removal test as observed on Day 140 but failed to improve the modified neurological severity score score compared with PBS-treated rats. Our data thus indicate that delayed administration of hUTC up to 30 days improved neurological functional recovery (Figure 1). Infarct Volume No significant reduction of infarct volume was detected in rats treated with hUTC regardless of dose and time of administration when compared with rats treated with PBS. In addition, treatment with hMSC did not significantly reduce the lesion volume compared with PBS-treated rats (Table). Detection of Human Cells Few HM-immunoreactive cells were detected within the ipsilateral hemisphere of rats treated either with hUTC or hMSC. Specifically, HM-positive cells ranged from 1.4⫾0.9 to 2.9⫾1.6 cells/section in hUTC-treated animals, with no correlation to dose, and reached 2.9⫾1.5 cells/section in hMSC-treated animals. The number of HM-immunoreactive cells did not differ between the experimental groups. No HM-immunoreactive human cells were found in PBS-treated rats 90 days after stroke. SVZ Cell Proliferation Treatment with hMSC and with hUTC at doses of 3⫻106 and 1⫻107 cells/injection but not at doses of 3⫻105 and 1⫻106 cells/injection significantly increased the number of ipsilat- Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 1440 Stroke May 2011 Figure 1. Adhesive removal test and modified neurological severity score for all groups up to 60 days poststroke for the dose–response study and 140 days poststroke for the time-of-administration study. All animals in the dose–response study were treated on Day 1 at doses indicated on the graph. Animals in the hUTC groups of the time-of-administration study were treated with 5⫻106 cells/injection at times indicated on the graph. Before the stroke, there was no significant difference in neurological function measured by adhesive removal test, as indicated on A, C, and modified neurological severity scores for normal, preischemic rats were equal to 0⫾0 for all animals (not shown on graphs). A, Adhesive removal test of rats in the dose– response study; (B) modified neurological severity score of rats in the dose–response study; (C) adhesive removal test of rats in the time-of-administration study; and (D) modified neurological severity score of rats in the time-of-administration study. *P⬍0.05 as compared with the phosphate-buffered saline-treated group. hUTC indicates human umbilical tissue-derived cells. eral BrdU-immunoreactive cells in the SVZ compared with PBS-treated rats. Treatment with hUTC thus dosedependently increased SVZ cell proliferation in rats after stroke (Figure 2A–B). In addition, treatment with hUTC at a dose of 3⫻106 cells/injection significantly increased the DCX-immunoreactive area in the ipsilateral SVZ (Figure 2C–D) compared with that of PBS-treated rats when the treatment was initiated at 24 hours after stroke onset, indicating that hUTC treatment enhanced neuroblast concentration in the ischemic brain. Double-staining immunohistochemistry revealed that fewer than 5% of BrdU-positive cells were reactive for NeuN and glial fibrillary acidic protein across groups. Treatment with hUTC at doses of 3⫻106 did not significantly increase Table. the proportion of BrdU/NeuN (2.7%⫾0.5% versus 2.1%⫾0.5%) or BrdU/glial fibrillary acidic protein (3.3%⫾0.5% versus 4.1%⫾0.8%) double-labeled cells compared with PBS-treated rats 60 days after stroke onset. Treatments and Lesion Volumes for All Groups Treatments Lesion Volume (% of Contralateral Hemisphere) Group 1 hUTC at 3⫻105 at Day 1 after MCA 34.9⫾2.2 Group 2 hUTC at 1⫻106 at Day 1 after MCA 34.3⫾2.3 Groups (n⫽8/Group) 6 Group 3 hUTC at 3⫻10 at Day 1 after MCA Group 4 hUTC at 1⫻107 at Day 1 after MCA 33.8⫾2.1 Group 5 PBS at Day 1 after MCA 34.9⫾2.6 Group 6 hMSC at 3⫻106 at Day 1 after MCA 34.6⫾2.2 6 33.2⫾1.9 Group 7 hUTC at 5⫻10 at Day 1 after MCA 31.3⫾2.6 Group 8 hUTC at 5⫻106 at Day 7 after MCA 33.0⫾2.4 Group 9 hUTC at 5⫻106 at Day 30 after MCA 31.3⫾2.1 Group 10 hUTC at 5⫻106 at Day 90 after MCA 34.0⫾2.5 Group 11 PBS at Day 30 after MCA 33.0⫾2.4 hUTC indicates human umbilical tissue-derived cells; MCA, middle cerebral artery; hMSC, human bone marrow-derived mesenchymal stromal cells; PBS, phosphate-buffered saline. Figure 2. A, Representative micrographs showing BrdU immunoreactivity at the ipsilateral SVZ acquired from rats treated with PBS (top panel) and hUTC at a dose of 3⫻106 cells (bottom panel); (B) quantitative analysis of BrdU-positive cell density (number of cells/ mm2) in the ipsilateral and contralateral ventricle walls; (C) representative micrographs of DCX immunoreactivity at ipsilateral hemispheres from rats treated with PBS (left panel) and hUTC at a dose of 3⫻106 cells (right panel); (D) quantitative analysis of DCX expression in the SVZ. Bars⫽50 m. *P⬍0.05 as compared with the PBS-treated group. BrdU indicates bromodeoxyuridine; SVZ, subventricular zone; PBS, phosphate-buffered saline; hUTC, human umbilical tissue-derived cells; DCX, doublecortin. Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 Zhang et al Effectiveness of hUTC in a Rodent Stroke Model 1441 Figure 3. A, B, Micrographs of synaptophysin immunoreactivity in representative rats treated with PBS (A) or hUTC at a dose of 3⫻106 cells (B); (C) quantitative analysis of synaptophysin expression in the ischemic boundary zone of rats from the dose-escalation study. The amount of synaptophysin is expressed as percentage area coverage vs overall area. Bar⫽100 m. *P⬍0.05 as compared with the PBS-treated group. PBS indicates phosphate-buffered saline; hUTC, human umbilical tissue-derived cells. Synaptogenesis Administration of hUTC at doses of 3⫻106 and 1⫻107 cells/injection, but not at the lower doses of 3⫻105 and 1⫻106 cells/injection, as well as treatment with hMSC significantly increased synaptophysin expression in the ischemic boundary area compared with that observed in animals treated with PBS (Figure 3). Vascular Density at the Ischemic Boundary Zone Treatment with hUTC at doses of 3⫻106 and 1⫻107 cells/ injection, but not at the lower doses of 3⫻105 and 1⫻106 cells/injection, as well as treatment with hMSC significantly increased vWF-immunoreactive vascular density in the ischemic boundary area compared with that observed in PBStreated rats at 60 days after stroke onset (Figure 4). Apoptotic Cell Death Scattered terminal deoxynucleotidyl transferase–mediated dUTP-biotinic end labeling-positive cells were present throughout the ipsilateral hemisphere. These cells were primarily located in the ischemic boundary area 60 days after stroke onset. Treatment with hUTC at doses of 3⫻106 and 1⫻107, but not at the lower doses of 3⫻105 and 1⫻106, as well as treatment with hMSC significantly reduced the number of terminal deoxynucleotidyl transferase–mediated dUTP-biotinic end labeling-positive cells compared with that observed in PBS-treated rats. Treatment with hUTC thus reduced apoptotic cell death in a dose-dependent manner (Figure 5). Discussion Intravenous administration of hUTC in a rodent MCA model 24 hours after stroke dose-dependently promoted neurological functional recovery, which persisted at least 2 months after stroke onset. Significant functional recovery was also observed when treatment was initiated at Day 7 or 30 but not at Day 90 after stroke onset. Treatment with hUTC enhanced SVZ cell proliferation, synaptogenesis, and vessel density and reduced apoptotic cell death in the ischemic boundary area, which likely contributed to the improvement of neurological functional recovery in rats after stroke. Prior research indicates that intracerebral implantation of human umbilical cord-derived mesenchymal stem cells at 2 weeks after stroke onset reduces ischemic brain damage and neurological functional deficits in rats, indicating a neuroprotective effect of these cells in experimental stroke.7 In the present study, intravenous administration of hUTC improved neurological function recovery without the reduction of lesion volume compared with PBS-treated rats, thus suggesting that the improvement of neurological function observed here was derived from neurorestorative effects in the ischemic boundary area, resulting in neurogenesis, synaptogenesis, and angiogenesis. These regenerative processes have previously been shown to contribute to the functional recovery after ischemic insult.24 –27 Neurogenesis is initiated with neural progenitor cell proliferation after stroke.28 Treatment with hUTC significantly increased the number of BrdUincorporating cells and the DCX-immunoreactive area in the ipsilateral SVZ suggesting that hUTC treatment enhanced Figure 4. A, B, Micrographs of vWF immunoreactivity at ischemic boundary zone (IBZ) acquired from representative rats treated with PBS (A) or hUTC at a dose of 3⫻106 cells (B); (C) quantitative data of vWF-positive vessel density in the IBZ of rats from the dose-escalation study. Bar⫽50 m. *P⬍0.05 as compared with the PBS-treated group. vWF indicates von Willebrand factor; PBS, phosphate-buffered saline; hUTC, human umbilical tissue-derived cells. Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 1442 Stroke May 2011 Figure 5. A, B, Micrographs of terminal deoxynucleotidyl transferase–mediated dUTP-biotinic end labeling (TUNEL) staining at the ischemic boundary zone (IBZ) acquired from representative rats treated with PBS (A) or hUTC at a dose of 3⫻106 cells (B); (C) quantitative analysis of the density of TUNEL-positive cells (absolute number of cells per section) in the IBZ of rats from the dose-escalation study. Bar⫽50 m. *P⬍0.05 as compared with the PBS-treated group. PBS indicates phosphatebuffered saline; hUTC, human umbilical tissuederived cells. endogenous neurogenesis. Neuronal differentiation was further evaluated here by the presence, albeit in small number, of BrdU-immunoreactive cells that also coexpressed NeuN, a neuronal marker. In our study, there was no difference in BrdU–NeuN coexpression results between hUTC- versus PBS-treated animals. This may be due to the fact that the BrdU pulse labeling methodology used here only allowed detection of cell proliferation within the first 2 weeks poststroke and thus did not detect neuronal differentiation at later stages. Based on these results, and despite the positive DCX results, the effect of hUTC on neuronal differentiation remains to be determined. Therefore, the data associating neurogenesis with functional recovery should be interpreted with caution. In the present study, treatment with hUTC increased synaptophysin immunoreactivity at the ischemic boundary area, suggesting that hUTC treatment enhanced synaptogenesis. As for angiogenesis, a physiological repair process that naturally occurs in the ischemic brain,29 the increased vWF-immunoreactive vessel density in the rats treated with hUTC indicated that hUTC modulated the vascular system. Collectively, our data therefore indicated that intravenous administration of hUTC promoted endogenous neural progenitor proliferation, synaptogenesis, and increased vessel density, which may explain how hUTC also improved functional outcomes in the rats. Although multiple prior studies have reported that implantation of exogenous stem/progenitor cells from multiple sources can enhance neurogenesis, synaptogenesis, and angiogenesis,13,25,30 –32 our study is the first to suggest a similar outcome after intravenous administration of hUTC. Apoptotic cell death has been identified in normal brain throughout life and plays a critical role in maintaining tissue homeostasis.33,34 Apoptosis is a common feature in neurogenic regions during development and in the adult brain, in which the steady production of newly generated cells is largely eliminated through an apoptotic mechanism.33 We have previously demonstrated that stroke-induced apoptotic cell death peaked at 1 to 2 days poststroke and persisted for at least 4 weeks after stroke onset.35 In the present study, hUTC treatment was associated with reduced apoptotic cell death at 2 months after stroke onset compared with controls, suggesting that hUTC treatment not only enhances SVZ cell proliferation, but also reduces the apoptotic cell death in the damaged brain tissue. Prior research has shown that, although endogenous neurogenesis occurs in response to ischemic injury, the majority (approximately 80%) of newly generated cells die after stroke, indicating that apoptosis contributes significantly to the fate of newly generated cells.31,36 Thus, it is reasonable to speculate that by reducing apoptotic cell death, hUTC treatment may improve the survival of newly generated cells, an effect that might be linked to the functional recovery observed in the animals after the stroke. The effects of intravenous hUTC treatment on the survival of newly generated cells after stroke warrant further investigation. Previous studies have indicated that hMSCs are multipotent cells that, when implanted directly into the ischemic rat brain, can integrate into the parenchymal brain tissue and express neuronal markers 3 weeks after intracerebral transplantation.7,37 However, in the present study and after intravenous administration of hUTC, few human cells were detected in the ischemic brain 2 months after treatment, suggesting that cells were eliminated from the host brain over time. In support of this hypothesis is the fact that hUTC were previously shown to elicit a host tissue immune response, especially under inflammatory conditions.38 Stroke triggers an inflammatory response, which contributes significantly to the progression of brain damage.39 Thus, it is possible that transplanted cells were scavenged by the host immune system. In the hemiparkinsonian rats, the engrafted human umbilical cord matrix cells disappeared 6 weeks after transplantation, which is consistent with our finding.7,37 Therefore, although hMSCs have the potential to differentiate into parenchymal cells, the limited number of human cells observed in the present study suggests that neural transdifferentiation and fusion are unlikely the predominant mechanisms of action of intravenous administration of hUTC in stroke. Considering that functional recovery was observed in our study, along with angiogenesis, synaptogenesis, and reduction of apoptotic cell death, it can be hypothesized that the mechanism of action of intravenous hUTC administration is linked to expression of neurotrophic factors from the cells. The hUTC secrete several neurotrophic factors such as brain-derived neurotrophic factor and fibroblast growth factor Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 Zhang et al 2, all of which have the capacity to induce neurogenesis, angiogenesis, and synaptogenesis after stroke.40,41 In addition, the antiapoptotic signaling pathway is activated by neurotrophic factors.42 Thus, although not investigated directly here, the enhancement of host brain plasticity and suppression of apoptosis observed in the present study are likely attributable to the paracrine neurotrophic action of hUTC. This hypothesis is supported by others who showed that administration of hMSCs increased neurotrophic factor expression, which in turn is known to augment host brain plasticity and reduce apoptotic cell death in the experimental stroke.14 Effectiveness of hUTC in a Rodent Stroke Model 10. 11. 12. 13. 14. Summary The intravenous administration of hUTC augmented endogenous neurorestorative responses and neurological functional recovery with a time of administration window up to 30 days after stroke onset in the rat MCA occlusion model. Intravenous administration of hUTC thus represents a novel treatment for further evaluation with a potential broad time of administration window after the treatment of stroke. Acknowledgments We acknowledge Yisheng Cui, MD, Hongqi Xin, PhD, and Qi Gao, PharmD, employees at Henry Ford Hospital; and Michael Romanko, PhD, Brian Kramer, PhD, and Anthony Kihm, PhD, employees at ATRM, for technical, editorial, and logistical support during the conduct of this study. 15. 16. 17. 18. 19. 20. Sources of Funding The research presented here was funded by Advanced Technologies and Regenerative Medicine, LLC. 21. 22. Disclosures K.H., Stroke Team Leader, and A.G., Senior Director of R&D, are both employees of ATRM. 23. References 24. 1. McKay R. Stem cells in the central nervous system. Science. 1997;276: 66 –71. 2. Zhao LR, Duan WM, Reyes M, Keene CD, Verfaillie CM, Low WC. Human bone marrow stem cells exhibit neural phenotypes and ameliorate neurological deficits after grafting into the ischemic brain of rats. Exp Neurol. 2002;174:11–20. 3. Grabowski M, Brundin P, Johansson BB. Functional integration of cortical grafts placed in brain infarcts of rats. Ann Neurol. 1993;34: 362–368. 4. Savitz SI, Rosenbaum DM, Dinsmore JH, Wechsler LR, Caplan LR. Cell transplantation for stroke. Ann Neurol. 2002;52:266 –275. 5. Chen J, Sanberg PR, Li Y, Wang L, Lu M, Willing AE, Sanchez-Ramos J, Chopp M. Intravenous administration of human umbilical cord blood reduces behavioral deficits after stroke in rats. Stroke. 2001;32: 2682–2688. 6. Li Y, Chen J, Wang L, Lu M, Chopp M. Treatment of stroke in rat with intracarotid administration of marrow stromal cells. Neurology. 2001;56: 1666 –1672. 7. Koh SH, Kim KS, Choi MR, Jung KH, Park KS, Chai YG, Roh W, Hwang SJ, Ko HJ, Huh YM, Kim HT, Kim SH. Implantation of human umbilical cord-derived mesenchymal stem cells as a neuroprotective therapy for ischemic stroke in rats. Brain Res. 2008;1229:233–248. 8. Secco M, Moreira YB, Zucconi E, Vieira NM, Jazedje T, Muotri AR, Okamoto OK, Verjovski-Almeida S, Zatz M. Gene expression profile of mesenchymal stem cells from paired umbilical cord units: cord is different from blood. Stem Cell Rev Rep. 2009;5:387– 401. 9. Ferrer I, Krupinski J, Goutan E, Marti E, Ambrosio S, Arenas E. Brainderived neurotrophic factor reduces cortical cell death by ischemia after 25. 26. 27. 28. 29. 30. 31. 32. 1443 middle cerebral artery occlusion in the rat. Acta Neuropathol. 2001;101: 229 –238. Gorski JA, Zeiler SR, Tamowski S, Jones KR. Brain-derived neurotrophic factor is required for the maintenance of cortical dendrites. J Neurosci. 2003;23:6856 – 6865. Matsuoka N, Nozaki K, Takagi Y, Nishimura M, Hayashi J, Miyatake S, Hashimoto N. Adenovirus-mediated gene transfer of fibroblast growth factor-2 increases BrdU-positive cells after forebrain ischemia in gerbils. Stroke. 2003;34:1519 –1525. Islam O, Gong X, Rose-John S, Heese K. Interleukin-6 and neural stem cells: more than gliogenesis. Mol Biol Cell. 2009;20:188 –199. Chen J, Zhang ZG, Li Y, Wang L, Xu YX, Gautam SC, Lu M, Zhu Z, Chopp M. Intravenous administration of human bone marrow stromal cells induces angiogenesis in the ischemic boundary zone after stroke in rats. Circ Res. 2003;92:692– 699. Li Y, Chen J, Chen XG, Wang L, Gautam SC, Xu YX, Katakowski M, Zhang LJ, Lu M, Janakiraman N, Chopp M. Human marrow stromal cell therapy for stroke in rat: neurotrophins and functional recovery. Neurology. 2002;59:514 –523. Chen H, Chopp M, Zhang ZG, Garcia JH. The effect of hypothermia on transient middle cerebral artery occlusion in the rat. J Cereb Blood Flow Metab. 1992;12:621– 628. Lund RD, Wang S, Lu B, Girman S, Holmes T, Sauve Y, Messina DJ, Harris IR, Kihm AJ, Harmon AM, Chin FY, Gosiewska A, Mistry SK. Cells isolated from umbilical cord tissue rescue photoreceptors and visual functions in a rodent model of retinal disease. Stem Cells. 2007;25: 602– 611. Chen J, Li Y, Wang L, Zhang Z, Lu D, Lu M, Chopp M. Therapeutic benefit of intravenous administration of bone marrow stromal cells after cerebral ischemia in rats. Stroke. 2001;32:1005–1011. Schallert T, Kozlowski DA, Humm JL, Cocke RR. Use-dependent structural events in recovery of function. Adv Neurol. 1997;73:229 –238. Zhang RL, Chopp M, Zhang ZG, Jiang Q, Ewing JR. A rat model of embolic focal cerebral ischemia. Brain Res. 1997;766:83–92. Palmer TD, Markakis EA, Willhoite AR, Safar F, Gage FH. Fibroblast growth factor-2 activates a latent neurogenic program in neural stem cells from diverse regions of the adult CNS. J Neurosci. 1999;19:8487– 8497. Anderson DJ. Stem cells and pattern formation in the nervous system: the possible versus the actual. Neuron. 2001;30:19 –35. Doetsch F, Caille I, Lim DA, Garcia-Verdugo JM, Alvarez-Buylla A. Subventricular zone astrocytes are neural stem cells in the adult mammalian brain. Cell. 1999;97:703–716. Stroemer RP, Kent TA, Hulsebosch CE. Neocortical neural sprouting, synaptogenesis, and behavioral recovery after neocortical infarction in rats. Stroke. 1995;26:2135–2144. Zhang ZG, Zhang L, Jiang Q, Zhang R, Davies K, Powers C, Bruggen N, Chopp M. VEGF enhances angiogenesis and promotes blood– brain barrier leakage in the ischemic brain. J Clin Invest. 2000;106:829 – 838. Zhang ZG, Chopp M. Neurorestorative therapies for stroke: underlying mechanisms and translation to the clinic. Lancet Neurol. 2009;8:491–500. Chopp M, Li Y. Treatment of stroke and intracerebral hemorrhage with cellular and pharmacological restorative therapies. Acta Neurochir Suppl. 2008;105:79 – 83. Krupinski J, Kaluza J, Kumar P, Kumar S, Wang JM. Role of angiogenesis in patients with cerebral ischemic stroke. Stroke. 1994;25: 1794 –1798. Zhang RL, Zhang ZG, Roberts C, LeTourneau Y, Lu M, Zhang L, Wang Y, Chopp M. Lengthening the G(1) phase of neural progenitor cells is concurrent with an increase of symmetric neuron generating division after stroke. J Cereb Blood Flow Metab. 2008;28:602– 611. Thored P, Wood J, Arvidsson A, Cammenga J, Kokaia Z, Lindvall O. Long-term neuroblast migration along blood vessels in an area with transient angiogenesis and increased vascularization after stroke. Stroke. 2007;38:3032–3039. Taguchi A, Soma T, Tanaka H, Kanda T, Nishimura H, Yoshikawa H, Tsukamoto Y, Iso H, Fujimori Y, Stern DM, Naritomi H, Matsuyama T. Administration of CD34⫹ cells after stroke enhances neurogenesis via angiogenesis in a mouse model. J Clin Invest. 2004;114:330 –338. Arvidsson A, Collin T, Kirik D, Kokaia Z, Lindvall O. Neuronal replacement from endogenous precursors in the adult brain after stroke. Nat Med. 2002;8:963–970. Lindvall O, Kokaia Z, Martinez-Serrano A. Stem cell therapy for human neurodegenerative disorders— how to make it work. Nat Med. 2004; 10(suppl):S42–50. Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 1444 Stroke May 2011 33. Zhang L, Kokkonen G, Roth GS. Identification of neuronal programmed cell death in situ in the striatum of normal adult rat brain and its relationship to neuronal death during aging. Brain Res. 1995;677: 177–179. 34. Biebl M, Cooper CM, Winkler J, Kuhn HG. Analysis of neurogenesis and programmed cell death reveals a self-renewing capacity in the adult rat brain. Neurosci Lett. 2000;291:17–20. 35. Li Y, Chopp M, Jiang N, Yao F, Zaloga C. Temporal profile of in situ DNA fragmentation after transient middle cerebral artery occlusion in the rat. J Cereb Blood Flow Metab. 1995;15:389 –397. 36. Zhang R, Xue YY, Lu SD, Wang Y, Zhang LM, Huang YL, Signore AP, Chen J, Sun FY. Bcl-2 enhances neurogenesis and inhibits apoptosis of newborn neurons in adult rat brain following a transient middle cerebral artery occlusion. Neurobiol Dis. 2006;24:345–356. 37. Weiss ML, Medicetty S, Bledsoe AR, Rachakatla RS, Choi M, Merchav S, Luo Y, Rao MS, Velagaleti G, Troyer D. Human umbilical cord matrix stem cells: preliminary characterization and effect of transplantation in a rodent model of Parkinson’s disease. Stem Cells. 2006;24:781–792. 38. Cho PS, Messina DJ, Hirsh EL, Chi N, Goldman SN, Lo DP, Harris IR, Popma SH, Sachs DH, Huang CA. Immunogenicity of umbilical cord tissue derived cells. Blood. 2008;111:430 – 438. 39. Hallenbeck JM. Significance of the inflammatory response in brain ischemia. Acta Neurochir Suppl. 1996;66:27–31. 40. Schabitz WR, Berger C, Kollmar R, Seitz M, Tanay E, Kiessling M, Schwab S, Sommer C. Effect of brain-derived neurotrophic factor treatment and forced arm use on functional motor recovery after small cortical ischemia. Stroke. 2004;35:992–997. 41. Maric D, Fiorio Pla A, Chang YH, Barker JL. Self-renewing and differentiating properties of cortical neural stem cells are selectively regulated by basic fibroblast growth factor (FGF) signaling via specific FGF receptors. J Neurosci. 2007;27:1836 –1852. 42. Schabitz WR, Sommer C, Zoder W, Kiessling M, Schwaninger M, Schwab S. Intravenous brain-derived neurotrophic factor reduces infarct size and counterregulates Bax and Bcl-2 expression after temporary focal cerebral ischemia. Stroke. 2000;31:2212–2217. Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 Delayed Administration of Human Umbilical Tissue-Derived Cells Improved Neurological Functional Recovery in a Rodent Model of Focal Ischemia Li Zhang, Yi Li, Chunling Zhang, Michael Chopp, Anna Gosiewska and Klaudyne Hong Stroke. 2011;42:1437-1444; originally published online April 14, 2011; doi: 10.1161/STROKEAHA.110.593129 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2011 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/42/5/1437 Data Supplement (unedited) at: http://stroke.ahajournals.org/content/suppl/2012/02/28/STROKEAHA.110.593129.DC1.html Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/ Downloaded from http://stroke.ahajournals.org/ by guest on March 5, 2016 34 Stroke 日本語版 Vol. 6, No. 2 Abstract げっ歯類の局所脳虚血モデルにおいてヒト臍帯組織由来細 胞の遅延投与が神経学的機能回復を改善する Delayed Administration of Human Umbilical Tissue-Derived Cells Improved Neurological Functional Recovery in a Rodent Model of Focal Ischemia Li Zhang, MD1; Yi Li, MD1; Chunling Zhang, MD1; Michael Chopp, PhD1,2; Anna Gosiewska, PhD3; Klaudyne Hong, PhD3 1 Department of Neurology, Henry Ford Hospital, Detroit, MI; 2 the Department of Physics, Oakland University, Rochester, MI; and 3 Advanced Technologies and Regenerative Medicine, LLC, c/o Ethicon, Inc, Somerville, NJ 背景および目的:虚血性脳卒中患者の治療を成功させるた めの神経保護戦略は短い治療適応時間が要件となるため, 大部分の治療が妨げられる。しかし,神経再生に基づく臨 床治療によりこの治療時間枠が延長され,それによりこれ まで対応できなかった重要な課題に取り組むことができる 可能性がある。ヒト臍帯組織由来細胞は脳卒中の神経再生 治療薬候補として大きな可能性を示している。 方法:ヒト臍帯組織由来細胞の静脈内投与の有効性を, げっ歯類の中大脳動脈脳卒中モデルを用いて,用量漸増試 験( 検討した用量:3 × 105,1 × 106,3 × 106,または 1 × 107 cells/ 回 )とそれに続く投与時期に関する試験( 脳卒中 後の時間:第 1 日,第 7 日,第 30 日,第 90 日に用量 5 × 106 cells/ 回 )において検討した。対照はリン酸緩衝食塩 水注射およびヒト骨髄由来間葉系間質細胞の注射とした。 治療後の転帰測定には改変神経学的重症度スコアおよび接 着除去試験を用いた。全例について組織診断を実施し,シ ナプス形成,神経発生,血管新生,および細胞アポトーシ スを評価した。 結果:脳卒中後最長 30 日目に 3 × 106 cells 以上の用量を 投与した場合,ヒト臍帯組織由来細胞ではリン酸緩衝食塩 水と比較して改変神経学的重症度スコアおよび接着剤試験 結果に統計学的に有意な改善が認められた。3 × 106 cells 以上の用量では,組織学的評価により,リン酸緩衝食塩水 の投与を受けた対照動物と比較してヒト臍帯組織由来細胞 の投与を受けた動物の虚血性境界域でシナプス形成,血管 密度の増大,およびアポトーシスの低下が確認され,また 脳室下帯における前駆細胞の増殖の増加が確認された。 結論:これらの結果は,リン酸緩衝食塩水の対照群と比較 した場合のげっ歯類脳卒中モデルにおけるヒト臍帯組織由 来細胞の静脈内投与の有効性を示すものであり,ヒトに対 する使用の可能性について研究を進める根拠となる。 Stroke 2011; 42: 1437-1444 A PBS B hUTC 1000 800 400 200 LV PBS LV stroke6-2.indb 34 *p < 0.05 (8 例 / 群) 600 0 C 対側 PBS hUTC hUTC hUTC hUTC hMSC 0.3M 1M 3M 10M 3M hUTC LV D DCX(+)領域の割合(%) (平均値± SE) LV 細胞数 /mm2(平均値± SE) 同側 20 10 0 PBS hUTC ( A )PBS( 上 の パ ネ ル )お よ び 3 × 106 cells の用量の hUTC( 下のパネル )の投与を 受けたラットの同側 SVZ に BrdU 免疫反応 が認められる典型的な顕微鏡写真。( B )同側 および対側の脳室壁の BrdU 陽性細胞密度( 1 mm2 あたりの細胞数 )の定量的解析。( C ) PBS( 左のパネル )および 3 × 106 cells の 用量の hUTC( 右のパネル )の投与を受けた 図2 ラットの同側脳半球における DCX 免疫反応 を示す典型的な顕微鏡写真。( D )SVZ 内の DCX 発現の定量的解析。バー= 50 μ m。 *PBS 投与群との比較で p < 0.05。BrdU: ブロモデオキシウリジン,SVZ:脳室下帯, PBS:リン酸緩衝食塩水,hUTC:ヒト臍帯 組織由来細胞,hMSC:ヒト骨髄由来間葉系 間質細胞,DCX:ダブルコルチン。 11.9.27 10:54:06 AM
© Copyright 2025 Paperzz