ISSN 1881-901X
INCLUDED IN THIS ISSUE
Full Articles
運動障害の鑑別診断における神経化学的バイオマーカー
傍腫瘍性運動障害
Abstracts
セロトニンとパーキンソン病:運動機能,気分,精神疾患との関連
他 7 本収載
日本語版 Vol.3 No.3 January 2010
e-mail: ProductionJapan@wiley.com
日本語版
Vol.3 No.3 January 2010
監修:
水野 美邦
順天堂大学医学部附属
順天堂越谷病院院長
編集委員: 宇川 義一
(五十音順)
福島県立医科大学医学部
髙橋 良輔
京都大学医学研究科臨床神経学教授
神経内科学講座教授
野元 正弘
愛媛大学大学院医学系研究科
病態治療内科教授
梶 龍兒
徳島大学医学部神経内科教授
近藤 智善
公立大学法人和歌山県立医科大学
服部 信孝
順天堂大学医学部脳神経内科教授
神経内科教授
山本 光利
香川県立中央病院神経内科主任部長
Full Articles
運動障害の鑑別診断における神経化学的バイオマーカー
2
傍腫瘍性運動障害
17
Abstracts
セロトニンとパーキンソン病:
運動機能,気分,精神疾患との関連
パーキンソン病における衝動行動と強迫行動
27
34
パーキンソン病と多系統萎縮症における
進行性核上性麻痺における小脳病変:
臨床病理学的研究
胃筋電図所見の違い
36
早期パーキンソン病における抑うつ症状の経過
38
28
パーキンソン病患者の衝動性障害・強迫性障害に関する
質問票の妥当性検討
30
パーキンソン病におけるレボドパ空腸内注入:非運動症状
およびQOL への効果に関する予備的多施設共同試験
代謝比率で評価したパーキンソン病患者の大脳皮質の代謝
低下は主に認知機能低下を反映する:[18F]FDG-PET
表紙:代謝指数(MI,黄色)と代替代謝指数(MI*,オレンジ色)の
計算に使用したマスク処理画像(mask)
(Movement Disorders, 2009, Vol. 24 No. 10, page 1504)
40
32
Selected from Movement Disorders Vol. 24 No. 9-12, 2009
運動障害の鑑別診断における神経化学的
バイオマーカー
Neurochemical Biomarkers in the Differential Diagnosis of Movement Disorders
*, **
Brit Mollenhauer, MD and Claudia Trenkwalder, MD
*
Paracelsus-Elena Klinik, Kassel, Germany
Department of Neurology and Clinical Neurophysiology, Georg August University, Goettingen, Germany
*
*
近年,アルツハイマー病やクロイツフェルト - ヤコブ病
経変性疾患では CSF および血中の蛋白質に関する研究
な ど の 神 経 変 性 認 知 症 の 診 断 に 際 し, 脳 脊 髄 液
においてバイオマーカーによる鑑別診断の有用性が検
(cerebrospinal fluid; CSF)中の神経蛋白質の神経化学
討されてきた。パーキンソン病,Lewy 小体型認知症,
的解析が行われるようになってきた。CSF は中枢神経
多系統萎縮症,進行性核上性麻痺,大脳皮質基底核変
系を取り囲むように存在し,CSF 蛋白質の中には,血
性症の臨床診断は,現在でも主に国際分類基準で定義
液由来の蛋白質よりも意義のある脳特異的蛋白質も認
された臨床症状に頼っている。本論文では,これらの運
められている。CSF 中の特異的蛋白質濃度は,中枢神
動障害における CSF バイオマーカーをレビューすると
経系疾患のきわめて有望なバイオマーカーとなりうる。
ともに,神経変性疾患の神経化学的な生前診断に関して
我々は,さらに採取が容易な血中バイオマーカーを確立
最近発表された報告(最近の CSF 中α—シヌクレイン
する必要がある。認知症合併の有無にかかわらず,神
に関する知見も含む)について考察する。
Movement Disorders Vol. 24, No. 10, 2009, pp. 1411–1426
Key Word 運動障害,バイオマーカー,脳脊髄液
科学界は国際臨床分類基準の導入を通じ,神経変性疾
最近,National Institute of Neurological Disorders and
患の分類に少なからず努力してきた。特異的で神経防御・
Stroke-Alzheimer Disease and Related Disorders(NINCDS-
神経保護効果の期待できる新薬の登場に伴い,神経変性
ADRDA)の AD 作業部会による基準が改訂され,AD の
疾患の正確かつ早期の鑑別診断はとりわけ重要となって
バイオマーカーに関しては次のように記載された。
「AD
いる。しかし,神経画像検査などの専門的検査(technical
のバイオマーカーに関するエビデンスも増えつつあり,
investigation)に関するコンセンサスが得られ,多系統萎
これらを新たな AD 診断研究基準に加えることが容認さ
縮症(multiple system atrophy; MSA)の補助的診断基準
れる」3。この研究基準の最新版では,専門的検査(画像
の 1 つとして受け入れられるようになったのは,つい最
検査や CSF 蛋白質検査など)を補助的手段と位置づけて
近のことである。
いる。最近開発された病態特異的アミロイド蛋白質の in
理想的なバイオマーカーとは何かを考えた場合,その条
vivo 画像検査(Pittsburg compound B による)4 も研究基
件として,アルツハイマー病(Alzheimer’
s disease; AD)の
準に取り入れられた。CSF を用いる診断技術はエビデン
「本質的な神経病理学的特徴を検出できること,神経病理
スに基づいており,比較的安価で,広く利用可能である
学的な確定症例で妥当性が確認されていること〔
(AD を
にもかかわらず,検討対象となるまでに 15 年を要した 5,6。
検出するための)診断の感度> 80%,他の認知症との鑑
別の特異度> 80%〕
,信頼性が高く,再現性があり,非侵
襲的で,容易に実施でき,安価であること,少なくとも 2
つの独立した試験で検討されていること」が挙げられる 1,2。
2
CSF バイオマーカー
神経変性疾患では,脳周囲の体液である CSF は腰椎穿
B. Mollenhauer and C. Trenkwalder
刺で採取できる。CSF 組成が脳の生化学的変化をある程
度反映していることは明らかである。
(c)死後ではなく生前のヒトへの腰椎穿刺で得た CSF の
研究,とした。
一般に疾患特異的バイオマーカーは,その疾患の生化
すべての研究に共通する限界として,感度と特異度が
学的特徴〔例えばパーキンソン病(Parkinson’
s disease;
低い,独立したコホートによって結果の再現性が検証さ
PD)ではドパミン作動性経路〕
,神経病理学的特徴およ
れていない,疾患特異的な蛋白質もしくは蛋白質パター
び / または神経生理学的特徴(例えばシヌクレイノパチー
ンの測定方法はごく新しいものである,
などが挙げられる。
ではα—シヌクレイン)を反映する。代用マーカーと呼ば
れる別のタイプのバイオマーカーは,疾患に特異的な生
化学的,神経病理学的および / または神経生理学的特徴
とは独立した様々な発現パターンを反映する。
神経変性疾患に関連する CSF
蛋白質
タウ蛋白質
CSF における蛋白質動態
リン蛋白質タウ(68 kDa)は微小管の安定化に重要な
役割を果たし,自然状態では折りたたまれていない微小
血液 - 脳(厳密には血液 -CSF)関門を形態学的に捉え
管関連蛋白質である 11。AD における神経原線維変化は,
た「漏出(leakage)
」モデルとは対照的に,これを分子流
対をなすらせん状の蛋白フィラメントで,神経細胞の細
速と CSF 流量のより動的なプロセスとして捉える最近の
胞骨格に認められる 12,13。これらの蛋白フィラメントは,
理論により,少なくとも CSF 蛋白質濃度の調節に関する
微小管に関連する不溶性かつ安定性の低分子タウ蛋白ポ
我々の理解は深まった 7。CSF 蛋白質濃度はその起源(血
リマーである 14。微小管への親和性は,潜在する 79 部位
液または脳)に依存し,
血液由来蛋白質濃度は,
脊髄に沿っ
の異なるリン酸化によって調節されている 15,16。フィラメ
た CSF への受動拡散によって脳室から腰椎腔(lumbar
ント状沈着物を伴うヒト疾患の場合,タウ蛋白質は過剰
space)に至るまでの間,持続的に上昇していく 。CSF
にリン酸化されているが,これはフィラメント集合に先
が流れるための駆動エネルギーは,動脈血液系と静脈血
立つ初期変化であると考えられる 13,17。
7,8
液系の圧力差で生じる 9。血液 - 脳関門が障害された場合
AD 患者では CSF 総タウ蛋白質(以下,CSF タウ蛋白
には,主として CSF 流量が CSF 中の血液由来蛋白質濃
質とする)濃度が上昇するが,その濃度は 300 ~ 900 pg/
度を調節することになる。CSF 流量が低下すると,それ
mL と研究によって異なっている 18,19。ただし,タウオパ
らの蛋白質の分子流速が増加する 8,10。
チー以外の神経変性疾患でも,複数の単独例で CSF タウ
蛋白質濃度の上昇が認められている 20,21。一方,タウオ
方 法
Table 1 に,PD,Lewy 小体型認知症(dementia with
パチーであっても正常な CSF タウ蛋白質が検出される場
合もある 22,23。これらの結果から,CSF タウ蛋白質はタウ
関連疾患に特異的な所見ではないと考えられる。
Lewy bodies; DLB)
,MSA,進行性核上性麻痺(progressive
クロイツフェルト - ヤコブ病(Creutzfeldt-Jakob disease;
supranuclear palsy; PSP)
,大脳皮質基底核変性症
CJD)
患者のCSFタウ蛋白質濃度は通常1,300 pg/mLを超え,
(corticobasal degeneration; CBD)を対象とした CSF バイ
広範な神経細胞喪失による細胞内分画を反映している 24,25。
オマーカーに関する既発表研究の概要を示す。この一覧
さらに,脳卒中のような他の急性神経疾患でも CSF タウ蛋
表はすべての研究を網羅したものではなく,以下の用語
白質濃度の上昇を示すことから,神経細胞喪失のマーカー
で検索した PubMed 論文である(2008 年 5 月まで)
。単
としての役割を担っていることが示唆される 26。
一疾患名としての「パーキンソン病(Parkinson disease)
」
CSF タウ蛋白質濃度の測定は,PD ならびに認知症を伴
「Lewy 小体型認知症(dementia with Lewy bodies)
」
「多系
う PD(Parkinson’
s disease with dementia; PDD)と AD と
統萎縮症(multiple system atrophy)
」
「進行性核上性麻痺
の鑑別に役立つ可能性があるが 27,対照群と比べると PD
(progressive supranuclear palsy)
」
「大脳皮質基底核変性症
(PDD
および PDD の CSF タウ蛋白質の差はわずかである 28
」
, な ら び に「 脳 脊 髄 液
(corticobasal degeneration)
73 例,PD 23 例,非認知症性神経疾患の対照 41 例;カッ
(cerebrospinal fluid)
」
。適格基準は,
(a)バイオマーカー
トオフ値 250 pg/mL での PDD に対する感度 42%,特異度
に焦点を絞った研究,
(b)対象患者が 7 名を超える研究,
88%)
。DLB の場合には,CSF タウ蛋白質濃度は AD より
3
運動障害の鑑別診断における神経化学的バイオマーカー
CSF DIAGNOSTICS IN MOVEMENT DISORDERS
1413
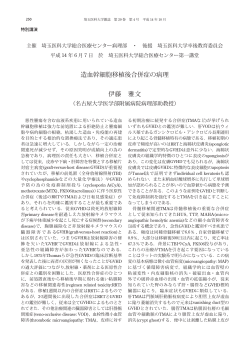
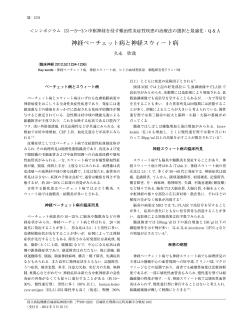
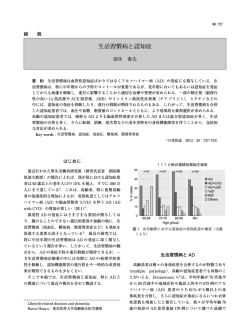
Table 1 パーキンソン病(PD)
,Lewy 小体型認知症(DLB)
,多系統萎縮症(MSA)
,進行性核上性麻痺(PSP)
,
TABLE 1. CSF biomarker in Parkinson disease (PD), dementia with Lewy Bodies (DLB), multiple system atrophy (MSA),
大脳皮質基底核変性症(CBD)の CSF バイオマーカー
progressive supranuclear palsy (PSP) or corticobasal degeneration (CBD)
Marker
4
CSF DIAGNOSTICSPD
IN MOVEMENT
DISORDERS MSA
DLB
PSP
1413
CBD
129,130
129
8-hydroxy-20 -deoxyguanosine (8-OHDG),
8-hydroxyguanosine
(8-OHG) in Parkinson disease (PD), dementia with Lewy Bodies (DLB), multiple system atrophy (MSA),
TABLE 1. CSF biomarker
Acetyl choline
126–128
progressive supranuclear palsy
(PSP) or corticobasal degeneration (CBD)
Angiotensin-converting enzyme (ACE)
131,132
133
131
Acetylcholinesterase (AChE) and butyrylcholinesterase
134–139
140
141–143
Marker
PD
DLB
MSA
PSP
CBD
(BChE)
0
129,130
129
8-hydroxy-2
Amino acids -deoxyguanosine
and metabolites (8-OHDG),
144–158
159,160
156,158,161
8-hydroxyguanosine
(8-OHG)
Annexin
V
162
Acetyl
choline
126–128
Bcl-2 protein
163
Angiotensin-converting
(ACE)
131,132
133
131
Biogene amine and theirenzyme
metabolites
30,132,135,139,
119,120
(30,101,140,164,
Acetylcholinesterase (AChE) and butyrylcholinesterase
134–139
140
141–143
155,164–193
165,184,194,195
(BChE)
C4d
complement protein
196
Amino and
acidscGMP
and metabolites
144–158
159,160
156,158,161
cAMP
197–201
Annexin V
162
Carnitine
202
Bcl-2 protein
163
Ceruloplasmin
203
Biogene amine Aand
30,132,135,139,
119,120
(30,101,140,164,
Chromogranin
andtheir
B metabolites
204
155,164–193
165,184,194,195
Coenzyme Q-10
205
C4d
complement protein
196
Delta-sleep-inducing
peptide (DSIP), phosphorylated
206
cAMP
and cGMP
197–201
Delta-sleep-inducing
peptide (p-DSIP)
Carnitine
202
DJ-1 (PARK7)
207
Ceruloplasmin
203
Dipeptidyl-aminopeptidase II (DAP II)
208
Chromogranin
204
Ferroxidase A and B
209
Coenzyme
Q-10
205
Ferritin
210,211
210
Delta-sleep-inducing
206
Glial fibrillary acidic peptide
protein (DSIP),
(GFAP) phosphorylated
30,116
30,116
Delta-sleep-inducing
peptide (p-DSIP)
Glutathione
peroxidase (GPx)
DJ-1
(PARK7)
207
4-hydroxynonenal
(HNE)-conjugated GPx
212
Dipeptidyl-aminopeptidase
II (DAP II)hormone (GHRH)
208
Growth hormone (GH), GH-releasing
213
Ferroxidase
209
Growth-associated protein 43 (GAP-43)
214
Ferritin
210,211
210
Harman and norharman
215
Glial
fibrillary
protein
(GFAP)
30,116
30,116
Heart-fatty
acidacidic
binding
protein
(H-FABP)
93
91–93
Glutathione
peroxidase (GPx)
Homocarnosine
151
4-hydroxynonenal
(HNE)-conjugated GPx
212
Homocystein
216
Growth
hormone (GH),
213
Hydroxyindoleacetic
acidGH-releasing
(HYDA) hormone (GHRH)
140
Growth-associated
protein 43 (GAP-43)
214
Interleukins
217,218
219
Harman
and norharman
215
Isoprostanes
220
Heart-fatty
acid binding protein (H-FABP)
93
91–93
Lysosomal enzymes
221
Homocarnosine
151
Metals
222–228
229
230
Homocystein
216
Methionine-enkephalin
172,231
Hydroxyindoleacetic
acid (HYDA)
140
Methyl-6,7-dihydroxy-1,2,3,4-tetrahydroisoquinolines
187,188,232
Interleukins
217,218
219
(2-MDTIQ); (1-MDTIQ, salsolinol);
Isoprostanes
220
N-methyl-norsalsolinol
Lysosomal
enzymes
221
Myelin basic
protein (MBP)
30
30,31
Metals
222–228
229
230
Neopterin and biopterin
157,233,234
Methionine-enkephalin
172,231
Neural thread protein
235
236
Methyl-6,7-dihydroxy-1,2,3,4-tetrahydroisoquinolines
187,188,232
Neurofilaments heavy and light chain (NFL, NFH)
31,115,116
237
101,115,116,
115,116,239
(2-MDTIQ); (1-MDTIQ, salsolinol);
195,238,239
N-methyl-norsalsolinol
Neuronspecific
enolase (NSE)
30
30,101
Myelin
basic protein (MBP)
30 165,
30,31
Neuropeptides
135,139,
165,249
249,250
Neopterin and biopterin
157,233,234
172, 185, 197,
Neural thread protein
236
231,235
240–248
Neurofilaments
31,115,116
237
101,115,116,
115,116,239
Neuroserpins heavy and light chain (NFL, NFH)
133
195,238,239
Nitrite, nitrate, nitric oxide metabolites
199,210, 251–253
159
210
Neuronspecific
enolase (NSE)
30
30,101
Orexin A/hypocretin-1
110
110,254
101,255
110
110
Neuropeptides
135,139,
165,249
249,250
Oxidative stress indices
227 165,
172,208
185, 197,
Post-proline cleaving enzyme
231, 240–248
Proteins 14-3-3
256–259
Neuroserpins
133
Reelin
260
260
Nitrite,
nitrate, nitric oxide metabolites
199,210,30251–253
159
210
1414 protein
B. MOLLENHAUER
AND C. TRENKWALDER
S100B
20,261
30,101
Orexin
A/hypocretin-1
110
110,254
101,255
110
110
Secretogranin
II
204
Oxidative
stressofindices
227
Soluble forms
intercellular adhesion molecule-1
133
Post-proline
cleaving
enzyme
2081. (Continued )
(sICAM-1),
vascular
cell adhesion molecule-1
TABLE
Proteins
14-3-3and platelet endothelial cell adhesion
256–259
(sVCAM-1)
Reelin
260
260
molecule-1 (sPECAM-1)
Marker protein
PD
DLB
MSA
PSP
CBD
S100B
30
20,261
30,101
Superoxide
dismutase activity (SOD) (Cu, Zn, MN)
227,262
212,263
Secretogranin
204
Tau isoforms II
264
264
264
264
Soluble
forms
of intercellular adhesion molecule-1
133
Tau protein
(total)
27,28,31,154,
20,33,39,54,93,
30,101
22,32,271
22,32,56,
(sICAM-1), vascular cell adhesion molecule-1
214,235,265
219,237,261,
271,272
(sVCAM-1) and platelet endothelial cell adhesion
264,266–270
molecule-1
(sPECAM-1)
Tau
protein phosphorylated
27
39,237,261,264,
271
Movement Disorders,
Vol. 24, No.56,271
10, 2009
Superoxide dismutase activity (SOD) (Cu, Zn, MN)
227,262
212,263
267,270,273–275
Thyroid-stimulating hormone (TSH) response to
213
thyrotropin-releasing hormone (TRH)
TNF-alpha
276
Transglutaminase
277
Urate
278
Movement Disorders, Vol. 24, No. 10, 2009
Vitamins alpha-tocopherol (vitamin E);
154,279,280
194
Thiamine (vitamin B1)
Xanthine
278
a-synuclein (total and oligomeric)
74,77–79,
78,281
281
86,281
1414
B. MOLLENHAUER AND C. TRENKWALDER
TABLE 1.
Marker
1414
(Continued )
PD AND C. TRENKWALDER
DLB
B. MOLLENHAUER
Tau isoforms
Tau protein (total)
Tau
protein phosphorylated
Marker
264
264
27,28,31,154,
20,33,39,54,93,
Table
1 214,235,265
219,237,261,
TABLE
1. (つづき)
(Continued
)
264,266–270
27
39,237,261,264,
PD
DLB
267,270,273–275
264
264
27,28,31,154,
20,33,39,54,93,
214,235,265
219,237,261,
276
264,266–270
277
27
39,237,261,264,
278
267,270,273–275
154,279,280
B. Mollenhauer PSP
and C. Trenkwalder
MSA
CBD
30,101
264
22,32,271
264
22,32,56,
271,272
MSA
271
PSP
56,271
CBD
Tau isoforms
264
264
Thyroid-stimulating
hormone (TSH) response to
213
Tauthyrotropin-releasing
protein (total)
30,101
22,32,271
22,32,56,
hormone (TRH)
271,272
TNF-alpha
Transglutaminase
Tau
271
56,271
Urateprotein phosphorylated
Vitamins alpha-tocopherol (vitamin E);
194
Thyroid-stimulating
(TSH) response to
213
Thiamine (vitaminhormone
B1)
thyrotropin-releasing hormone (TRH)
Xanthine
278
TNF-alpha (total and oligomeric)
276
a-synuclein
74,77–79,
78,281
281
Transglutaminase
277
86,281
Urate
278
b 2-microglobulin
282
Vitamins
alpha-tocopherol
(vitamin E);
154,279,280
194
b-Amyloid
1-40
20,269
Thiamine1-40*
(vitamin
B1)
b-Amyloid
(oxidized)
58,59,266
58,59,266
Xanthine
278
b-Amyloid 1-42
28,54,55,214,
20,33,39,54,219,
55
55,271
56,289
a-synuclein (total and oligomeric)
74,77–79,
78,281
281
265,283
237,270,275
86,281
b-Amyloid peptide pattern
57
57
57
57
57
b 2-microglobulin
282
死後ではなく生前のヒトへの腰椎穿刺で得た
CSFthan
を対象とし,バイオマーカーに焦点を当てた対象患者
8 例以上の研究のみを掲載した(齧
b-Amyloid
1-40with a biomarker focus, and more
Only studies
7 patients were included, as20,269
were studies based only
on intra vitam, not post mortem,
b-Amyloid
1-40*
(oxidized)
58,59,266
gained
CSFのみを扱った研究は除外)
by lumbar
puncture in humans
from rodents were 58,59,266
excluded).
歯類の
CSF
。 (studies on CSF only
b-Amyloid 1-42
28,54,55,214,
20,33,39,54,219,
55
55,271
56,289
265,283
237,270,275
b-Amyloid peptide
pattern
57
57
57の方がより小規模である
57
5737,38。
的な共通点であるが,DLB
も低く,PD
および
PDD よりも高い 20(DLB 71 例,AD
tau levels in MSA patients (MSA-P and MSA-C) were
towards AD by p-tau protein 181 than with total tau
shown
to
be
elevated
compared
to
PD,
possibly
due
to
protein (DLB n 5 18; AD n 5 23).
gained CSF29 by lumbar puncture in humans (studies on CSF only from rodents were excluded).
で「DLBaxonal
がほぼ確実(probable
分類基準
度は,総タウ蛋白質よりも p タウ蛋白質 181 の方が高い
more widespread
degeneration inDLB)
MSA」と判定
relative
20
5 15; MSA-C n 5 14; PD n 5 35;
to PD30 (MSA-P n タウ蛋白質濃度が低い傾向にある
Amyloid-b-Peptides
。
18 例,AD 23 例)
。
された患者は,CSF
としている 39(DLB
31
sensitivity
95%,
specificity
77%)
(MSA-P
n
5
19;
Different
of protein
Amyloid-b
peptides
tau levels in MSA patients
(MSA-P and MSA-C) were
towards
AD lengths
by p-tau
181 (Ab)
than with
totalarise
tau
最近の研究では,MSA
患者〔パーキンソン型多系統萎縮
PD n 5to31;
76%, specificity
97%). In due
CBD,
through39enzymatic
the23).
120 kDa transmemshown
be sensitivity
elevated compared
to PD, possibly
to
(DLB n 5cleavage
18; AD of
n5
protein
症(parkinsonian
variantelevated
of multipleCSF
system
atrophy;
MSA-P)
アミロイドβペプチド
there widespread
were slightly
tauin
protein
levels
brane amyloid precursor protein (APP) by three differmore
axonal degeneration
MSA relative
30
compared
to
controls
and
PSP
patients
as
reported
by
および小脳型多系統萎縮症(cerebellar
variant
of
multiple
kDa の膜貫通性アミロイド前駆体蛋白質(amyloid
ent120secretases,
resulting
in either carboxyterminally
n
5
15;
MSA-C
n
5
14;
PD
n
5
35;
to PD (MSA-P
Amyloid-b-Peptides
22
32
40
31 n 5 12);
(CBD
n
5
10;
PSP
(CBD
Urakami
et
al.
cleavage
truncated
or
–elongated
Ab
peptides.
sensitivity
95%,
specificity
77%)
(MSA-P n 5
system
atrophy;
MSA-C)
〕の CSF
タウ蛋白質濃度が
PD19;
患
precursor
protein;
APP)が
3
つの異なるセクレターゼで酵素
Different lengths of Amyloid-b
(Ab) This
peptides
arise
nPD5n 27;
PSPsensitivity
n 5 30; 76%,
sensitivity
81, 5 97%).
and specificity
is
divided
into
an
amyloidogenic
processing
conducted
5
31;
specificity
In
CBD,
through enzymatic長さの異なる複数のアミロイドβ(Aβ)
cleavage of the 120 kDa transmem者よりも高いことが示されたが,これは
PD
に比べ
MSA
で
的に切断されると,
41,42
80%
a cut-off
of 180
pg/mL);
waslevels
also
by
b-secretase
(called BACE-1)
and b-secretase,
there atwere
slightly
elevated
CSFthistaufinding
protein
brane
amyloid precursor
protein (APP)
by three differ33
30
shown
in an
independent
smallas sample
(MSA-P
は軸索変性がより広範囲なせいかもしれない
ペプチドが産生される。これらはカルボキシル末端側が
and
a nonamyloidogenic
by metalloprocompared
to controls
and but
PSPvery
patients
reportedset15
by
ent secretases,
resulting43inprocessing
either carboxyterminally
22
(CBD
n
5
3;
PSP
n
5
6).
3132
40
The
emerging
vary
teases
called
a-secretase.
40 peptides
例,
MSA-C 14
35 例;感度
特異度
n 5 95%,
10; PSP
n 577%)
12);(MSA-P
(CBD
Urakami
et 例,
al. PD(CBD
。この切
短縮もしくは延長された
Aβペプチドである
truncated or –elongated Ab peptides. This cleavage
As
hyperphosphorylation
of
tau
protein
promotes
its
in
their
proneness
to
aggregate,
depending
on
their
5 27; PSP
n 5 30;76%,特異度
sensitivity 81,
5 。Urakami
and specificity
is divided into an amyloidogenicと呼ばれる)とγセクレ
processing conducted
97%)
ら 22
19n
例,PD
31 例;感度
断は,βセクレターゼ(BACE-1
44
aggregation
through
the facilitation
process
neurofilength
and the degree
post-translational
oxidation.
41,42
80%
at a cut-off
of 180
pg/mL); this
findingofwas
also
by
b-secretase
(called ofBACE-1)
and b-secretase,
41,42
が報告しているように,CBD
では,CSF
タウ蛋白質濃度
33
ターゼによるアミロイド産生プロセシング
brillary intangles,
it is obvious
that
quantification
Amyloid-plaques
depositedprocessing
in the brain
ofと,αセク
patients
shown
an independent
but
verythe
small
sample setof
and a nonamyloidogenic
by metallopro40,45
phosphorylated
tau
protein
in
CSF
might
serve
as
an
mainly
consist
of
carboxytermiwith
AD
and
DLB
が対照および
レターゼと呼ばれるメタロプロテアーゼによる非アミロ
(CBD n 5 3;PSP
PSP患者に比べてわずかに高かった(CBD
n 5 6).
teases called a-secretase.43 The emerging peptides vary
even
more
specific
marker for
AD
apart from
neuronal
nally-elongated
formstoof
Ab peptides
such as Ab
32
43aggregate,
As
hyperphosphorylation
of
tau
protein
promotes
its
in their proneness
depending
on 1-42.
their
10 例,PSP3412 例) (CBD 27 例,PSP 30 例;カットオフ
に分けられる。切断後に生じる
イド産生プロセシング
cell
loss.
For
CSF
tau
protein
phosphorylated
at
threoStudies
in
transgenic
mice
have
shown
that
the
lack of
44
aggregation through the facilitation process of neurofilength
and
the
degree
of
post-translational
oxidation.
46
値
180181
pg/mL
で感度
81%,特異度
80%)
。この所見は,
ペプチドは,その長さと翻訳後酸化程度によって凝集傾
nine
(p-tau
protein
181),
Blennow
et
al.
showed,
for
APP
leads
to
impaired
neuronal
function.
brillary tangles, it is obvious that the quantification of
Amyloid-plaques deposited in the brain of patients
33 to
44
the
first time in 1995,
elevated
AD compared
In AD
1992,
Seubert
et al.
demonstrated
existence of
非常に小規模ではあるが,独立したサンプルセット
。AD
および
DLBconsist
患者の脳内に沈着するア
向が異なる
phosphorylated
tau protein
in levels
CSF in
might
serve as で
an
mainly
ofthecarboxytermiwith
and
DLB40,45
27
5
healthy
controls
and
other
neurodegenerative
diseases.
This
observation
extracellular
Ab,
including
CSF.
40,45 of Ab peptides such as
even more specific 3marker
for6 例)
AD。apart from neuronal
nally-elongated forms
Ab 1-42.
も確認された(CBD
例,PSP
は,主として Aβ 1-42 などの
Aβ
ミロイドプラーク
34epitope phosphorylations of CSF tau protein
Different
offered
new
opportunities
for
developing
diagnostic
cell loss. For CSF tau protein phosphorylated
at threoStudies
in
transgenic
mice
have
shown
that
the
lack
of
23,27,35,36
タウ蛋白質のリン酸化が過剰に亢進すると,神経原線
ペプチドのカルボキシル末端延長型からなる。トランス
have
been(p-tau
analyzed
for their
value.
tests
for AD.
Initially,neuronal
Motter et
al. reported
signifi46
nine 181
protein
181),diagnostic
Blennow et
al. showed, for
APP leads
to impaired
function.
respect
to DLB,
the neuropathological
overlap
cantly
decreased
levels
CSF Ab 1-42theinの欠損が神経
37 patients
維変化の促進プロセスを通してその凝集が加速されるこ
ジェニックマウスを用いた研究では,APP
theWith
first time
in 1995,
elevated
levels in AD compared
to
In 1992,
Seubert
et al.ofdemonstrated
existence
of
27
with
AD
involves
the
phosphorylation
of
tau
protein,
with
AD,
compared
to
32
neurological
disease
controls
5
healthy controls
and other
neurodegenerative diseases.
This46。
observation
extracellular Ab, including CSF.
とから,CSF
中のリン酸化タウ蛋白質の定量化は,神経
機能障害を引き起こすことが示されている
37,38
6
Some of
CSF
have
but to a epitope
lesser extent.
Since
then, there
have
and
20 nondemented
controls.
Different
phosphorylations
CSFstudies
tau protein
offered
new opportunities
for などの細胞外にも
developing
diagnostic
細胞喪失とは別に,AD
のより特異的なマーカーとして用
1992
年に,Seubert
らはand
CSF
Aβが
revealed
a
better
specificity
for
the
discrimination
23,27,35,36
been
several
independent
multicenter
studies
replihave been analyzed for34 their diagnostic value.
tests for AD. Initially, Motter
et al. reported signifi5
。1995
年に Blennow らは,スレ
いられる可能性がある
。この観察所見は,AD
の
存在することを明らかにした
With respect to DLB,
the neuropathological
overlap
cantly decreased levels of CSF
Ab 1-42 in 37 patients
with AD
involves the phosphorylation
of tau protein,
オニン
181 でリン酸化された
CSF タウ蛋白質(p
タウ蛋
with
AD,
compared
to
32
neurological
disease
controls
診断検査法を開発する新たなきっかけとなった。まず
37,38
but 181)濃度は,AD
to Disorders,
a lesserVol.extent.
then, there have
and 20 らは,神経疾患の対照群
nondemented controls.6 Since
Movement
24, No.
10, 2009Some CSF studies have
白質
患者では健常対照および他の神経
Motter
32 例ならびに非認知症
revealed a better specificity for the discrimination
been
several
independent
and
multicenter
studies repli27
67 例,
非認知症性神経疾患の対照
例)
。興味深いことに,
一部のas39
CSF
Only
studies with a biomarker focus,41and
more
than 7 patients were included,
were研究では,DLB
studies based onlyと
onAD
intraとの鑑別における特異
vitam, not post mortem,
変性疾患患者よりも高いことを初めて示した 。CSF タ
の対照群 20 例に比べ,AD 患者 37 例では CSF の Aβ
ウ蛋白質の異なるエピトープのリン酸化については,そ
1-42 濃度が有意に低いことを報告した 6。その後,この成
23,27,35,36
。
の診断的価値が解析されている
Movement Disorders, Vol. 24, No. 10, 2009
績を再現するいくつかの独立した多施設共同研究が報告
タウ蛋白質のリン酸化は,DLB と AD との神経病理学
されている 19。その中には神経病理学的変化との相関を
5
運動障害の鑑別診断における神経化学的バイオマーカー
示す研究もあったが 47,その研究は最適とは言えない死
ト法でも確認されている 57(PD 11 例,PSP 20 例,CBD
後採取 CSF で実施されていた(下記参照)
。脳内の Aβ
12 例,MSA 18 例,DLB 20 例,神経疾患の対照 19 例)
。
プラークが Aβ 1-42 の「巣窟(sink)
」として働き,脳と
CSF 間の可溶性 Aβ 1-42 の輸送を妨げるとの理論 6,48 は,
Aβ 1-40OX
AD 患者で CSF 中の Aβ 1-42 が少ない理由として広く受
け入れられている。
最近,SDS-PAGE/ イムノブロット法により,新規の A
βペプチドが同定された。このペプチドは,すでに知ら
CSF 中の Aβ 1-42 は従来の ELISA(Enzyme-Linked
Immunosorbent Assay)法,免疫沈降質量分析法,ウエス
タン/イムノブロット法で測定することができる
。A
6,49,50
れている断片 Aβ 1-40 によく似た生理化学的性質をもつ
ことが示されたが,易動度は非定型的であった。その後,
このペプチドはαヘリックス構造を有する,Aβ 1-40 の
βのドデシル硫酸ナトリウム(sodium dodecylsulfate;
酸化型(Aβ 1-40OX)と同定された 58,59。DLB 患者(21 例)
SDS)- ポリアクリルアミドゲル電気泳動(polyacrylamide
では,PDD 患者(21 例)や非認知症対照群(23 例)に
gel electrophoresis ; PAGE)/ イムノブロット法は Wiltfang
比べ Aβ 1-40OX が特異的に上昇することが示されている。
ら 50 によって導入された方法で,Aβペプチドと他の
AD 患者では Aβ 1-40OX がやや上昇しているが,DLB と
APP 代謝物を電気泳動により分離し,ウエスタン / イム
の重複はわずかであるため,DLB では Aβ 1-40OX が独自
ノブロットで超高感度に検出することができる。この方
の病態生理学的代謝を受けているとの議論も成り立つと
法では,8 M 尿素処理を加えることによって 1 つのアミ
考えられる。ただし,これについては独立した研究グルー
ノ酸のみが異なる CSF Aβペプチドも分離可能である。
プによるさらなる解明と結果の再現が必要である。Aβ
本 法 で 検 討した結 果,Aβペ プ チド 1-42,1-40,1-39,
1-40OX をマーカーとする診断感度はそれぞれ 81%および
1-38,1-37 が CSF およびその他の細胞外体液中に恒常的
71%であった。
に存在することが明らかになった 。検出限界は,Aβペ
51
プチド 1-40 が 600 pg/mL,Aβペプチド 1-42 が 1 pg/mL
CSF および血清中のα—シヌクレイン
であった 。アッセイ間およびアッセイ内変動は 10%未
α—シヌクレインは 140 個のアミノ酸からなり,主とし
満であった 。この方法には従来の ELISA 法を上回る価
てシナプス前に存在し,PD と DLB の病理学的特徴であ
値のあることは明らかであるが,複数の独立した研究グ
る Lewy 小体や,MSA のグリア細胞質封入体に認められ
ループあるいはより多くのサンプルによって結果の妥当
る細胞内凝集体の主要成分である 60,61。約 16 kDa のα—
性が確認されていないため,本法をハイスループット解
シヌクレインをコードする SNCA 遺伝子において,遺伝
析(大量高速解析)に用いるのは適当ではない。
性のパーキンソニズムと認知障害を引き起こす 3 つ(本
52
53
一般に Aβペプチドは翻訳後修飾(特にメチオニン 35
の酸化)を非常に受けやすいため,解析前試料の取り扱
64
いはきわめて重要である(下記参照)
。
認されている 65,66。発症年齢や臨床症状の重症度,とりわ
大部分の研究では,PD 患者の CSF Aβ 1-42 は対照群
と比べ正常ないし軽度低下していると報告されているが,
,新たに SNCA 遺伝子の重複(multiplication)現象が確
け 認 知 機 能 の 低 下は,遺 伝 子 量(duplication ないし
triplication)に依存すると考えられる。
(PD 15 例,
DLB 患者の CSF Aβ 1-42 は通常低下している 54
α—シヌクレインのホメオスタシスに関する生体内動態
DLB 11 例,対照 19 例)
。PD 患者の CSF Aβ 1-42 濃度は,
は様々な代謝イベントによって変化し,この動態に応じて
より長期の罹病期間および認知障害の併発に伴って低下
シヌクレイノパチーが促進される 223。α—シヌクレインの
する傾向がある (PD 73 例,PDD 23 例,神経疾患の対
動態を変化させる代謝イベントには,合成速度の上昇 68,
照 41 例;カットオフ値 350 pg/mL での PDD に対する感
protofibril(原線維)を生成する変異体の沈着増加 69,セ
。
度 85%,特異度 41%)55(PD 48 例,健常対照 32 例)
リン 129 の持続的リン酸化 70,C 末端の短縮,分解の低
このような Aβ 1-42 濃度の低下は,MSA55(MSA 36 例)
下 71 などがある。最近,α—シヌクレインの分解経路が検
に加え,
一部の研究では PSP と CBD でも認められ 55(PSP
討され,プロテオソームあるいはリソソーム活性の関与
15 例) (PSP 18 例,CBD 9 例,神経疾患の対照 43 例;
が示された 71-73。細胞内α—シヌクレインが減少する別の
AD と比較した場合の感度と特異度は PSP では 43%と
機序として,細胞間腔への放出が考えられる 74。完全長
92%,CBD では 64%と 91%)
,ウエスタン / イムノブロッ
のα—シヌクレインは,血漿や調製細胞培養液などの生
28
56
6
論文執筆時)のミスセンス変異が発見されたのに続き 62-
B. Mollenhauer and C. Trenkwalder
体試料中において検出されている 73,74。したがって,我々
上昇していることを見出した 242(PD 34 例,非神経疾患
のグループや他の研究者は,細胞外α—シヌクレインの
の対照 27 例;感度 51%,特異度 85%)
。
定量化がシヌクレイノパチーの有望なバイオマーカーに
なりうると判断している
。
抗体ならびに全α—シヌクレインおよびオリゴマーα—
シヌクレインの ELISA 法については,特異性に関してさ
75-78
ヒト CSF 中にα—シヌクレインが存在することは,こ
れまでに 2 つの研究で報告されている。1 つ目の研究では,
らなる検証が必要であり,
血液および CSF を様々なコホー
トで検討する独立した研究も必要である。
α—シヌクレインに対する同一抗体が濃縮と検出に使用さ
れたため,非特異的反応である可能性が残されている 79。
心臓由来脂肪酸結合蛋白質
2 つ目の研究では,剖検時に CSF が採取されたため,自
当初,心臓由来脂肪酸結合蛋白質(heart-type fatty acid-
己融解が結果に影響した可能性がある 。CSF 中にα—
binding protein; H-FABP)は,CJD の CSF バイオマーカー
シヌクレインが存在することの最終的な証明は,アフィ
候補として 2 次元ゲル電気泳動法で同定された 87。脂肪
ニティ濃縮と質量分析によって示された 78。
酸結合蛋白質は,脂肪酸の取り込み,輸送,代謝に関与す
74
腰椎穿刺で採取した CSF に関する複数の独立した横断
る 14 ~ 16 kDa の細胞質蛋白質である。心筋から最初に精
的研究では,PD および DLB 患者の CSF α—シヌクレイン
製された H-FABP は 88,心虚血と脳傷害の生化学マーカー
は,対照患者や AD 患者に比べ有意に少ないことがサンド
としてすでに評価されている 89。H-FABP は,脳での発現
イッチ ELISA 法による測定で示された (PD 8 例,DLB
も含め,広汎な組織分布を示すことが確認されている 90。
55 例,神経疾患の対照 13 例;これとは独立したサンプル
CJD 症例では CSF 中 H-FABP 濃度が上昇していること
サブセットは PD 5 例,DLB 6 例,健常対照 4 例) (PD
が独立した複数の研究グループによって示されているが,
33 例,健常対照 9 例と神経疾患の対照 29 例からなる対照
これは神経変性に起因する可能性が最も高い 87,91。血清
被験者 38 例;受信者動作特性曲線下面積 0.874)
。これら
H-FABP 濃度の上昇はすでに DLB と PD で示されており 92
とは別の ELISA 法による研究では,同様の結果は認めら
(PD 63 例,DLB 17 例,AD 23 例,神経疾患の対照 10 例;
78
77
。
れなかった (PD 15 例,DLB 15 例,健常対照 55 例)
80
93
(PD
DLB と AD を比較した場合の感度 47%,
特異度 91%)
現時点では CSF 中のα—シヌクレインが減少する機序
45 例,PDD 25 例,神経疾患の対照 51 例;DLB と AD を
は明らかにされていないが,第 1 にα—シヌクレインの細
比較した場合の感度 71%,特異度 69%,PDD と対照を比
胞内凝集による細胞間腔への放出低下,第 2 に SNCA 遺
較した場合の感度,特異度 64%)
,その原因として心臓交
伝子転写の変化 ,mRNA 発現の変化 ,あるいは蛋白
感神経組織の損傷が考えられる。血清 H-FABP 濃度と 123I-
質プロセシング 70 の変化,第 3 に CSF への血漿α—シヌ
メタヨードベンジルグアニン(metaiodobenzyl guanine;
クレインの透過低下を伴う CSF 流量増加,第 4 に CSF か
MIBG)心筋シンチグラフィーの相関は,血清濃度が交感
らのα—シヌクレインのクリアランス率の上昇 ,第 5 に
神経性組織の損傷を反映することを示している 94。
81
82
83
未知の因子あるいは複数の機序の協同による可能性が考
えられる。
S100B 蛋白質
末梢血漿中のα—シヌクレインに関する研究では,一
S100 蛋白質は,細胞質に存在する 21 kDa の二量体カル
貫した結果が得られていない。Lee らは,市販の ELISA
シウム結合蛋白質ファミリーの一員で,星状膠細胞とシュ
キットを用いて,PD および MSA では年齢を一致させた
。様々
ワン細胞に認められる 95(Bloomfield96 の総説参照)
健常対照と比べ血漿α—シヌクレイン濃度が上昇してい
な機序で細胞間腔に放出される S100B 蛋白質のβアイソ
ることを報告した 84(PD 105 例,MSA 38 例,健常対照
マー 97 は,急性神経疾患 98 のみならず神経変性疾患 99,100
51 例)
。一方,
Li らはウエスタンブロット法による測定で,
においても CSF 中での増加が示されている。S100B 蛋白
PD 患者では健常対照に比べ血漿α—シヌクレイン濃度が
質は一部の DLB 患者でわずかに増加することが示されて
(PD 27 例,
健常対照 11 例)
。
低下していることを報告した 85
,
いるが 20(DLB 71 例,非認知症性神経疾患の対照 41 例)
この不一致は,ELISA 法ではオリゴマーとその他の交差
MSA と PD30(MSA-C 14 例,MSA-P 15 例,PD 35 例;
反応分子も併せて定量されたためと考えられている。一
PD と MSA の鑑別に関する感度 79%,特異度 45%)
,あ
方,El-Agnaf らはオリゴマーα—シヌクレイン特異的
るいは MSA-P と MSA-C101(MSA-P 19 例,MSA-C 26 例)
ELISA 法を開発し,PD 患者では対照に比べ血漿濃度が
との間で差は認められていない。
7
運動障害の鑑別診断における神経化学的バイオマーカー
ヒポクレチン -1(オレキシン -A)
アミン代謝物
ヒポクレチン -1 は,外側視床下部ニューロンの小さな
生化学的研究によるとソマトスタチンはドパミン放出
サブセットで産生される 33 アミノ酸からなる神経ペプチ
の生化学的機構,ひいては PD の総体的症状に関与して
ドで,脳のほぼ全域に広く投射し,睡眠と覚醒の調節に
いる可能性があり 118,これを受けて PD,DLB,MSA 患
。ノックアウト
関与している(Zeitzer ら 102 の総説参照)
者の CSF におけるモノアミンとその代謝物が研究されて
マウスのデータでは,ヒポクレチン -1 の神経伝達障害と
いる。いくつかの研究で,PD および DLB(AD および対
。ナル
照と比較)におけるホモバニリン酸(homovanillic acid;
コレプシー患者ではヒポクレチン -1 ニューロン数が減少
HVA)の減少が報告されているが 119(PD 56 例,DLB 14
している 104。臨床的には,ナルコレプシー患者における
,
例,対照 34 例)120(AD 58 例,DLB 24 例;死後診断)
このニューロンの減少は CSF 中のヒポクレチン -1 濃度の
5- ヒドロキシインドール酢酸(5-hydroxyindole acetic acid;
低下を伴っており,特に脱力発作を併発する患者で著し
5-HIAA)と 3- メトキシ -4- ヒドロキシフェニルエチレン
ナルコレプシー様症状との関連が示されている
い
。このような減少は,神経変性など
103
,他の神経
105,106
107
グリコール(3-methoxy-4-hydroxyphenyl-ethylene glycol;
学的状態(例えば腫瘍および多発性硬化症)による二次
MHPG)の CSF 濃度は正常ないしわずかに低下すること
性ナルコレプシーでも認められる 106。PD では,変性変
が示されている。
化と Lewy 小体病変は視床下部領域に及ぶ 108,109。
腰椎穿刺による CSF 中のヒポクレチン -1 濃度は,ほと
イソプロスタン
んどの PD,
DLB,
MSA,
CBD 症例では正常であるが 107(PD
イソプロスタンは,フリーラジカル由来の脂質過酸化
7 例およびその他,健常対照 48 例) (PD 62 例,DLB
によって生成される安定なプロスタグランジンアイソ
13 例,CBD 7 例) (MSA-P 6 例,MSA-C 6 例,年齢を
マーで,酸化的ストレスを反映すると考えられている 121。
一致させた対照)
,PSP 患者 16 例を対象としたある研究
イソプロスタンの代謝物は尿,血漿および CSF 中に認め
。その研究で
られ,ヒト体液中のこれらの定量化は,神経変性疾患に
111
111
では,PSP では低下することが示された
110
はヒポクレチン -1 濃度は罹病期間と逆相関していたが,
おける生体内酸化ストレスを評価する上で信頼性の高い
これは PSP では特定領域に神経変性が広く分布している
基本手段になるとの仮説も提唱されている 122。AD にお
ことによると考えられた 110。
いてイソプロスタンは前臨床期や経過観察期も含め広範
に研究されているが 123,124,神経変性性シヌクレイノパ
チーに関するデータは未だにわずかしかない 125。
ニューロフィラメント
細胞骨格蛋白質の一員であるニューロフィラメント
(neurofilament; NF)はニューロンにのみ発現し,細胞の
PD,DLB,MSA,PSP,CBD で実施された CSF 蛋白
質バイオマーカーの研究の一覧を Table 1 に示す。
安定性の維持と,細胞質内粒子や細胞小器官の輸送の円
滑化を担っている。NF は,60 kDa の NF-light(NF-L)
,
100 kDa の NF-medium(NF-M)
,110 kDa の NF-heavy
(NF-H)の 3 つのサブユニットからなり,糖化,リン酸化
(phosphorylated neurofilament; NFp)などの翻訳後修飾を
複数のバイオマーカーの併用が診断精度の向上に有用
受ける。細胞質内における NF の異常な蓄積や再分布は,
であることが,最近の研究で示されている 284,285。今後も,
AD や MSA(主として NFp)112,113 および DLB や PD など,
少量の試料で様々なマーカーを同時に測定できる基本手
多くのヒト神経変性疾患で検出されている(Liu ら 114 の
段が増すにつれ,このような併用はますます一般的とな
総説参照)
。
るであろう 286。
CSF 中の NF-L(一部の研究では NFp も)は,PD や他
DLB では,ELISA 法で測定した CSF タウ蛋白質と
の神経疾患の対照に比べ MSA と PSP で増加が認めら
Aβ 1-42/Aβ 1-37 比の併用は,AD との鑑別において感度
れ
(PD 35 例,MSA 36 例,PSP 14 例) (PD 19 例,
115
116
100%,
特異度 92%であった 287。血清マーカーと CSF マー
PSP 12 例,MSA 10 例)31(PD 31 例,MSA-P 19 例,感
カーの併用に関しては,血清 H-FABP と CSF タウ蛋白質
度 76 ~ 94%,特異度 83 ~ 97%)
,DLB でも対照に比べ
の比は DLB と AD との鑑別において感度 91%,特異度
増加していた
8
複数の CSF バイオマーカーの
併用
(DLB 18 例,非神経疾患の対照 26 例)
。
117
66%であった 285。
B. Mollenhauer and C. Trenkwalder
運動障害における CSF 蛋白質バイオマーカー(具体的
サンドイッチ ELISA など,新たな方法も開発されており,
には,Aβ 1-42,NF-L,NF-H,タウ蛋白質,グリア線維
今後,血液によるバイオマーカー検査が発展する可能性
性酸性蛋白質,ニューロン特異的エノラーゼ,S100B 蛋
PD の血液トランスクリプトームマー
がある 295,296。さらに,
白質,ミエリン塩基性蛋白質,脳関連蛋白質)に関する
カーの妥当性確認の見通しは明るい 297。単核血液細胞は
最近のある総説では,鑑別診断を補助する上で,複数の
血液と脳コンパートメントとの間を行き来して脳の転写
マーカーの併用が有用であることが明らかにされた
。
287
さらに,神経画像検査,神経化学的検査,嗅覚機能検査
など,CSF によらないバイオマーカーと CSF バイオマー
カーとの併用も今後重要となる可能性がある
。
の異常状態を末梢に伝えるが 298,これは血液トランスク
リプトームに反映されることが示されている。
現時点では個々の患者でカットオフ値を決定できない
ため,CSF 解析は運動障害の臨床診断を単に補強する程
164
度である。当分の間,運動障害の CSF および血液バイオ
CSF バイオマーカー研究にお
ける交絡因子
マーカーについて,エビデンスに基づく研究はあまり出
てこないであろう。また,特に早期,さらには前臨床段
階における診断能力および予後判定能力に関し,大部分
一般に,解析前試料の取り扱いや生物学的交絡因子な
のマーカーは未だに疾患非特異的であり,さらに一部の
どのいくつかの要因がバイオマーカーの研究結果に影響
マーカーではさらなる妥当性確認が必要である。CSF 中
を与える。不適切な試料処理,遠心分離ステップ,保存
のα—シヌクレインのような有望なバイオマーカーについ
状態(- 80℃以下)
,
保存容器(ポリプロピレンを除く)は,
ては,臨床分類が同等の独立した大規模サンプルサブ
しばしば翻訳後修飾,変性および/または蛋白質喪失の
セットでの妥当性確認が必要であり,他の疾患特異的マー
原因となるが,プロテオミクスやその他のバイオマーカー
カーについても最適なコホート(剖検で疾患が証明済み)
研究では,凍結解凍サイクルの反復にも考慮する必要が
および健常対照で検討する必要がある。
ある
。標準操作手順を決めておくことが望ましい
288
。
289
謝 辞
また死後採取 CSF は,血液や死後自己融解物を混入して
いる可能性があるため(死後経過時間による)
,
バイオマー
本研究は,Dr. W. Jackstaedt Fellowship des Stifterverbandes
カー研究には推奨されない。バイオマーカー研究では試
fuer die Deutsche Wissenschaft,米国パーキンソン病協会
料の小さいサブグループを対象とする独立した検証が必
(APDA),Michael J. Fox Foundation の支援を受けた(B.M. に
要であり,マーカーと疾患との誤った関連性が検出され
対して)。
ることを避けるためには異なる研究グループによる実施
が望ましい 290。
これらの交絡因子はすべてに当てはまるわけではなく,
具体的な試料処理や保存条件はマーカー候補ごとに異な
著者の役割
B.M. は本総説の目的とデザインの策定,表の項目の選択,
原稿作成を担当した。C.T. はアイデアの提供と原稿の校閲を
担当した。
ると考えられる。
今後のバイオマーカーの展望
質量分析に基づく新たな方法論は,今後,神経変性疾
患や運動障害の新たなバイオマーカーを見出す上で役立
。
つであろう 290,291(Zetterberg288 の総説参照)
腰椎穿刺のリスクは低いが 292,将来の目標は,末梢血
で神経変性疾患の信頼性の高いバイオマーカーを見つけ
ることである。AD のバイオマーカーの領域では,AD は
他の神経変性疾患よりも開発が 10 年先行しているが,血
液バイオマーカーに関してはまだ高い成功率は得られて
いない 293,294。ただし,フィルターを用いるアレイ方式の
9
W. Jackstaedt Fellowship des Stifterverbandes fuer die Deutsche Wissenschaft, the American Parkinson Disease Association and Michael J. Fox Foundation (to B.M.).
nto account for
The definition
ptimal.289 Addibe contaminated
epending on the
ot recommended
dation in a small
ed in biomarker
nt group to avoid
d diseases.290
versally applicaconditions may
candidate.
88
ARKERS
n the basis of
new biomarkers
ement disorders
erberg288].
puncture,292 the
r for neurodegeThe biomarker
f biomarker dediseases, has not
omarkers,293,294
d, arrayed sandfacilitate bloode.295,296 Furthermic markers for
hown that monoblood and brain
of transcription
can be reflected
movement disoranalysis as cutr the individual
evidence-based
for movement
disease-nonspeespecially as far
nostic and progsing biomarkers
ed in independparative clinical
pecific markers
10
19. Hulstaert F, Blennow K, Ivanoiu A, et al. Improved discrimination of AD patients using beta-amyloid(1-42) and tau levels in
CSF. Neurology 1999;52:1555–1562.
20. Mollenhauer B, Cepek L, Bibl M, et al. Tau protein, Abeta42
Author Roles: B.M. developed the idea and the design of
and S-100B protein in cerebrospinal fluid of patients with dementia with Lewy bodies. Dement Geriatr Cogn Disord 2005;
the review, did the selection of the items in the table and
19:164–170.
wrote the manuscript. C.T. provided ideas and reviewed the
21. Paraskevas GP, Kapaki E, Liappas I, et al. The diagnostic value
manuscript.
運動障害の鑑別診断における神経化学的バイオマーカー
of cerebrospinal fluid tau protein in dementing and nondementing neuropsychiatric disorders. J Geriatr Psychiatry Neurol
2005;18:163–173.
22. Urakami K, Mori M, Wada K, et al. A comparison of tau proREFERENCES
REFERENCES
tein in cerebrospinal fluid between corticobasal degeneration
1. Trojanowski JQ, Growdon JH. A new consensus report on
and progressive supranuclear palsy. Neurosci Lett 1999;259:
biomarkers for the early antemortem diagnosis of Alzheimer
127–129.
disease: current status, relevance to drug discovery, and recom23. Itoh N, Arai H, Urakami K, et al. Large-scale, multicenter study
mendations for future research. J Neuropathol Exp Neurol 1998;
of cerebrospinal fluid tau protein phosphorylated at serine 199
57:643–644.
for the antemortem diagnosis of Alzheimer’s disease. Ann Neu2. Wiltfang J, Lewczuk P, Riederer P, et al. Consensus paper of
rol 2001;50:150–156.
the WFSBP Task Force on Biological Markers of Dementia: the
24. Otto M, Wiltfang J, Cepek L, et al. Tau protein and 14-3-3 prorole of CSF and blood analysis in the early and differential
tein in the differential diagnosis of Creutzfeldt-Jakob disease.
diagnosis of dementia. World J Biol Psychiatry 2005;6:69–84.
Neurology 2002;58:192–197.
3. Dubois B, Feldman HH, Jacova C, et al. Research criteria for
25. Mollenhauer B, Serafin S, Zerr I, et al. Diagnostic problems
the diagnosis of Alzheimer’s disease: revising the NINCDSduring late course in Creutzfeldt-Jakob disease. J Neurol 2003;
ADRDA criteria. Lancet Neurol 2007;6:734–746.
250:629–630.
4. Klunk WE, Engler H, Nordberg A, et al. Imaging brain amyloid
26. Hesse C, Rosengren L, Andreasen N, et al. Transient increase
in Alzheimer’s disease with Pittsburgh Compound-B. Ann Neuin total tau but not phospho-tau in human cerebrospinal fluid
rol 2004;55:306–319.
after acute stroke. Neurosci Lett 2001;297:187–190.
5. Seubert P, Vigo-Pelfrey C, Esch F, et al. Isolation and quantifi27. Blennow K, Wallin A, Agren H, Spenger C, Siegfried J,
cation of soluble Alzheimer’s beta-peptide from biological fluVanmechelen E. Tau protein in cerebrospinal fluid: a biochemiids. Nature 1992;359:325–327.
cal marker for axonal degeneration in Alzheimer disease? Mol
6. Motter R, Vigo-Pelfrey C, Kholodenko D, et al. Reduction of
Chem Neuropathol 1995;26:231–245.
beta-amyloid peptide42 in the cerebrospinal fluid of patients
28. Mollenhauer B, Trenkwalder C, von Ahsen N, et al. Betawith Alzheimer’s disease. Ann Neurol 1995;38:643–648.
amlyoid 1-42 and tau-protein in cerebrospinal fluid of patients
7. Reiber H. Flow rate of cerebrospinal fluid (CSF)--a concept
with Parkinson’s disease dementia. Dement Geriatr Cogn Disord
common to normal blood-CSF barrier function and to dysfunc2006;22:200–208.
tion in neurological diseases. J Neurol Sci 1994;122:189–203.
29. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines
8. Reiber H. Dynamics of brain-derived proteins in cerebrospinal
for the clinical and pathologic diagnosis of dementia with Lewy
fluid. Clin Chim Acta 2001;310:173–186.
bodies (DLB): report of the consortium on DLB international
9. Reiber H. Liquorraeume, liquorbildung und liquorfluss. In:
workshop. Neurology 1996;47:1113–1124.
Wildemann B, Reiber H, Oschmann P, editors. Neurlogische
30. Abdo WF, De Jong D, Hendriks JC, et al. Cerebrospinal fluid
Labordiagnostik. Thieme Verlag; 2006.
analysis differentiates multiple system atrophy from Parkinson’s
10. Reiber H, Peter JB. Cerebrospinal fluid analysis: disease-related
disease. Mov Disord 2004;19:571–579.
data patterns and evaluation programs. J Neurol Sci 2001;184:
31. Abdo WF, Bloem BR, Van Geel WJ, Esselink RA, Verbeek
101–122.
MM. CSF neurofilament light chain and tau differentiate multi11. Cleveland DW, Spiegelman BM, Kirschner MW. Conservation
ple system atrophy from Parkinson’s disease. Neurobiol Aging
of microtubule associated proteins. Isolation and characteriza2007;28:742–747.
tion of tau and the high molecular weight microtubule associ32. Urakami K, Wada K, Arai H, et al. Diagnostic significance of
ated protein from chicken brain and from mouse fibroblasts and
tau protein in cerebrospinal fluid from patients with corticobasal
comparison to the corresponding mammalian brain proteins.
degeneration or progressive supranuclear palsy. J Neurol Sci
J Biol Chem 1979;254:12670–12678.
2001;183:95–98.
12. Braak H, Braak E, Grundke-Iqbal I, Iqbal K. Occurrence of
33. Arai H, Morikawa Y, Higuchi M, et al. Cerebrospinal fluid
neuropil threads in the senile human brain and in Alzheimer’s
tau levels in neurodegenerative diseases with distinct tau-related
disease: a third location of paired helical filaments outside of
pathology. Biochem Biophys Res Commun 1997;236:262–264.
neurofibrillary tangles and neuritic plaques. Neurosci Lett 1986;
34. Hampel H, Goernitz A, Buerger K. Advances in the developCSF DIAGNOSTICS IN MOVEMENT
1419
65:351–355.
ment ofDISORDERS
biomarkers for Alzheimer’s disease: from CSF total
tau
13. Grundke-Iqbal I, Iqbal K, Quinlan M, Tung YC, Zaidi MS,
and Abeta(1-42) proteins to phosphorylated tau protein. Brain
Wisniewski HM. Microtubule-associated protein tau. A compoRes Bull 2003;61:243–253.
action,
intracellularpaired
trafficking
neurodegeneration.
35. Buerger K, Zinkowski R, Teipel SJ, et al. Differential diagnosis
nent
of Alzheimer
helicaland
filaments.
J Biol ChemBiochem
1986;
J 1997;323 (Part 3):577–591.
of Alzheimer disease with cerebrospinal fluid levels of tau pro261:6084–6089.
tein phosphorylated at threonine 231. Arch Neurol 2002;59:
16.Lee
Buee
L, Goedert
BussiereM,
T, Trojanowski
Buee-Scherrer
Delacourte A, Hof
PR.
14.
VM,
JQ.V,Neurodegenerative
tauoCSFandDIAGNOSTICS
IN MOVEMENT
DISORDERS
1419
1267–1272.
Tau protein
phosphorylation
role in neurodegenerpathies.
Annuisoforms,
Rev Neurosci
2001;24:1121–1159.
ative disorders.
ResRL.
BrainRegulated
Res Rev 2000;33:95–130.
36. Hu YY, He SS, Wang XC, et al. Elevated levels of phosphoryl15. Billingsley
ML, Brain
Kincaid
phosphorylation and
ated neurofilament proteins in cerebrospinal fluid of Alzheimer
17.dephosphorylation
Lee VM, Trojanowski
JQ. Neurodegenerative
tauopathies:
of tau protein:
effects on microtubule
interdisease K,
patients.
Neurosci
Lett 2002;320:156–160.
humanintracellular
disease andtrafficking
transgenicand
mouse
models. NeuronBiochem
1999;24:
action,
neurodegeneration.
35. Buerger
Zinkowski
R, Teipel
SJ, et al. Differential diagnosis
37.ofArima
K, Hirai
S, Sunohara
N, et al. Cellular
co-localization
J 507–510.
1997;323 (Part 3):577–591.
Alzheimer
disease
with cerebrospinal
fluid levels
of tau pro-of
phosphorylated
tau-at and
NACP/alpha-synuclein-epitopes
18.Buee
Andreasen
N, Minthon
L, ClarbergV,
A, Delacourte
et al. Sensitivity,
tein
phosphorylated
threonine
231. Arch Neurol 2002;59:in
16.
L, Bussiere
T, Buee-Scherrer
A, Hof speciPR.
lewy bodies in sporadic Parkinson’s disease and in dementia
ficity,
and isoforms,
stability of
CSF-tau in AD
community-based
1267–1272.
Tau
protein
phosphorylation
and in
rolea in
neurodegenerwith
Lewy
bodies.
Brain
1999;843:53–61.
patient
sample.Brain
Neurology
1999;53:1488–1494.
ative
disorders.
Res Brain
Res Rev 2000;33:95–130.
36. Hu
YY,
He SS,
Wang
XC,Res
et al.
Elevated levels of phosphoryl38.ated
Merdes
AR, Hansen
LA, Jeste
DV, et al. Influence
of Alzhei19.Lee
Hulstaert
Blennow K, JQ.
Ivanoiu
A, et al. Improvedtauopathies:
discriminaneurofilament
proteins
in cerebrospinal
fluid of Alzheimer
17.
VM, F,Trojanowski
Neurodegenerative
mer pathology
clinicalLett
diagnostic
accuracy in dementia with
tion ofdisease
AD patients
using beta-amyloid(1-42)
and tau1999;24:
levels in
disease
patients. on
Neurosci
2002;320:156–160.
human
and transgenic
mouse models. Neuron
Lewy K,
bodies.
2003;60:1586–1590.
CSF. Neurology 1999;52:1555–1562.
507–510.
37. Arima
HiraiNeurology
S, Sunohara
N, et al. Cellular co-localization of
39.phosphorylated
Parnetti L, Tiraboschi
P, Lanari
A, et al. Cerebrospinal Fluid
20.Andreasen
Mollenhauer
CepekL,L,Clarberg
Bibl M, A,
et et
al. al.
Tau
protein, Abeta42
tau- and
NACP/alpha-synuclein-epitopes
in
18.
N, B,
Minthon
Sensitivity,
speciBiomarkers
Disease with
Dementia
Demenand S-100B
proteinofinCSF-tau
cerebrospinal
patients with delewy
bodies in Parkinson’s
sporadic Parkinson’s
disease
and inand
dementia
ficity,
and stability
in ADfluid
in aofcommunity-based
tia with
Bodies.
2008;64:850–855.
mentiasample.
with Lewy
bodies.1999;53:1488–1494.
Dement Geriatr Cogn Disord 2005;
with
LewyLewy
bodies.
BrainBiol
Res Psychiatry
1999;843:53–61.
patient
Neurology
19:164–170.
40.Merdes
GlennerAR,
GG,Hansen
Wong LA,
CW,Jeste
Quaranta
V, al.
Eanes
ED. The
amyloid
38.
DV, et
Influence
of Alzhei19. Hulstaert
F, Blennow K, Ivanoiu A, et al. Improved discriminadeposits
in Alzheimer’s
their
nature in
and
pathogenesis.
21.tion
Paraskevas
GP, Kapaki
Liappas I, et al. The
mer
pathology
on clinical disease:
diagnostic
accuracy
dementia
with
of AD patients
usingE,beta-amyloid(1-42)
anddiagnostic
tau levelsvalue
in
Appl bodies.
Pathol 1984;2:357–369.
of cerebrospinal
fluid tau protein in dementing and nondementLewy
Neurology 2003;60:1586–1590.
CSF.
Neurology 1999;52:1555–1562.
ing neuropsychiatric
disorders.
Neurol
41.Parnetti
Vassar L,
R. Tiraboschi
BACE1: the
enzyme
in Alzheimer’s
39.
P, beta-secretase
Lanari A, et al.
Cerebrospinal
Fluid
20. Mollenhauer
B, Cepek L,
Bibl M, JetGeriatr
al. Tau Psychiatry
protein, Abeta42
2005;18:163–173.
disease. J Mol
Neurosci 2004;23:105–114.
Biomarkers
in Parkinson’s
Disease with Dementia and Demenand
S-100B protein in cerebrospinal fluid of patients with de22.mentia
Urakami
K, Lewy
Mori bodies.
M, Wada
K, et al.
A comparison
of tau
pro42.tiaTakasugi
N, Tomita
Hayashi
I, et2008;64:850–855.
al. The role of presenilin
with Lewy
Bodies. T,
Biol
Psychiatry
with
Dement
Geriatr
Cogn Disord
2005;
tein in cerebrospinal fluid between corticobasal degeneration
cofactors
in Wong
the gamma-secretase
complex.
Nature
19:164–170.
40. Glenner
GG,
CW, Quaranta V,
Eanes ED.
The 2003;422:
amyloid
and progressive
supranuclear
palsy.
Lett 1999;259:
438–441.
deposits
in Alzheimer’s disease: their nature and pathogenesis.
21. Paraskevas
GP, Kapaki
E, Liappas
I, et Neurosci
al. The diagnostic
value
43.Appl
Parkin
ET, 1984;2:357–369.
Trew A, Christie G, et al. Structure-activity relationPathol
of127–129.
cerebrospinal fluid tau protein in dementing and nondement23.ing
Itohneuropsychiatric
N, Arai H, Urakami
K, et al.J Large-scale,
multicenter
study
ship ofR. hydroxamate-based
inhibitorsenzyme
on theinsecretases
that
disorders.
Geriatr Psychiatry
Neurol
41. Vassar
BACE1: the beta-secretase
Alzheimer’s
of cerebrospinal fluid tau protein phosphorylated at serine 199
cleave Jthe
protein, angiotensin converting
2005;18:163–173.
disease.
Molamyloid
Neurosciprecursor
2004;23:105–114.
for the antemortem
disease.
Neuenzyme, N,
CD23,
and T,
pro-tumor
22. Urakami
K, Mori M,diagnosis
Wada K, ofet Alzheimer’s
al. A comparison
of Ann
tau pro42. Takasugi
Tomita
Hayashinecrosis
I, et al. factor-alpha.
The role of Biochemispresenilin
rol 2001;50:150–156.
try 2002;41:4972–4981.
tein
in cerebrospinal fluid between corticobasal degeneration
cofactors
in the gamma-secretase complex. Nature 2003;422:
24.and
Ottoprogressive
M, Wiltfangsupranuclear
J, Cepek L, palsy.
et al. Tau
proteinLett
and 14-3-3
pro44.438–441.
Guntert A, Dobeli H, Bohrmann B. High sensitivity analysis of
Neurosci
1999;259:
tein in the differential diagnosis of Creutzfeldt-Jakob disease.
amyloid-beta
composition
in amyloid deposits
from
127–129.
43. Parkin
ET, Trewpeptide
A, Christie
G, et al. Structure-activity
relationNeurology
human
PS2APP mouse inhibitors
brain. Neuroscience
2006;143:461–
23. Itoh
N, Arai 2002;58:192–197.
H, Urakami K, et al. Large-scale, multicenter study
ship
of and
hydroxamate-based
on the secretases
that
475. the amyloid precursor protein, angiotensin converting
25.ofMollenhauer
Serafin
Zerr phosphorylated
I, et al. Diagnostic
problems
cerebrospinalB,fluid
tau S,
protein
at serine
199
cleave
during
late course diagnosis
in Creutzfeldt-Jakob
disease.
J Neurol
2003;
45.enzyme,
Jendroska
K, Kashiwagi
M, necrosis
Sassoonfactor-alpha.
J, Daniel SE.
Amyloid
for
the antemortem
of Alzheimer’s
disease.
Ann NeuCD23,
and pro-tumor
Biochemis250:629–630.
beta-peptide
and its relationship with dementia in Lewy body
rol
2001;50:150–156.
try
2002;41:4972–4981.
disease.A,J Neural
Suppl 1997;51:137–144.
26.Otto
Hesse
Rosengren
L, Andreasen
N, protein
et al. Transient
increase
24.
M, C,
Wiltfang
J, Cepek
L, et al. Tau
and 14-3-3
pro44. Guntert
Dobeli Transm
H, Bohrmann
B. High sensitivity analysis of
in total
but not phospho-tau
human cerebrospinal
fluid
46.amyloid-beta
Perez RG, Zheng
Van der Ploeg
Koo deposits
EH. Thefrom
betatein
in thetaudifferential
diagnosis ofin Creutzfeldt-Jakob
disease.
peptideH, composition
in LH,
amyloid
after acute2002;58:192–197.
stroke. Neurosci Lett 2001;297:187–190.
amyloid
Alzheimer’s
disease2006;143:461–
enhances neuNeurology
human
andprecursor
PS2APPprotein
mouse ofbrain.
Neuroscience
38. Merdes AR, Han
mer pathology on
Lewy bodies. Neu
39. Parnetti L, Tirab
Biomarkers in Pa
tia with Lewy Bo
40. Glenner GG, Wo
deposits in Alzhe
Appl Pathol 1984
41. Vassar R. BACE
disease. J Mol Ne
42. Takasugi N, Tom
cofactors in the
438–441.
43. Parkin ET, Trew
ship of hydroxa
cleave the amyl
enzyme, CD23, a
try 2002;41:4972
44. Guntert A, Dobel
amyloid-beta pep
human and PS2A
475.
45. Jendroska K, Ka
beta-peptide and
disease. J Neural
46. Perez RG, Zheng
amyloid precurso
ron viability and
17:9407–9414.
47. Strozyk D, Blenn
levels correlate w
based autopsy stu
48. Fagan AM, Min
between in vivo
Abeta42 in huma
49. Portelius E, Zette
disease-specific b
nal fluid. Neurosc
50. Wiltfang J, Smirn
phoretic separati
beta) peptides 1527–532.
51. Lewczuk P, Essel
tion of amyloid b
25:3336–3343.
52. Wiltfang J, Esse
amyloid peptide
ease and its gen
2001;276:42645–
53. Wiltfang J, Essel
disease-specific p
peptides 1-37/38/
ease and in patie
chem 2002;81:48
54. Kanemaru K, Ka
loid beta42 and
bodies. Neurology
he diagnostic value
ng and nondementPsychiatry Neurol
mparison of tau proobasal degeneration
sci Lett 1999;259:
e, multicenter study
ylated at serine 199
disease. Ann Neu-
ein and 14-3-3 profeldt-Jakob disease.
Diagnostic problems
ase. J Neurol 2003;
Transient increase
cerebrospinal fluid
87–190.
er C, Siegfried J,
l fluid: a biochemieimer disease? Mol
en N, et al. Betanal fluid of patients
Geriatr Cogn Disord
onsensus guidelines
ementia with Lewy
DLB international
Cerebrospinal fluid
hy from Parkinson’s
elink RA, Verbeek
differentiate multie. Neurobiol Aging
ostic significance of
ts with corticobasal
alsy. J Neurol Sci
Cerebrospinal fluid
distinct tau-related
997;236:262–264.
ces in the developfrom CSF total tau
tau protein. Brain
system atrophy: a new alpha-synuclein disease? Lancet 1998;
40. Glenner GG, Wong CW, Quaranta V, Eanes ED. The amyloid
352:547–548.
deposits in Alzheimer’s disease: their nature and pathogenesis.
62. Polymeropoulos MH, Lavedan C, Leroy E, et al. Mutation in
Appl Pathol 1984;2:357–369.
the alpha-synuclein gene identified in families with Parkinson’s
41. Vassar R. BACE1: the beta-secretase enzyme in Alzheimer’s
disease. Science 1997;276:2045–2047.
disease. J Mol Neurosci 2004;23:105–114.
63. Kruger R, Kuhn W, Muller T, et al. Ala30Pro mutation in the
42. Takasugi N, Tomita T, Hayashi I, et al. The role of presenilin
gene encoding alpha-synuclein in Parkinson’s disease. Nat
cofactors in the gamma-secretase complex. Nature 2003;422:
Genet 1998;18:106–108.
438–441.
B. Mollenhauer
C. Trenkwalder
64. Zarranz JJ, Alegre J, Gomez-Esteban
JC, etand
al. The
new muta43. Parkin ET, Trew A, Christie G, et al. Structure-activity relationtion, E46K, of alpha-synuclein causes Parkinson and Lewy
ship of hydroxamate-based inhibitors on the secretases that
body dementia. Ann Neurol 2004;55:164–173.
cleave the amyloid precursor protein, angiotensin converting
enzyme, CD23, and pro-tumor necrosis factor-alpha. Biochemis65. Chartier-Harlin M-C, Kachergus J, Roumier C, et al. Alpha-syntry 2002;41:4972–4981.
uclein locus duplication as a cause of familial Parkinson’s disease. The Lancet 2004;364:1167–1169.
44. Guntert A, Dobeli H, Bohrmann B. High sensitivity analysis of
66. Singleton AB, Farrer M, Johnson J, et al. alpha-Synuclein locus
amyloid-beta peptide composition in amyloid deposits from
human and PS2APP mouse brain. Neuroscience 2006;143:461–
triplication causes Parkinson’s disease. Science 2003;302(5646):
475.
841.
67. Cookson MR. The biochemistry of Parkinson’s disease. Annu
45. Jendroska K, Kashiwagi M, Sassoon J, Daniel SE. Amyloid
Rev Biochem 2005;74:29–52.
beta-peptide and its relationship with dementia in Lewy body
disease. J Neural Transm Suppl 1997;51:137–144.
68. Outeiro TF, Lindquist S. Yeast cells provide insight into alpha46. Perez RG, Zheng H, Van der Ploeg LH, Koo EH. The betasynuclein biology and pathobiology. Science 2003;302:1772–1775.
amyloid precursor protein of Alzheimer’s disease enhances neu69. Conway KA, Lee SJ, Rochet JC, Ding TT, Williamson RE,
ron viability and modulates neuronal polarity. J Neurosci 1997;
Lansbury PT, Jr. Acceleration of oligomerization, not fibrilliza17:9407–9414.
tion, is a shared property of both alpha-synuclein mutations
47. Strozyk D, Blennow K, White LR, Launer LJ. CSF Abeta 42
linked to early-onset Parkinson’s disease: implications for
levels correlate with amyloid-neuropathology in a populationpathogenesis and therapy. Proc Natl Acad Sci USA 2000;97:
571–576.
based autopsy study. Neurology 2003;60:652–656.
70. Anderson JP, Walker DE, Goldstein JM, et al. Phosphorylation
48. Fagan AM, Mintun MA, Mach RH, et al. Inverse relation
between in vivo amyloid imaging load and cerebrospinal fluid
of Ser 129 is the dominant pathological modification of alpha Abeta42 in humans. Ann Neurol 2006;59:512–519.
synuclein in familial and sporadic Lewy body disease. J Biol
Chem 2006;281:29739–29752.
49. Portelius E, Zetterberg H, Andreasson U, et al. An Alzheimer’s
71. Cuervo AM, Stefanis L, Fredenburg R, Lansbury PT, Sulzer D.
disease-specific beta-amyloid fragment signature in cerebrospiImpaired degradation of mutant alpha-synuclein by chaperonenal fluid. Neurosci Lett 2006;409:215–219.
mediated autophagy. Science 2004;305:1292–1295.
50. Wiltfang J, Smirnov A, Schnierstein B, et al. Improved electro72. Shin Y, Klucken J, Patterson C, Hyman BT, McLean PJ. The
phoretic separation and immunoblotting of beta-amyloid (A
co-chaperone carboxyl terminus of hsp70-interacting protein
beta) peptides 1-40, 1-42, and 1-43. Electrophoresis 1997;18:
(CHIP) mediates {alpha}-synuclein degradation decisions
527–532.
between proteasomal and lysosomal pathways. J Biol Chem
51. Lewczuk P, Esselmann H, Bibl M, et al. Electrophoretic separa2005;280:23727–23734.
tion of amyloid beta peptides in plasma. Electrophoresis 2004;
73. Lee HJ, Patel S, Lee SJ. Intravesicular localization and exocyto25:3336–3343.
sis of alpha-synuclein and its aggregates. J Neurosci 2005;25:
52. Wiltfang J, Esselmann H, Cupers P, et al. Elevation of beta6016–6024.
amyloid peptide 2-42 in sporadic and familial Alzheimer’s disease and its generation in PS1 knockout cells. J Biol Chem
74. El-Agnaf OM, Salem SA, Paleologou KE, et al. Alpha-synu1420
B. MOLLENHAUER AND C. TRENKWALDER
2001;276:42645–42657.
clein implicated in Parkinson’s disease is present in extracellular biological fluids, including human plasma. FASEB J 2003;
53. Wiltfang J, Esselmann H, Bibl M, et al. Highly conserved and
17:1945–1947.
disease-specific patterns of carboxyterminally truncated Abeta
55.peptides
Holmberg
B, Johnels
Blennow
K, Rosengren
L. Cerebrospi75. van Geel WJ, Abdo WF, Melis R, Williams S, Bloem BR, Ver1-37/38/39
in B,
addition
to 1-40/42
in Alzheimer’s
disnal fluid
Abeta42
reduced
in multiple
system atrophy
but norbeek MM. A more efficient enzyme-linked immunosorbent
ease
and in
patientsis with
chronic
neuroinflammation.
J Neuromal in
Parkinson’s disease and progressive supranuclear palsy.
assay for measurement of alpha-synuclein in cerebrospinal fluid.
chem
2002;81:481–496.
1420
Mov Disord
J Neurosci Methods 2008;168:182–185.
54. Kanemaru
K, 2003;18:186–190.
Kameda N, YamanouchiB.H.MOLLENHAUER
Decreased CSF amy- AND C. TRENKWALDER
Movement
Disorders,
24, No.K,
10,Jensen
2009 PH. Determination of alpha56.loid
Noguchi
Yoshita
Ono K,
Iwasa
76. Fjorback
AW,Vol.
Varming
beta42M,and
normalM,tauMatsumoto
levels in Y,
dementia
with
LewyK,
Yamada
M. Decreased
b-amyloid peptide42 in cerebrospinal
synuclein concentration in human plasma using ELISA. Scand J
bodies.
Neurology
2000;54:1875–1876.
fluid of patients
withB,progressive
supranuclear
and corti55. Holmberg
B, Johnels
Blennow K,
Rosengren palsy
L. CerebrospiClinGeel
LabWJ,
Invest
2007;67:431–435.
75. van
Abdo
WF, Melis R, Williams S, Bloem BR, Vercobasal
degeneration.
J Neurol
Sci 2005;237:61–65.
nal
fluid Abeta42
is reduced
in multiple
system atrophy but norMM.
moreSA,efficient
immunosorbent
77.beek
Tokuda
T, A
Salem
Allsop enzyme-linked
D, et al. Decreased
alpha-synuin Parkinson’s
disease
and progressive
palsy.
assay
alpha-synuclein
in cerebrospinal
fluid.
cleinfor
in measurement
cerebrospinaloffluid
of aged individuals
and subjects
57.mal
Mollenhauer
B, Bibl
M, Esselmann
H, et supranuclear
al. Tauopathies
and
Mov
Disord 2003;18:186–190.
J with
Neurosci
Methodsdisease.
2008;168:182–185.
synucleinopathies:
Do cerebrospinal fluid beta-amyloid peptides
Parkinson’s
Biochem Biophys Res Commun 2006;
Movement
Disorders,
Vol. 24,
No.
10, 2007;
2009
reflect disease-specific
JY,Neural
Transm
56. Noguchi
M, Yoshita M,pathogenesis?
Matsumoto
Ono
K,
Iwasa
K,
349:162–166.
76. Fjorback
AW, Varming K, Jensen PH. Determination of alpha114:919–927.
Yamada
M. Decreased b-amyloid peptide42 in cerebrospinal
concentration
plasma
Scand Jof
78.synuclein
Mollenhauer
B, CulleninV,human
Kahn I,
et al. using
DirectELISA.
quantification
with progressive
palsy andofcorti58.fluid
BiblofM,patients
Mollenhauer
B, Lewczuksupranuclear
P, et al. Validation
amyClin
Invest 2007;67:431–435.
CSFLab
alpha-synuclein
by ELISA and first cross-sectional study
cobasal
degeneration.
2005;237:61–65.
in patients
with neurodegeneration.
ExpDecreased
Neurol 2008;213:315–
loid-beta
peptides JinNeurol
CSF Sci
diagnosis
of neurodegenerative
77. Tokuda
T, Salem
SA, Allsop D, et al.
alpha-synudementias. Mol
Psychiatry
2007;12:671–680.
clein
57. Mollenhauer
B, Bibl
M, Esselmann
H, et al. Tauopathies and
325. in cerebrospinal fluid of aged individuals and subjects
Do cerebrospinal
peptides
59.synucleinopathies:
Bibl M, Mollenhauer
B, Esselmann fluid
H, etbeta-amyloid
al. CSF amyloid-betaParkinson’s
disease.
Biochem
Reslength
Commun
2006;
79.with
Borghi
R, Marchese
R, Negro
A, Biophys
et al. Full
alpha-synureflect
disease-specific
pathogenesis?
J Neural
peptides
in Alzheimer’s
disease, dementia
withTransm
Lewy 2007;
bodies
349:162–166.
clein is present in cerebrospinal fluid from Parkinson’s disease
114:919–927.
and Parkinson’s disease dementia. Brain 2006;129 (Part 5):
and normal B,
subjects.
78. Mollenhauer
CullenNeurosci
V, KahnLett
I, et2000;287:65–67.
al. Direct quantification of
58. Bibl
M, Mollenhauer B, Lewczuk P, et al. Validation of amy1177–1187.
alpha-synuclein
by Andreasen
ELISA andN,first
cross-sectional
80.CSF
Ohrfelt
A, Grognet P,
et al.
Cerebrospinalstudy
fluid
inalpha-synuclein
patients with neurodegeneration.
Exp Neurol
2008;213:315–
in CSF
neurodegenerative
60.loid-beta
Spillantinipeptides
MG, Schmidt
ML,diagnosis
Lee VM, of
Trojanowski
JQ, Jakes
in neurodegenerative
disorders-A
marker of
dementias.
Mol
2007;12:671–680.
R, Goedert
M.Psychiatry
Alpha-synuclein
in Lewy bodies. Nature 1997;
325.
synapse loss? Neurosci Lett 2008;450:332–335.
388:839–840.
59. Bibl
M, Mollenhauer B, Esselmann H, et al. CSF amyloid-beta79.
R, Marchese I,R,Klucken
Negro A,
et al. FullM,
length
81.Borghi
Cantuti-Castelvetri
J, Ingelsson
et al. alpha-synuAlpha-synuAlzheimer’s
disease, dementia
with WW.
LewyMultiplebodies
clein
present
in cerebrospinal
Parkinson’s
disease
cleinisand
chaperones
in dementiafluid
withfrom
Lewy
bodies. J Neuropa61.peptides
Gai WP,in Power
JH, Blumbergs
PC, Blessing
and
Parkinson’s
dementia. Braindisease?
2006;129
(Part1998;
5):
and
subjects.
Neurosci Lett 2000;287:65–67.
system
atrophy: disease
a new alpha-synuclein
Lancet
tholnormal
Exp Neurol
2005;64:1058–1066.
1177–1187.
352:547–548.
80.
A, Humbert
Grognet P,
Andreasen
al. Cerebrospinal
82.Ohrfelt
Beyer K,
J, Ferrer
A, etN,al.etLow
alpha-synucleinfluid
126
60.
MG, Schmidt
ML, Lee
Trojanowski
JQ, Jakesin
62.Spillantini
Polymeropoulos
MH, Lavedan
C,VM,
Leroy
E, et al. Mutation
alpha-synuclein
neurodegenerative
disorders-A
marker disof
mRNA levels inindementia
with Lewy bodies
and Alzheimer
R,theGoedert
M. Alpha-synuclein
in Lewy
bodies.with
Nature
1997;
synapse
loss? Neurosci
Lett 2008;450:332–335.
ease. Neuroreport
2006;17:1327–1330.
alpha-synuclein
gene identified
in families
Parkinson’s
388:839–840.
disease. Science 1997;276:2045–2047.
81.
I, Klucken J, Ingelsson
et al. plexus:
Alpha-synu83.Cantuti-Castelvetri
Chodobski A, Szmydynger-Chodobska
J. M,
Choroid
target
clein
and chaperones
dementia
with
Lewy bodies.
J Neuropa61.
WP, R,Power
Multiple63.Gai
Kruger
KuhnJH,
W, Blumbergs
Muller T, etPC,
al. Blessing
Ala30ProWW.
mutation
in the
for polypeptides
andinsite
of their
synthesis.
Microsc
Res Tech
system
atrophy: aalpha-synuclein
new alpha-synuclein
disease? Lancet
1998;
gene encoding
in Parkinson’s
disease.
Nat
thol
Exp Neurol 2005;64:1058–1066.
2001;52:65–82.
352:547–548.
Genet 1998;18:106–108.
82.
K, Humbert
J, Ferrer
A, etOY,
al. Joo
LowIS,alpha-synuclein
126
84.Beyer
Lee PH,
Lee G, Park
HJ, Bang
Huh K. The plasma
62.
MH,J, Lavedan
C, Leroy
Mutation
in
mRNA
levels in dementia
Lewy
bodies
and Alzheimer
alpha-synuclein
levels in with
patients
with
Parkinson’s
diseasedisand
64.Polymeropoulos
Zarranz JJ, Alegre
Gomez-Esteban
JC,E,etetal.al.The
new mutaease.
Neuroreport
2006;17:1327–1330.
the
alpha-synuclein
gene identified causes
in families
with Parkinson’s
tion,
E46K, of alpha-synuclein
Parkinson
and Lewy
multiple
system atrophy.
J Neural Transm 2006;113:1435–1439.
disease.
Science 1997;276:2045–2047.
body dementia.
Ann Neurol 2004;55:164–173.
83.
A, SS,
Szmydynger-Chodobska
Choroid
plexus: targetis
85.Chodobski
Li QX, Mok
Laughton KM, et al. J.Plasma
alpha-synuclein
63.
R, Kuhn M-C,
W, Muller
T, et J,al.Roumier
Ala30Pro
in the
for
polypeptides
and sitewith
of their
synthesis.disease.
MicroscExp
Res Neurol
Tech
decreased
in subjects
Parkinson’s
65.Kruger
Chartier-Harlin
Kachergus
C, mutation
et al. Alpha-syngene
alpha-synuclein
in of
Parkinson’s
disease. Nat
2001;52:65–82.
2007;204:583–588.
ucleinencoding
locus duplication
as a cause
familial Parkinson’s
disGenet
ease. 1998;18:106–108.
The Lancet 2004;364:1167–1169.
84.
PH, LeeOM,
G, Park
HJ,SA,
Bang
OY, Joo IS,
K. The
plasmaof
86.Lee
El-Agnaf
Salem
Paleologou
KE,Huh
et al.
Detection
alpha-synuclein
levels
in patients with protein
Parkinson’s
diseaseplasma
and
64.
JJ, AB,
Alegre
J, Gomez-Esteban
al. The new muta66.Zarranz
Singleton
Farrer
M, Johnson J, etJC,al.etalpha-Synuclein
locus
oligomeric forms
of alpha-synuclein
in human
tion,
E46K, causes
of alpha-synuclein
causes Science
Parkinson
and Lewy
multiple
system atrophy.
J Neural
2006;113:1435–1439.
as a potential
biomarker
for Transm
Parkinson’s
disease. FASEB J
triplication
Parkinson’s disease.
2003;302(5646):
body
841.dementia. Ann Neurol 2004;55:164–173.
85. Li2006;20:419–425.
QX, Mok SS, Laughton KM, et al. Plasma alpha-synuclein is
with Parkinson’s
Exp Neurol
65.
Kachergus J, Roumier
C, et al.disease.
Alpha-syn87.decreased
GuillaumeinE,subjects
Zimmermann
C, Burkhard disease.
PR, Hochstrasser
DF,
67.Chartier-Harlin
Cookson MR. M-C,
The biochemistry
of Parkinson’s
Annu
2007;204:583–588.
uclein
locus duplication
as a cause of familial Parkinson’s disRev Biochem
2005;74:29–52.
Sanchez JC. A potential cerebrospinal fluid and plasmatic
The TF,
Lancet
2004;364:1167–1169.
marker for
theSalem
diagnosis
Creutzfeldt-Jakob
Proteo86. El-Agnaf
OM,
SA, of
Paleologou
KE, et al.disease.
Detection
of
68.ease.
Outeiro
Lindquist
S. Yeast cells provide insight into alpha66. Singleton
Farrer
Johnson J, et
al. alpha-Synuclein
locus
mics 2003;3:1495–1499.
oligomeric
forms of alpha-synuclein protein in human plasma
synucleinAB,
biology
andM,
pathobiology.
Science
2003;302:1772–1775.
a potential
biomarker
for EH,
Parkinson’s
disease.
J
causes
disease.
Science
88.asHeuckeroth
RO,
Birkenmeier
Levin MS,
GordonFASEB
JI. Analy69.triplication
Conway KA,
LeeParkinson’s
SJ, Rochet
JC, Ding
TT, 2003;302(5646):
Williamson RE,
2006;20:419–425.
841.
sis of the tissue-specific expression, developmental regulation,
Lansbury PT, Jr. Acceleration of oligomerization, not fibrillizaand linkage
rodent gene
heart DF,
fatty
87. Guillaume
E, relationships
ZimmermannofC,a Burkhard
PR,encoding
Hochstrasser
67. Cookson
The biochemistry
of Parkinson’s
disease.
Annu
tion, is MR.
a shared
property of both
alpha-synuclein
mutations
Rev
Biochem
2005;74:29–52.
acid binding
J Biolcerebrospinal
Chem 1987;262:9709–9717.
Sanchez
JC. protein.
A potential
fluid and plasmatic
linked
to early-onset
Parkinson’s disease: implications for
the Hermens
diagnosis WT,
of Creutzfeldt-Jakob
disease. Proteo89.marker
Pelsersfor
MM,
Glatz JF. Fatty acid-binding
propathogenesis
and therapy.
Proccells
Natl
Acad insight
Sci USA
68. Outeiro
TF, Lindquist
S. Yeast
provide
into2000;97:
alphamics
teins2003;3:1495–1499.
as plasma markers of tissue injury. Clin Chim Acta 2005;
571–576.biology and pathobiology. Science 2003;302:1772–1775.
synuclein
352:15–35.RO, Birkenmeier EH, Levin MS, Gordon JI. Analy88. Heuckeroth
70.Conway
Anderson
JP, Lee
Walker
Goldstein
JM, TT,
et al.Williamson
Phosphorylation
69.
KA,
SJ, DE,
Rochet
JC, Ding
RE,
thol Exp Neurol 2
82. Beyer K, Humbe
mRNA levels in d
ease. Neuroreport
83. Chodobski A, Szm
for polypeptides
2001;52:65–82.
84. Lee PH, Lee G, P
alpha-synuclein l
multiple system at
85. Li QX, Mok SS,
decreased in sub
2007;204:583–58
86. El-Agnaf OM, S
oligomeric forms
as a potential b
2006;20:419–425
87. Guillaume E, Zim
Sanchez JC. A
marker for the d
mics 2003;3:1495
88. Heuckeroth RO, B
sis of the tissueand linkage relati
acid binding prote
89. Pelsers MM, Her
teins as plasma m
352:15–35.
90. Veerkamp JH, Zi
nervous tissue. J
151–137.
91. Steinacker P, Mo
binding protein a
nerative diseases.
92. Wada-Isoe K, Im
K. Serum heart-fa
Lewy body diseas
93. Mollenhauer B, S
fatty acid-binding
candidates for de
2007;4:366–375.
94. Arimoto T, Take
damage relates t
patients with hear
95. Kligman D, Hilt
Sci 1988;13:437–
11
nson’s disease. Nat
t al. The new mutaarkinson and Lewy
73.
C, et al. Alpha-synilial Parkinson’s dis-
lpha-Synuclein locus
nce 2003;302(5646):
son’s disease. Annu
de insight into alpha2003;302:1772–1775.
TT, Williamson RE,
zation, not fibrilliza-synuclein mutations
e: implications for
d Sci USA 2000;97:
t al. Phosphorylation
odification of alpha body disease. J Biol
nsbury PT, Sulzer D.
uclein by chaperone2–1295.
BT, McLean PJ. The
0-interacting protein
gradation decisions
ways. J Biol Chem
lization and exocytoJ Neurosci 2005;25:
, et al. Alpha-synupresent in extracelluma. FASEB J 2003;
12
and other hypersomnias. Arch Neurol 2002;59:1553–1562.
2001;52:65–82.
107. Ripley B, Overeem S, Fujiki N, et al. CSF hypocretin/orexin
84. Lee PH, Lee G, Park HJ, Bang OY, Joo IS, Huh K. The plasma
levels in narcolepsy and other neurological conditions. Neurolalpha-synuclein levels in patients with Parkinson’s disease and
ogy 2001;57:2253–2258.
multiple system atrophy. J Neural Transm 2006;113:1435–1439.
108. Jellinger KA. The pathology of Parkinson’s disease. Adv Neurol
85. Li QX, Mok SS, Laughton KM, et al. Plasma alpha-synuclein is
2001;86:55–72.
decreased in subjects with Parkinson’s disease. Exp Neurol
2007;204:583–588.
109. Langston JW, Forno LS. The hypothalamus in Parkinson disease. Ann Neurol 1978;3:129–133.
86. El-Agnaf OM, Salem SA, Paleologou KE, et al. Detection of
運動障害の鑑別診断における神経化学的バイオマーカー
110. Yasui K, Inoue Y, Kanbayashi T, Nomura T, Kusumi M, Nakaoligomeric forms of alpha-synuclein protein in human plasma
shima K. CSF orexin levels of Parkinson’s disease, dementia
as a potential biomarker for Parkinson’s disease. FASEB J
2006;20:419–425.
with Lewy bodies, progressive supranuclear palsy and corticobasal degeneration. J Neurol Sci 2006;250:120–123.
87. Guillaume E, Zimmermann C, Burkhard PR, Hochstrasser DF,
111. Abdo WF, Bloem BR, Kremer HP, Lammers GJ, Verbeek MM,
Sanchez JC. A potential cerebrospinal fluid and plasmatic
Overeem S. CSF hypocretin-1 levels are normal in multiple-sysmarker for the diagnosis of Creutzfeldt-Jakob disease. Proteotem atrophy. Parkinsonism Relat Disord 2008;14:342–344.
mics 2003;3:1495–1499.
88. Heuckeroth RO, Birkenmeier EH, Levin MS, Gordon JI. Analy112. Sternberger NH, Sternberger LA, Ulrich J. Aberrant neurofilasis of the tissue-specific expression, developmental regulation,
ment phosphorylation in Alzheimer disease. Proc Natl Acad Sci
and linkage relationships of a rodent gene encoding heart fatty
USA 1985;82:4274–4276.
acid binding protein. J Biol Chem 1987;262:9709–9717.
113. Yazawa I, Giasson BI, Sasaki R, et al. Mouse model of multiple
89. Pelsers MM, Hermens WT, Glatz JF. Fatty acid-binding prosystem atrophy alpha-synuclein expression in oligodendrocytes
teins as plasma markers of tissue injury. Clin Chim Acta 2005;
causes glial and neuronal degeneration. Neuron 2005;45:847–
352:15–35.
859.
114. Liu Q, Xie F, Siedlak SL, et al. Neurofilament proteins in
90. Veerkamp JH, Zimmerman AW. Fatty acid-binding proteins of
neurodegenerative diseases. Cell Mol Life Sci 2004;61:3057–
nervous tissue. J Mol Neurosci 2001;16:133–142; discussion
151–137.
3075.
91. Steinacker P, Mollenhauer B, Bibl M, et al. Heart fatty acid
115. Holmberg B, Johnels B, Ingvarsson P, Eriksson B, Rosengren
binding protein as a potential diagnostic marker for neurodegeL. CSF-neurofilament and levodopa tests combined with discriminant analysis may contribute to the differential diagnosis
nerative diseases. Neurosci Lett 2004;370:36–39.
of Parkinsonian syndromes. Parkinsonism Relat Disord 2001;8:
92. Wada-Isoe K, Imamura K, Kitamaya M, Kowa H, Nakashima
23–31.
K. Serum heart-fatty acid binding protein levels in patients with
Lewy body disease. J Neurol Sci 2008;266:20–24.
116. Holmberg B, Rosengren L, Karlsson JE, Johnels B. Increased
DISORDERS
1421
cerebrospinal
fluid levels of neurofilament protein in progressive
93. Mollenhauer B, Steinacker P, Bahn CSF
E, et DIAGNOSTICS
al. Serum heart-typeIN MOVEMENT
supranuclear palsy and multiple-system atrophy compared with
fatty acid-binding protein and cerebrospinal fluid tau: marker
Parkinson’s disease. Mov Disord 1998;13:70–77.
candidates for dementia with Lewy bodies. Neurodegener Dis
96.2007;4:366–375.
Bloomfield SM, McKinney J, Smith L, Brisman J. Reliability of
117. de Jong D, Jansen RW, Pijnenburg YA, et al. CSF neurofilaS100B in
severity
central
injury.
ment proteins in the differential diagnosis of dementia. J Neurol
94. Arimoto
T, predicting
Takeishi Y,
Niizekiof T,
et al.nervous
Ongoingsystem
myocardial
Neurocrit
Care to
2007;6:121–138.
Neurosurg Psychiatry 2007;78:936–938.
damage
relates
cardiac sympathetic nervous disintegrity in
IN MOVEMENT
DISORDERS
1421
97.patients
Shashoua
Hesse
GW,
BW.DIAGNOSTICS
Proteins of the brain
118. Chesselet
MF, Reisine TD. Somatostatin regulates dopamine
withVE,
heart
failure.
AnnMoore
NuclCSF
Med
2005;19:535–540.
extracellular
fluid:
forprotein
releasefamily.
of S-100
protein.
J Neurelease in rat striatal slices and cat caudate nuclei. J Neurosci
95. Kligman
D, Hilt
DC.evidence
The S100
Trends
Biochem
rochem
1984;42:1536–1541.
1983;3:232–236.
Sci
1988;13:437–443.
98.Bloomfield
Berger RP,SM,
Pierce
MC, Wisniewski
et al.J.Neuron-specific
119.deKanemaru
Yamanouchi
H. Assessment
96.
McKinney
J, Smith L,SR,
Brisman
Reliability of
117.
Jong D, K,
Jansen
RW, Pijnenburg
YA, etofal.CSF
CSFhomovanillic
neurofilaenolaseinand
S100B in
cerebrospinal
fluid
after severe
acid proteins
levels in
distinguishes
dementia
withof dementia.
Lewy bodies
from
S100B
predicting
severity
of central
nervous
systemtraumatic
injury.
ment
the differential
diagnosis
J Neurol
brain injury
infants and children. Pediatrics 2002;109:E31.
Alzheimer’s
disease. 2007;78:936–938.
J Neurol 2002;249:1125–1126.
Neurocrit
Carein2007;6:121–138.
Neurosurg
Psychiatry
99.Shashoua
Maeck L,VE,
Meller
J, Otto
Stiens
G, Proteins
Wiltfang ofJ, the
Stoppe
120.Chesselet
Weiner MF,
RC,TD.
Cullum
CM, et al.regulates
Alzheimer’s
disease
97.
Hesse
GW, M,
Moore
BW.
brainG.
118.
MF,Risser
Reisine
Somatostatin
dopamine
Abeta peptide
1-42,
Tau protein
and ofS-100B
protein level
and itsinLewy
body variant:
a clinical
analysis
of Jpostmortem
extracellular
fluid:
evidence
for release
S-100 protein.
J Neu-in
release
rat striatal
slices and
cat caudate
nuclei.
Neurosci
cerebrospinal
fluid of three patients with primary progressive
verified cases. Am J Psychiatry 1996;153:1269–1273.
rochem
1984;42:1536–1541.
1983;3:232–236.
aphasia.
Neurosci
121.Kanemaru
Awad JA,K,Morrow
JD, Takahashi
K, Roberts
LJ,homovanillic
2nd. Identifi98. Berger
RP,
Pierce Lett
MC, 2002;333:33–36.
Wisniewski SR, et al. Neuron-specific
119.
Yamanouchi
H. Assessment
of CSF
100.enolase
Sussmuth
Tumani
H, Ecker D,fluid
Ludolph
Amyotrophic
cation
of non-cyclooxygenase-derived
(F2-isoprosandSD,
S100B
in cerebrospinal
after AC.
severe
traumatic
acid
levels
distinguishes dementia withprostanoid
Lewy bodies
from
lateral
sclerosis:
disease
stage related
changes
of tau protein
tane) metabolites
human 2002;249:1125–1126.
urine and plasma. J Biol Chem
brain
injury
in infants
and children.
Pediatrics
2002;109:E31.
Alzheimer’s
disease.inJ Neurol
and S100
beta inJ,cerebrospinal
fluidG,and
creatineJ,kinase
se1993;268:4161–4169.
99. Maeck
L, Meller
Otto M, Stiens
Wiltfang
Stoppein G.
120. Weiner
MF, Risser RC, Cullum CM, et al. Alzheimer’s disease
rum. Neurosci
Lett 2003;353:57–60.
122.and
Montine
TJ, body
Markesbery
Morrow
JD, Roberts
LJ, 2nd.
Abeta
peptide 1-42,
Tau protein and S-100B protein level in
its Lewy
variant:WR,
a clinical
analysis
of postmortem
101.cerebrospinal
Abdo WF, van
BP,with
Kremer
HP, progressive
Bloem BR,
Cerebrospinal
fluid
F2-isoprostane
levels are increased in
fluiddeofWarrenburg
three patients
primary
verified
cases. Am
J Psychiatry
1996;153:1269–1273.
VerbeekNeurosci
MM. CSF
biomarker profiles do not differentiate
Alzheimer’s
disease.
Neurol 1998;44:410–413.
aphasia.
Lett 2002;333:33–36.
121. Awad
JA, Morrow
JD,Ann
Takahashi
K, Roberts LJ, 2nd. Identifibetween the
andEcker
parkinsonian
phenotypes
of multiple
123.cation
de Leon
Mosconi L, Li J, et al. Longitudinal
CSF isopros100. Sussmuth
SD,cerebellar
Tumani H,
D, Ludolph
AC. Amyotrophic
of MJ,
non-cyclooxygenase-derived
prostanoid (F2-isoprossystemsclerosis:
atrophy. Parkinsonism
Disord
2007;13:480–482.
tane and
MRI atrophy
in the urine
progression
to AD. J Neurol
2007;
lateral
disease stage Relat
related
changes
of tau protein
tane)
metabolites
in human
and plasma.
Biol Chem
102.and
Zeitzer
S, Mignot fluid
E. The
neurobiology
of hypocre254:1666–1675.
S100JM,
betaNishino
in cerebrospinal
and
creatine kinase
in se1993;268:4161–4169.
tins Neurosci
(orexins),Lett
narcolepsy
and related therapeutic interventions.
124.Montine
RingmanTJ,JM,
Younkin WR,
SG, Morrow
Pratico D,
al. Biochemical
rum.
2003;353:57–60.
122.
Markesbery
JD, etRoberts
LJ, 2nd.
Trends
Pharmacol
2006;27:368–374.
markers in persons
preclinical familial
Alzheimer
disease.
101. Abdo
WF,
van de Sci
Warrenburg
BP, Kremer HP, Bloem BR,
Cerebrospinal
fluid with
F2-isoprostane
levels are
increased
in
103.Verbeek
ChemelliMM.
RM, CSF
Williebiomarker
JT, Sinton
CM, do
et al.
Neurology 2008;71:85–92.
profiles
not Narcolepsy
differentiatein
Alzheimer’s
disease. Ann Neurol 1998;44:410–413.
orexin knockout
mice:and
molecular
genetics
of sleepofregulation.
125.deConnolly
J, Mosconi
Siderowf L,
A,LiClark
Mu D, Pratico
F2 isobetween
the cerebellar
parkinsonian
phenotypes
multiple
123.
Leon MJ,
J, et CM,
al. Longitudinal
CSFD.isoprosCell 1999;98:437–451.
prostane
levels
in plasma
urine dotonot
increased
system
atrophy. Parkinsonism Relat Disord 2007;13:480–482.
tane
and MRI
atrophy
in the and
progression
AD.support
J Neurol
2007;
104.Zeitzer
Thannickal
TC, Moore
RY, Nienhuis
R, et al. Reduced
number
lipid peroxidation in cognitively impaired Parkinson disease
102.
JM, Nishino
S, Mignot
E. The neurobiology
of hypocre254:1666–1675.
of hypocretin
neurons inand
human
narcolepsy.
Neuron
2000;27:
patients. Cogn
Behav Neurol
tins
(orexins), narcolepsy
related
therapeutic
interventions.
124. Ringman
JM, Younkin
SG, 2008;21:83–86.
Pratico D, et al. Biochemical
469–474.
126.markers
Welch MJ,
Markham
CH,
Jenden DJ.
Acetylcholine
anddisease.
choline
Trends
Pharmacol Sci 2006;27:368–374.
in persons
with
preclinical
familial
Alzheimer
105.Chemelli
Nishino S,
Ripley
B, Overeem
S, etCM,
al. Low
in cerebrospinal
fluid of patients with Parkinson’s disease and
103.
RM,
Willie
JT, Sinton
et al.cerebrospinal
Narcolepsy fluid
in
Neurology
2008;71:85–92.
hypocretin
(Orexin)
altered energy
in human
Huntington’s
chorea. A,
J Neurol
Neurosurg
orexin
knockout
mice:and
molecular
geneticshomeostasis
of sleep regulation.
125. Connolly
J, Siderowf
Clark CM,
Mu D, Psychiatry
Pratico D. 1976;39:
F2 isonarcolepsy.
Ann Neurol 2001;50:381–388.
367–374.levels in plasma and urine do not support increased
Cell
1999;98:437–451.
prostane
106.Thannickal
Mignot E, TC,
Lammers
Ripley
B, etR,
al.etThe
of cerebrospi127.lipid
Manyam
BV, Giacobini
E, Colliver
JA. Cerebrospinal
fluid
104.
MooreGJ,
RY,
Nienhuis
al. role
Reduced
number
peroxidation
in cognitively
impaired
Parkinson disease
fluid hypocretin
in the diagnosis
of narcolepsy
choline Cogn
levels Behav
are decreased
in Parkinson’s disease. Ann Neurol
ofnalhypocretin
neuronsmeasurement
in human narcolepsy.
Neuron
2000;27:
patients.
Neurol 2008;21:83–86.
and other hypersomnias. Arch Neurol 2002;59:1553–1562.
1990;27:683–685.
469–474.
126. Welch
MJ, Markham CH, Jenden DJ. Acetylcholine and choline
107.Nishino
Ripley S,
B, Ripley
Overeem
S, Fujiki S,N,etetal.al.Low
CSFcerebrospinal
hypocretin/orexin
128.inYamada
H, Otsuka
K, Kawashima
Yoshidaand
M.
105.
B, Overeem
fluid
cerebrospinal
fluidM,
of Fujimoto
patients with
Parkinson’sK,disease
levels in narcolepsy
andaltered
other neurological
conditions.
NeurolDeterminationchorea.
of acetylcholine
concentration
in cerebrospinal
hypocretin
(Orexin) and
energy homeostasis
in human
Huntington’s
J Neurol Neurosurg
Psychiatry
1976;39:
ogy 2001;57:2253–2258.
fluid of patients with neurologic diseases. Acta Neurol Scand
narcolepsy.
Ann Neurol 2001;50:381–388.
367–374.
108.Mignot
Jellinger
The pathology
ofB,
Parkinson’s
Adv Neurol
1996;93:76–78.
106.
E, KA.
Lammers
GJ, Ripley
et al. The disease.
role of cerebrospi127. Manyam
BV, Giacobini E, Colliver JA. Cerebrospinal fluid
2001;86:55–72.
129.choline
Kikuchilevels
A, Takeda
A, Onodera
H, et al. disease.
SystemicAnn
increase
nal
fluid hypocretin measurement in the diagnosis of narcolepsy
are decreased
in Parkinson’s
Neurolof
109.and
Langston
JW, Forno LS.
TheNeurol
hypothalamus
in Parkinson disoxidative nucleic acid damage in Parkinson’s disease and multiother hypersomnias.
Arch
2002;59:1553–1562.
1990;27:683–685.
ease. Ann
Neurol 1978;3:129–133.
ple system
atrophy.M,
Neurobiol
107. Ripley
B, Overeem
S, Fujiki N, et al. CSF hypocretin/orexin
128. Yamada
H, Otsuka
FujimotoDis
K, 2002;9:244–248.
Kawashima K, Yoshida M.
110.levels
YasuiinK,narcolepsy
Inoue Y, Kanbayashi
T, Nomura T,
Kusumi M,
Naka130.Determination
Abe T, Isobe ofC,acetylcholine
Murata T, Sato
C, Tohgi in
H. cerebrospinal
Alteration of
and other neurological
conditions.
Neurolconcentration
shima
K. CSF orexin levels of Parkinson’s disease, dementia
8-hydroxyguanosine
in theActa
cerebrospinal
fluid
ogy
2001;57:2253–2258.
fluid
of patients with concentrations
neurologic diseases.
Neurol Scand
with Lewy
progressive
supranuclear
palsy Adv
and Neurol
corticoand serum from patients with Parkinson’s disease. Neurosci Lett
108. Jellinger
KA.bodies,
The pathology
of Parkinson’s
disease.
1996;93:76–78.
basal degeneration. J Neurol Sci 2006;250:120–123.
2003;336:105–108.
2001;86:55–72.
129. Kikuchi
A, Takeda A, Onodera H, et al. Systemic increase of
111.Langston
Abdo WF,
Bloem
HP, Lammers inGJ,Parkinson
Verbeek MM,
131.oxidative
Zubenkonucleic
GS, Volicer
L, Direnfeld
LK, Freeman
109.
JW,
FornoBR,
LS.Kremer
The hypothalamus
disacid damage
in Parkinson’s
diseaseM,
andLanglais
multiOvereem
S. CSF 1978;3:129–133.
hypocretin-1 levels are normal in multiple-sysPJ,system
Nixonatrophy.
RA. Cerebrospinal
fluid
levels of angiotensin-conease.
Ann Neurol
ple
Neurobiol Dis
2002;9:244–248.
tem atrophy.
Relat
verting
enzyme
Alzheimer’s
disease
110. Yasui
K, InoueParkinsonism
Y, Kanbayashi
T, Disord
Nomura2008;14:342–344.
T, Kusumi M, Naka130. Abe
T, Isobe
C, in
Murata
T, Sato disease,
C, TohgiParkinson’s
H. Alteration
of
and progressive supranuclear
palsy.inBrain
Res 1985;328:215–
112.shima
Sternberger
NH,
Sternberger
LA,
Ulrich J. Aberrant
neurofilaK. CSF
orexin
levels of
Parkinson’s
disease, dementia
8-hydroxyguanosine
concentrations
the cerebrospinal
fluid
221.
mentLewy
phosphorylation
in Alzheimer
disease. palsy
Proc Natl
Sci
with
bodies, progressive
supranuclear
and Acad
corticoand
serum from patients with Parkinson’s disease. Neurosci Lett
USAdegeneration.
1985;82:4274–4276.
132.2003;336:105–108.
Zubenko GS, Marquis JK, Volicer L, Direnfeld LK, Langlais
basal
J Neurol Sci 2006;250:120–123.
113.Abdo
Yazawa
GiassonBR,
BI,Kremer
Sasaki R,
al. MouseGJ,
model
of multiple
PJ, NixonGS,
RA.Volicer
Cerebrospinal
fluid levels
of angiotensin-convert111.
WF,I, Bloem
HP,etLammers
Verbeek
MM,
131. Zubenko
L, Direnfeld
LK, Freeman
M, Langlais
ingNixon
enzyme,
dopamine
metabolites in
system atrophy
alpha-synuclein
expression
in oligodendrocytes
Overeem
S. CSF hypocretin-1
levels
are normal
in multiple-sysPJ,
RA.acetylcholinesterase,
Cerebrospinal fluidand
levels
of angiotensin-condementia
associated
with Alzheimer’s
disease
and Parkinson’s
causes
glial Parkinsonism
and neuronalRelat
degeneration.
Neuron 2005;45:847–
tem
atrophy.
Disord 2008;14:342–344.
verting
enzyme
in Alzheimer’s
disease,
Parkinson’s
disease
disease:
a correlative
study.palsy.
Biol Brain
Psychiatry
1986;21:1365–
859.
and
progressive
supranuclear
Res 1985;328:215–
112. Sternberger
NH, Sternberger LA, Ulrich J. Aberrant neurofila1381.
114.ment
Liu phosphorylation
Q, Xie F, Siedlak
SL, et al.disease.
Neurofilament
221.
in Alzheimer
Proc Natlproteins
Acad Sciin
neurodegenerative
diseases. Cell Mol Life Sci 2004;61:3057–
133.Zubenko
Nielsen HM,
Londos E,
SM.
Soluble
USA
1985;82:4274–4276.
132.
GS, Marquis
JK,Minthon
VolicerL,L,Janciauskiene
Direnfeld LK,
Langlais
adhesion
molecules
and angiotensin-converting
enzyme in
3075. I, Giasson BI, Sasaki R, et al. Mouse model of multiple
113. Yazawa
PJ,
Nixon RA.
Cerebrospinal
fluid levels of angiotensin-convertdementia.
Dis 2007;26:27–35.
115.system
Holmberg
B, Johnels
B, Ingvarsson
P, Eriksson
B, Rosengren
ing
enzyme,Neurobiol
acetylcholinesterase,
and dopamine metabolites in
atrophy
alpha-synuclein
expression
in oligodendrocytes
L. CSF-neurofilament
anddegeneration.
levodopa tests
combined
with dis134.dementia
Ruberg M,
Rieger F,
Villageois
A, Bonnet
Y. Aceassociated
with
Alzheimer’s
diseaseAM,
andAgid
Parkinson’s
causes
glial and neuronal
Neuron
2005;45:847–
criminant analysis may contribute to the differential diagnosis
tylcholinesterase
and butyrylcholinesterase
in frontal
cortex and
disease:
a correlative
study. Biol Psychiatry
1986;21:1365–
859.
1990;27:683–685
128. Yamada H, Otsu
Determination o
fluid of patients
1996;93:76–78.
129. Kikuchi A, Tak
oxidative nucleic
ple system atrop
130. Abe T, Isobe C
8-hydroxyguano
and serum from
2003;336:105–10
131. Zubenko GS, V
PJ, Nixon RA.
verting enzyme
and progressive
221.
132. Zubenko GS, M
PJ, Nixon RA. C
ing enzyme, ace
dementia associ
disease: a corr
1381.
133. Nielsen HM, Lo
adhesion molec
dementia. Neuro
134. Ruberg M, Rieg
tylcholinesterase
cerebrospinal flu
Parkinson’s dise
135. Jolkkonen J, So
immunoreactivit
kinson’s disease
surg Psychiatry
us in Parkinson dis-
T, Kusumi M, Naka’s disease, dementia
ar palsy and cortico120–123.
rs GJ, Verbeek MM,
rmal in multiple-sys08;14:342–344.
. Aberrant neurofila. Proc Natl Acad Sci
use model of multiple
in oligodendrocytes
Neuron 2005;45:847–
ofilament proteins in
e Sci 2004;61:3057–
iksson B, Rosengren
combined with disdifferential diagnosis
Relat Disord 2001;8:
Johnels B. Increased
protein in progressive
ophy compared with
0–77.
148. de Jong PJ, Lakke JP, Teelken AW. CSF GABA levels in
oxidative nucleic acid damage in Parkinson’s disease and multiParkinson’s disease. Adv Neurol 1984;40:427–430.
ple system atrophy. Neurobiol Dis 2002;9:244–248.
149. Manyam BV, Tremblay RD. Free and conjugated GABA in
130. Abe T, Isobe C, Murata T, Sato C, Tohgi H. Alteration of
human cerebrospinal fluid: effect of degenerative neurologic
8-hydroxyguanosine concentrations in the cerebrospinal fluid
diseases and isoniazid. Brain Res 1984;307:217–223.
and serum from patients with Parkinson’s disease. Neurosci Lett
2003;336:105–108.
150. Araki K, Takino T, Ida S, Kuriyama K. Alteration of amino
acids in cerebrospinal fluid from patients with Parkinson’s dis131. Zubenko GS, Volicer L, Direnfeld LK, Freeman M, Langlais
ease and spinocerebellar degeneration. Acta Neurol Scand 1986;
PJ, Nixon RA. Cerebrospinal fluid levels of angiotensin-conB. Mollenhauer and C. Trenkwalder
73:105–110.
verting enzyme in Alzheimer’s disease, Parkinson’s disease
and progressive supranuclear palsy. Brain Res 1985;328:215–
151. Bonnet AM, Tell G, Schechter PJ, et al. Cerebrospinal fluid
221.
GABA and homocarnosine concentrations in patients with
Friedreich’s ataxia, Parkinson’s disease, and Huntington’s cho132. Zubenko GS, Marquis JK, Volicer L, Direnfeld LK, Langlais
rea. Mov Disord 1987;2:117–123.
PJ, Nixon RA. Cerebrospinal fluid levels of angiotensin-converting enzyme, acetylcholinesterase, and dopamine metabolites in
152. Jimenez-Jimenez FJ, Molina JA, Vargas C, et al. Neurotransdementia associated with Alzheimer’s disease and Parkinson’s
mitter amino acids in cerebrospinal fluid of patients with Pardisease: a correlative study. Biol Psychiatry 1986;21:1365–
kinson’s disease. J Neurol Sci 1996;141:39–44.
1381.
153. Mally J, Szalai G, Stone TW. Changes in the concentration of
133. Nielsen HM, Londos E, Minthon L, Janciauskiene SM. Soluble
amino acids in serum and cerebrospinal fluid of patients with
adhesion molecules and angiotensin-converting enzyme in
Parkinson’s disease. J Neurol Sci 1997;151:159–162.
1422
C. TRENKWALDER
dementia. Neurobiol Dis 2007;26:27–35.B. MOLLENHAUER AND 154.
Molina JA, Jimenez-Jimenez FJ, Gomez P, et al. Decreased cere134. Ruberg M, Rieger F, Villageois A, Bonnet AM, Agid Y. Acebrospinal fluid levels of neutral and basic amino acids in patients
tylcholinesterase and butyrylcholinesterase in frontal cortex and
with Parkinson’s disease. J Neurol Sci 1997;150:123–127.
136.cerebrospinal
Sirvio J, Soininen
Kutvonen
Hyttinen JM,patients
Helkala
EL,
155. Tohgi H, Abe T, Takahashi S, Nozaki Y, Kikuchi T. Concenfluid ofHS,
demented
and R,
non-demented
with
Riekkinen disease.
PJ. Acetyltrations of tyrosine, L-dihydroxyphenylalanine, dopamine, and
Parkinson’s
Brainand
Resbutyrylcholinesterase
1986;362:83–91. activity in the
cerebrospinal
fluid of H,
patients
with T,
Parkinson’s
disease. J Neu3-O-methyldopa in the cerebrospinal fluid of Parkinson’s dis135. Jolkkonen
J, Soininen
Halonen
et al. Somatostatin-like
1422immunoreactivity
rol Sci 1987;81:273–279.
ease. Neurosci Lett 1991;127:212–214.
in the cerebrospinal B.
fluidMOLLENHAUER
of patients with Par- AND C. TRENKWALDER
Movement
Disorders,
Vol. 24, No.
2009 JJ, Bergmans PL, Scheltens P,
137.kinson’s
Yoshinaga
J, Sasaki
T, Ideshita
Hikiji A, Kuwaki
Acetyl156. Kuiper
MA, Teerlink
T, 10,
Visser
disease
and its
relation H,
to dementia.
J NeurolT.Neurocholinesterase
activity in CSF in senile dementia of Alzheimer
Wolters EC. L-glutamate, L-arginine and L-citrulline levels in
surg
Psychiatry 1986;49:1374–1377.
type, J,
vascular
dementia,
and Parkinson’s
disease.
Rinsho Shincerebrospinal
fluid
of Parkinson’s
disease,
multiple T.
system
atro136. Sirvio
Soininen
HS, Kutvonen
R, Hyttinen
JM, Helkala
EL,
155. Tohgi
H, Abe T,
Takahashi
S, Nozaki
Y, Kikuchi
Concenkeigaku 1989;29:376–378.
phy, and
disease patients. J Neural
Transm 2000;
Riekkinen
PJ. Acetyl- and butyrylcholinesterase activity in the
trations
of Alzheimer’s
tyrosine, L-dihydroxyphenylalanine,
dopamine,
and
107:183–189. in the cerebrospinal fluid of Parkinson’s dis138.cerebrospinal
Konings CH,fluid
Kuiper
MA, Mulder
C, Calliauwdisease.
J, Wolters
EC.
of patients
with Parkinson’s
J Neu3-O-methyldopa
CSF
acetylcholinesterase in Parkinson disease: decreased
157.ease.
Widner
B, Leblhuber
F, Fuchs D. Increased neopterin producrol
Sci 1987;81:273–279.
Neurosci
Lett 1991;127:212–214.
Movement
Disorders,
Vol.
24,
No.
10,
2009
enzyme activity
immunoreactivity
in Kuwaki
demented
patients.
tion and
degradation
advancedPL,
Parkinson’s
137. Yoshinaga
J, Sasakiand
T, Ideshita
H, Hikiji A,
T. Acetyl156. Kuiper
MA,tryptophan
Teerlink T,
Visser JJ, inBergmans
Scheltens disP,
Clin Chim Acta
1995;235:101–105.
ease. J Neural
Transm 2002;109:181–189.
cholinesterase
activity
in CSF in senile dementia of Alzheimer
Wolters
EC. L-glutamate,
L-arginine and L-citrulline levels in
139.type,
Hartikainen
Reinikainen
KJ, Soininendisease.
H, Sirvio
J, Soikkeli
158.cerebrospinal
Konings CH,fluid
Kuiper
MA, Teerlink
T, Mulder
Scheltens
vascular P,dementia,
and Parkinson’s
Rinsho
Shinof Parkinson’s
disease,
multipleC,system
atro-P,
R, Riekkinen
PJ. Neurochemical markers in the cerebrospinal
Wolters
EC. Normal disease
cerebrospinal
fluid
glutathione
concentrakeigaku
1989;29:376–378.
phy,
and Alzheimer’s
patients.
J Neural
Transm
2000;
fluid of CH,
patients
withMA,
Alzheimer’s
Parkinson’s
tions in Parkinson’s disease, Alzheimer’s disease and multiple
107:183–189.
138. Konings
Kuiper
Mulder C,disease,
Calliauw
J, Woltersdisease
EC.
and amyotrophic
lateral sclerosis
and normal
controls.
J Neural
system B,
atrophy.
J Neurol
Sci 1999;168:112–115.
CSF
acetylcholinesterase
in Parkinson
disease:
decreased
157. Widner
Leblhuber
F, Fuchs
D. Increased neopterin producTransm activity
Park Disand
Dement
Sect 1992;4:53–68.
159.tion
Molina
Leza JC, degradation
Ortiz S, et al.inCerebrospinal
fluid and plasma
enzyme
immunoreactivity
in demented patients.
and JA,
tryptophan
advanced Parkinson’s
dis140.Clin
Polinsky
RT, Burns RS, Harvey-White J, Kopin IJ.
concentrations
of nitric2002;109:181–189.
oxide metabolites are increased in demenChim RJ,
ActaBrown
1995;235:101–105.
ease.
J Neural Transm
Low lumbarP,CSF
levels ofKJ,
homovanillic
acidSirvio
and 5-hydroxyintia with CH,
LewyKuiper
bodies.MA,
Neurosci
Lett 2002;333:151–153.
139. Hartikainen
Reinikainen
Soininen H,
J, Soikkeli
158. Konings
Teerlink
T, Mulder C, Scheltens P,
acid
multiple systemmarkers
atrophyinwith
fail160.Wolters
Molina EC.
JA, Normal
Gomez P,
Vargas C, etfluid
al. glutathione
Neurotransmitter
amino
R,doleacetic
Riekkinen
PJ.inNeurochemical
the autonomic
cerebrospinal
cerebrospinal
concentraure. of
J Neurol
Psychiatrydisease,
1988;51:914–919.
acid in
in Parkinson’s
cerebrospinaldisease,
fluid ofAlzheimer’s
patients withdisease
dementia
Lewy
fluid
patientsNeurosurg
with Alzheimer’s
Parkinson’s disease
tions
andwith
multiple
141.and
Konagaya
M, Konagaya
Y, Iidaand
M.normal
[CSF acetylcholinesterase
bodies.atrophy.
J NeuralJ Neurol
TransmSci
2005;112:557–563.
amyotrophic
lateral sclerosis
controls. J Neural
system
1999;168:112–115.
activityPark
in central
neurological
diseases involving cholinergic
161.Molina
Tosca JA,
P, Canevari
L, DiS,Paolo
et al. Glutamate
andplasma
GABA
Transm
Dis Dement
Sect 1992;4:53–68.
159.
Leza JC, Ortiz
et al. E,
Cerebrospinal
fluid and
systems].RJ,
Rinsho
Shinkeigaku
levels in CSFof from
affected are
by increased
dementia in
and
olivo140. Polinsky
Brown
RT, Burns 1992;32:266–271.
RS, Harvey-White J, Kopin IJ.
concentrations
nitric patients
oxide metabolites
demen142.Low
Ruberg
M, Villageois
AM, Pillon
B, Rieger
F, Agid
atrophy.
ActaLett
Neurol
Scand 1992;85:430–435.
lumbar
CSF levelsA,
of Bonnet
homovanillic
acid and
5-hydroxyintiaponto-cerebellar
with Lewy bodies.
Neurosci
2002;333:151–153.
Y. Acetylcholinesterase
butyrylcholinesterase
activity in
the
162.Molina
VermesJA,
I, Steur
C, Haanen C. Decreased
doleacetic
acid in multipleand
system
atrophy with autonomic
fail160.
GomezEN,
P, Reutelingsperger
Vargas C, et al. Neurotransmitter
amino
cerebrospinal
fluid of patients
with
neurodegenerative diseases
concentration
of annexin
V patients
in parkinsonian
cerebrospinal
fluid:
ure.
J Neurol Neurosurg
Psychiatry
1988;51:914–919.
acid
in cerebrospinal
fluid of
with dementia
with Lewy
involving M,
cholinergic
Neurol
Psychiatry
speculation
on Transm
the underlying
cause. Mov Disord 1999;14:
141. Konagaya
Konagayasystems.
Y, Iida JM.
[CSF Neurosurg
acetylcholinesterase
bodies.
J Neural
2005;112:557–563.
1987;50:538–543.
1008–1010.
activity
in central neurological diseases involving cholinergic
161. Tosca
P, Canevari L, Di Paolo E, et al. Glutamate and GABA
143.systems].
Atack JR,
Litvan
I, Thal LJ,1992;32:266–271.
May C, Rapoport SI, Chase TN.
163.levels
Mogi inM,CSF
Harada
Kondo affected
T, et al. by
bcl-2
protein and
is increased
Rinsho
Shinkeigaku
fromM,patients
dementia
olivoCerebrospinal
fluid acetylcholinesterase
in progressive
supranuin the brain from
parkinsonian
patients.
Lett 1996;
142. Ruberg
M, Villageois
A, Bonnet AM, Pillon
B, Rieger F,
Agid
ponto-cerebellar
atrophy.
Acta Neurol
Scand Neurosci
1992;85:430–435.
palsy: reduced activity
relative to normalactivity
subjects
and
215:137–139.
Y.clear
Acetylcholinesterase
and butyrylcholinesterase
in the
162. Vermes
I, Steur EN, Reutelingsperger C, Haanen C. Decreased
lack of inhibition
bypatients
oral physostigmine.
J Neurol Neurosurg
164.concentration
Goldstein DS,ofHolmes
O, et al. Biomarkers
detect
cerebrospinal
fluid of
with neurodegenerative
diseases
annexinC,V Bentho
in parkinsonian
cerebrospinalto fluid:
Psychiatrycholinergic
1991;54:832–835.
central dopamine
distinguish
Parkinson
disease
involving
systems. J Neurol Neurosurg Psychiatry
speculation
on the deficiency
underlyingandcause.
Mov Disord
1999;14:
144.1987;50:538–543.
Abbott RJ, Pye IF, Nahorski SR. CSF and plasma GABA levels
from multiple system atrophy. Parkinsonism Relat Disord 2008;
1008–1010.
in Parkinson’s
Neurol
Psychiatry
1982;45:
14:600–607.
143. Atack
JR, Litvandisease.
I, ThalJ LJ,
MayNeurosurg
C, Rapoport
SI, Chase
TN.
163. Mogi
M, Harada M, Kondo T, et al. bcl-2 protein is increased
253–256.
165.inMartignoni
Blandini
F, Petraglia
F, Pacchetti
Cerebrospinal
fluid acetylcholinesterase in progressive supranuthe brain E,
from
parkinsonian
patients.
Neurosci C,
LettBono
1996;G,
145.clear
Kuroda
H, Ogawa
Yamawaki
Y, to
et al.
Cerebrospinal
fluid
Nappi G. Cerebrospinal fluid norepinephrine, 3-methoxy-4palsy:
reduced N,activity
relative
normal
subjects and
215:137–139.
GABA
levels in various
andJ psychiatric
diseases.
hydroxyphenylglycol
neuropeptide
levels in Parkinson’s
lack
of inhibition
by oral neurological
physostigmine.
Neurol Neurosurg
164. Goldstein
DS, Holmes and
C, Bentho
O, et al.YBiomarkers
to detect
J Neurol Neurosurg
Psychiatry 1982;45:257–260.
disease,dopamine
multiple deficiency
system atrophy
and dementia
of the Alzheimer
Psychiatry
1991;54:832–835.
central
and distinguish
Parkinson
disease
146.Abbott
Manyam
Low
CSF gamma-aminobutyric
acid levels
type.multiple
J Neuralsystem
Transm
Park Dis
Dement Sect
1992;4:191–205.
144.
RJ, BV.
Pye IF,
Nahorski
SR. CSF and plasma GABA
levelsin
from
atrophy.
Parkinsonism
Relat
Disord 2008;
of Neurosurg
levodopa Psychiatry
and carbidopa.
Arch
166.14:600–607.
Papeschi R, Molina-Negro P, Sourkes TL, Erba G. The conceninParkinson’s
Parkinson’sDisease.
disease. Effect
J Neurol
1982;45:
Neurol 1982;39:391–392.
tration of homovanillic
andPetraglia
5-hydroxyindoleacetic
acids
in ven253–256.
165. Martignoni
E, Blandini F,
F, Pacchetti C,
Bono
G,
147.Kuroda
FerraroH,
TN,
Manyam
BV, Hare TA.
Further
characterization
tricularG.andCerebrospinal
lumbar CSF. Studies
in patients with 3-methoxy-4extrapyramidal
145.
Ogawa
N, Yamawaki
Y, et
al. Cerebrospinal
fluidof
Nappi
fluid norepinephrine,
in vitro
conditions
appropriate
for and
GABA
determination
disorders, epilepsy, and
andneuropeptide
other diseases.
Neurology
1972;22:
GABA
levels
in various
neurological
psychiatric
diseases.in
hydroxyphenylglycol
Y levels
in Parkinson’s
impact
of acid 1982;45:257–260.
deproteinization and freeze/thaw.
1151–1159.
J human
Neurol CSF:
Neurosurg
Psychiatry
disease,
multiple system atrophy and dementia of the Alzheimer
J Neurochem
167.type.
Casati
C, Agnoli
A,Park
JoriDis
A, Dement
Dolfini Sect
E. On
the relationship
146. Manyam
BV. 1983;41:1057–1064.
Low CSF gamma-aminobutyric acid levels in
J Neural
Transm
1992;4:191–205.
148.Parkinson’s
de Jong PJ,
Lakke Effect
JP, Teelken
AW. CSF
GABA levels
betweenR,L-DOPA
therapyP,and
CSF TL,
monoamine
Disease.
of levodopa
and carbidopa.
Archin
166. Papeschi
Molina-Negro
Sourkes
Erba G. metabolites
The concen-in
Parkinson’s
disease. Adv Neurol 1984;40:427–430.
Parkinson’s
disease. Z and
Neurol
1973;204:149–154. acids in venNeurol
1982;39:391–392.
tration
of homovanillic
5-hydroxyindoleacetic
149.Ferraro
Manyam
Tremblay
RD. TA.
Free Further
and conjugated
GABAofin
168.tricular
Watsonand
E, lumbar
Wilk S.CSF.
Assessment
cerebrospinal
fluid levels of
147.
TN,BV,
Manyam
BV, Hare
characterization
Studies inofpatients
with extrapyramidal
fluid: effect
degenerative
neurologic
dopamine epilepsy,
metabolites
gas chromatography.
Psychopharmainhuman
vitro cerebrospinal
conditions appropriate
for ofGABA
determination
in
disorders,
andbyother
diseases. Neurology
1972;22:
diseases
and impact
isoniazid.
Res 1984;307:217–223.
cologia 1975;42:57–56.
human
CSF:
of Brain
acid deproteinization
and freeze/thaw.
1151–1159.
150.J Araki
K, Takino
T, Ida S, Kuriyama K. Alteration of amino
169.Casati
Chase C,
TN,Agnoli
Eng N,A,Gordon
EK.Dolfini
Biochemical
the diagnoNeurochem
1983;41:1057–1064.
167.
Jori A,
E. Onaids
the inrelationship
cerebrospinal
from AW.
patients
with
Parkinson’s
sis of Parkinson’s
disease.and
AnnCSF
Clinmonoamine
Lab Sci 1976;6:4–10.
148. deacids
Jongin PJ,
Lakke JP,fluid
Teelken
CSF
GABA
levels disin
between
L-DOPA therapy
metabolites in
ease and spinocerebellar
degeneration.
Acta Neurol Scand 1986;
170.Parkinson’s
Extein I, Van
Woert
M, Roth1973;204:149–154.
RH, Bowers MB, Jr. 14C-homoParkinson’s
disease. Adv Neurol
1984;40:427–430.
disease.
Z Neurol
73:105–110.
vanillicE,acid
in S.
theAssessment
cerebrospinal
fluid of parkinsonian
patients
149. Manyam
BV, Tremblay RD. Free and conjugated GABA in
168. Watson
Wilk
of cerebrospinal
fluid levels
of
151.human
Bonnetcerebrospinal
AM, Tell G,fluid:
Schechter
al. Cerebrospinal
fluid
after intravenous
14C-L-dopa.
Psychiatry 1976;11:227–232.
effect PJ,
of et
degenerative
neurologic
dopamine
metabolites
by gas Biol
chromatography.
PsychopharmaGABA and
andisoniazid.
homocarnosine
in patients with
171.cologia
Davidson
DL, Yates CM, Mawdsley C, Pullar IA, Wilson H.
diseases
Brain Resconcentrations
1984;307:217–223.
1975;42:57–56.
Friedreich’s
ataxia,
disease,
Huntington’s
choCSF TN,
studies
relationship
between dopamine
5-hy150. Araki
K, Takino
T, Parkinson’s
Ida S, Kuriyama
K. and
Alteration
of amino
169. Chase
EngonN,the
Gordon
EK. Biochemical
aids in theand
diagnorea. Mov
Disord 1987;2:117–123.
Parkinsonism
other
disorders.
acids
in cerebrospinal
fluid from patients with Parkinson’s dissisdroxytryptamine
of Parkinson’s in
disease.
Ann Clinand
Lab
Sci movement
1976;6:4–10.
152.ease
Jimenez-Jimenez
FJ, Molina
JA, Vargas
et al.Scand
NeurotransJ Neurol
Neurosurg
1977;40:1136–1141.
and spinocerebellar
degeneration.
Acta C,
Neurol
1986;
170. Extein
I, Van
Woert Psychiatry
M, Roth RH,
Bowers MB, Jr. 14C-homomitter amino acids in cerebrospinal fluid of patients with Par172.vanillic
Pezzoliacid
G, in
Panerai
AE, Di Giulio
A, Passerini
73:105–110.
the cerebrospinal
fluidA,ofLongo
parkinsonian
patientsD,
kinson’s
disease.
Sci 1996;141:39–44.
Carenzi
A. Methionine-enkephalin,
substance
P, and homovanil151. Bonnet
AM,
Tell JG,Neurol
Schechter
PJ, et al. Cerebrospinal fluid
after
intravenous
14C-L-dopa. Biol Psychiatry
1976;11:227–232.
153.GABA
Mally J,and
Szalai
G, Stone TW.
Changes in the
lic acid in
CSF CM,
of parkinsonian
patients.
homocarnosine
concentrations
in concentration
patients withof
171. Davidson
DL,theYates
Mawdsley C,
Pullar Neurology
IA, Wilson1984;
H.
amino acidsataxia,
in serum
and cerebrospinal
of patientschowith
34:516–519.
Friedreich’s
Parkinson’s
disease, andfluid
Huntington’s
CSF
studies on the relationship between dopamine and 5-hyParkinson’s
disease.
J Neurol Sci 1997;151:159–162.
173.droxytryptamine
Direnfeld LK, Albert
ML, Volicer
L, Langlais
PJ, disorders.
Marquis J,
rea.
Mov Disord
1987;2:117–123.
in Parkinsonism
and other
movement
154.Jimenez-Jimenez
Molina JA, Jimenez-Jimenez
FJ, Gomez
Decreased
cereE. Parkinson’s
disease.1977;40:1136–1141.
The possible relationship of lat152.
FJ, Molina JA,
Vargas P,C,etetal.al.
NeurotransJ Kaplan
Neurol Neurosurg
Psychiatry
brospinal
fluid
levels
neutral and basic
acidswith
in patients
erality G,
to Panerai
dementiaAE,
andDineurochemical
findings.
Arch Neurol
mitter
amino
acids
in of
cerebrospinal
fluid amino
of patients
Par172. Pezzoli
Giulio A, Longo
A, Passerini
D,
with Parkinson’s
Neurol
Sci 1997;150:123–127.
1984;41:935–941.
kinson’s
disease. Jdisease.
Neurol JSci
1996;141:39–44.
Carenzi
A. Methionine-enkephalin, substance P, and homovanil153. Mally J, Szalai G, Stone TW. Changes in the concentration of
lic acid in the CSF of parkinsonian patients. Neurology 1984;
amino acids in serum and cerebrospinal fluid of patients with
34:516–519.
Parkinson’s disease. J Neurol Sci 1997;151:159–162.
173. Direnfeld LK, Albert ML, Volicer L, Langlais PJ, Marquis J,
154. Molina JA, Jimenez-Jimenez FJ, Gomez P, et al. Decreased cereKaplan E. Parkinson’s disease. The possible relationship of latMovement
Disorders,
Vol. 24,ofNo.
10, 2009
brospinal
fluid levels
neutral
and basic amino acids in patients
erality to dementia and neurochemical findings. Arch Neurol
with Parkinson’s disease. J Neurol Sci 1997;150:123–127.
1984;41:935–941.
168.
169.
170.
171.
172.
173.
13
between L-DOP
Parkinson’s dise
Watson E, Wilk
dopamine metab
cologia 1975;42
Chase TN, Eng
sis of Parkinson
Extein I, Van W
vanillic acid in
after intravenous
Davidson DL, Y
CSF studies on
droxytryptamine
J Neurol Neuros
Pezzoli G, Pan
Carenzi A. Meth
lic acid in the
34:516–519.
Direnfeld LK, A
Kaplan E. Parki
erality to deme
1984;41:935–94
with Parkinson’s disa Neurol Scand 1986;
sis of Parkinson’s disease. Ann Clin Lab Sci 1976;6:4–10.
170. Extein I, Van Woert M, Roth RH, Bowers MB, Jr. 14C-homovanillic acid in the cerebrospinal fluid of parkinsonian patients
. Cerebrospinal fluid
after intravenous 14C-L-dopa. Biol Psychiatry 1976;11:227–232.
ns in patients with
171. Davidson DL, Yates CM, Mawdsley C, Pullar IA, Wilson H.
nd Huntington’s choCSF studies on the relationship between dopamine and 5-hydroxytryptamine in Parkinsonism and other movement disorders.
CSF DIAGNOSTICS IN MOVEMENT DISORDERS
1423
C, et al. NeurotransJ Neurol Neurosurg Psychiatry 1977;40:1136–1141.
運動障害の鑑別診断における神経化学的バイオマーカー
of patients with Par172. Pezzoli G, Panerai AE, Di Giulio A, Longo A, Passerini D,
–44.
Carenzi A. Methionine-enkephalin, substance P, and homovanil174.licVolicer
Direnfeld
Freedman patients.
M, AlbertNeurology
ML, Langlias
192. Kuhn W, Muller T, Gerlach M, et al. Depression in Parkinson’s
the concentration of
acid inL,the
CSF ofLK,
parkinsonian
1984;PJ,
Bird ED. Serotonin and 5-hydroxyindoleacetic acid in CSF. Difdisease: biogenic amines in CSF of ‘‘de novo’’ patients. J Neufluid of patients with
34:516–519.
ference in
Parkinson’s
disease
and L,
dementia
the Marquis
Alzheimer’s
ral Transm 1996;103:1441–1445.
:159–162.
173. Direnfeld
LK,
Albert ML,
Volicer
Langlaisof PJ,
J,
DIAGNOSTICS
IN MOVEMENT
1423
type. Arch
Neurol 1985;42:127–129.
193. Zhou DISORDERS
G, Shoji H, Yamada S, Matsuishi T. Decreased
betaet al. Decreased cereKaplan
E. Parkinson’s
disease. TheCSF
possible
relationship of lat175.erality
Gibson
Logue M,
JH. CSFfindings.
monoamine
phenylethylamine in CSF in Parkinson’s disease. J Neurol Neumino acids in patients
to CJ,
dementia
andGrowdon
neurochemical
Archmetabolite
Neurol
levels in Alzheimer’s and Parkinson’s disease. Arch Neurol
rosurg Psychiatry 1997;63:754–758.
150:123–127.
1984;41:935–941.
1985;42:489–492.
174. Volicer
L, Direnfeld LK, Freedman M, Albert ML, Langlias PJ,
192.
W,MI,
Muller
T, SN.
Gerlach
M, etamine
al. Depression
in Parkinson’s
194.Kuhn
Botez
Young
Biogenic
metabolites
and thiamine
ED. Serotonin
and D,
5-hydroxyindoleacetic
acid in CSF. Difdisease:
biogenic amines
of ‘‘de novo’’ patients.
in cerebrospinal
fluid in CSF
heredo-degenerative
ataxias.J NeuCan J
176.Bird
Kurlan
R, Goldblatt
Zaczek R, et al. Cerebrospinal
fluid
ference
in Parkinson’s
disease
and dementia
of the Alzheimer’s
ralNeurol
Transm
homovanillic
acid and
parkinsonism
in Huntington’s
disease.
Sci1996;103:1441–1445.
2001;28:134–140.
type.
Neurol
1985;42:127–129.
AnnArch
Neurol
1988;24:282–284.
193.
Shoji
S, Matsuishi
T. Decreased
195.Zhou
AbdoG,WF,
vanH,deYamada
Warrenburg
BP, Munneke
M, et al.betaCSF
175.
JH. CSF
monoamine
metaboliteS,
phenylethylamine
in CSFmultiple-system
in Parkinson’s disease.
Neurol
Neuanalysis differentiates
atrophy Jfrom
idiopathic
177.Gibson
Nishi CJ,
K, Logue
Kondo M,
T, Growdon
Narabayashi
H, Takubo
H, Muramoto
levels
Alzheimer’s
and Parkinson’s
disease.inArch
Neurol
rosurg
Psychiatry
1997;63:754–758.
late-onset
cerebellar
ataxia. Neurology 2006;67:474–479.
Arakiin H.
Unresponsiveness
to L-DOPA
parkinsonian
1985;42:489–492.
patients: a study of homovanillic acid concentration in the cere194.
MI, Young
SN. I,
Biogenic
amine
metabolites
thiamineK.
196.Botez
Yamada
T, Moroo
Koguchi
Y, Asahina
M, and
Hirayama
brospinal
J Neurol
Sci 1989;92:65–70.
inIncreased
cerebrospinal
fluid in ofheredo-degenerative
ataxias.
CancereJ
176. Kurlan
R, fluid.
Goldblatt
D, Zaczek
R, et al. Cerebrospinal fluid
concentration
C4d complement protein
in the
and parkinsonism
Huntington’s
disease.M.
Neurol
Sci 2001;28:134–140.
brospinal
fluids in progressive supranuclear palsy. Acta Neurol
178.homovanillic
Fukuda H, acid
Nakamura
S, Hara K, in
Udaka
F, Kameyama
Ann
Neurol
ScandWF,
1994;89:42–46.
[Study
on 1988;24:282–284.
the concentration of 5-hydroxyindoleacetic acid (5195. Abdo
van de Warrenburg BP, Munneke M, et al. CSF
HIAA)
the lumbar
cerebrospinal
fluid (CSF)
in neurological
idiopathic
177. Nishi
K, in
Kondo
T, Narabayashi
H, Takubo
H, Muramoto
S,
197.analysis
Volicerdifferentiates
L, Beal MF,multiple-system
Direnfeld LK, atrophy
Marquisfrom
JK, Albert
ML.
diseases].
Shinkeigaku to
1989;29:1192–1194.
late-onset
cerebellar
ataxia.
Neurology
2006;67:474–479.
Araki
H. Rinsho
Unresponsiveness
L-DOPA in parkinsonian
CSF cyclic
nucleotides
and
somatostatin
in Parkinson’s disease.
a study
of FC,
homovanillic
concentration
in themetabocereNeurology
179.patients:
Chia LG,
Cheng
Kuo JS. acid
Monoamines
and their
196. Yamada
T, 1986;36:89–92.
Moroo I, Koguchi Y, Asahina M, Hirayama K.
brospinal
fluid. J and
Neurol
Sci 1989;92:65–70.
lites in plasma
lumbar
cerebrospinal fluid of Chinese patients
concentration
C4d complement
in the cere198.Increased
Covickovic-Sternic
N, ofKostic
VS, Djuricicprotein
BM, Bumbasirevicwith Parkinson’s
disease.
NeurolK,SciUdaka
1993;116:125–134.
brospinal
fluids
in progressive
Acta Neurol
178. Fukuda
H, Nakamura
S, J Hara
F, Kameyama M.
Beslac L,
Nikolic
M, Mrsuljasupranuclear
BB. Cyclic palsy.
nucleotides
in cereScand
1994;89:42–46.
on the concentration
of 5-hydroxyindoleacetic
acid study
(5180.[Study
Cerebrospinal
fluid homovanillic
acid in the DATATOP
brospinal
fluid of drug-free Parkinson patients. Eur Neurol
HIAA)
in the lumbar
cerebrospinal
(CSF)
in neurological
1987;27:24–28.
on Parkinson’s
disease.
Parkinsonfluid
Study
Group.
Arch Neurol
197. Volicer
L, Beal MF, Direnfeld LK, Marquis JK, Albert ML.
diseases].
Rinsho Shinkeigaku 1989;29:1192–1194.
1995;52:237–245.
cyclic
nucleotides
in Parkinson’s
disease.
199.CSF
Ikeda
M, Sato
I, Yuasaand
T, somatostatin
Miyatake T, Murota
S. Nitrite,
nitrate
Neurology
1986;36:89–92.
179.
LG,E,Cheng
FC, Kuo
JS. Monoamines
and their
metaboand cGMP
in the cerebrospinal fluid in degenerative neurologic
181.Chia
Eldrup
Mogensen
P, Jacobsen
J, Pakkenberg
H, Christensen
lites
plasma
lumbarconcentrations
cerebrospinal fluid
of Chinese
patients
diseases. J Neural N,
Transm
1995;100:263–267.
198. Covickovic-Sternic
KosticGen
VS,Sect
Djuricic
BM, BumbasirevicNJ.inCSF
andandplasma
of free
norepinephrine,
with
Parkinson’s
disease. J Neurol Sci 1993;116:125–134.
L, JA,
Nikolic
M, Mrsulja BB.
Cyclic nucleotides
in ceredopamine,
3,4-dihydroxyphenylacetic
acid (DOPAC), 3,4-dihy200.Beslac
Navarro
Jimenez-Jimenez
FJ, Molina
JA, et al. Cerebrospi180. Cerebrospinal
fluid homovanillic
acidepinephrine
in the DATATOP
study
droxyphenylalanine
(DOPA), and
in Parkinson’s
brospinal
drug-free3’5’
Parkinson
patients.levels
Eur inNeurol
nal fluid fluid
cyclicofguanosine
monophosphate
ParkinActa Neurol
1995;92:116–121.
1987;27:24–28.
ondisease.
Parkinson’s
disease.Scand
Parkinson
Study Group. Arch Neurol
son’s disease. J Neurol Sci 1998;155:92–94.
199.
M, Sato
I, Yuasa
Miyatake
Murota of
S. neurotransmitter
Nitrite, nitrate
182.1995;52:237–245.
Chia LG, Cheng LJ, Chuo LJ, Cheng FC, Cu JS. Studies of
201.Ikeda
Cramer
H, Warter
JM,T,Renaud
B. T,
Analysis
and
cGMP in and
the cerebrospinal
fluid in degenerative
181. Eldrup
E, Mogensen
P, electrophysiology
Jacobsen J, Pakkenberg
H, Christensen
dementia,
depression,
and cerebrospinal
fluid
metabolites
adenosine 3’,5’-monophosphate
in neurologic
the CSF of
diseases.
Neural
Transm Gen motor
Sect 1995;100:263–267.
monoamine
in patients with
Parkinson’s
disease.
NJ.
CSF and metabolites
plasma concentrations
of free
norepinephrine,
patientsJwith
extrapyramidal
disorders. Adv Neurol 1984;
J Neurol Sci
1995;133:73–78.
dopamine,
3,4-dihydroxyphenylacetic
acid (DOPAC), 3,4-dihy40:431–435.
200. Navarro
JA, Jimenez-Jimenez FJ, Molina JA, et al. Cerebrospi(DOPA),
and epinephrine
in Parkinson’s
fluid cyclic guanosine
3’5’JC,
monophosphate
in Parkin202.nalJimenez-Jimenez
FJ, Rubio
Molina JA, etlevels
al. Cerebrospinal
183.droxyphenylalanine
LeWitt PA, Galloway
MP, Matson
W, et al. Markers
of dopadisease.
Acta NeurolinScand
1995;92:116–121.
son’s
J Neurol
mine metabolism
Parkinson’s
disease. The Parkinson Study
fluiddisease.
carnitine
levelsSciin1998;155:92–94.
patients with Parkinson’s disease.
Group.
182. Chia
LG,Neurology
Cheng LJ,1992;42:2111–2117.
Chuo LJ, Cheng FC, Cu JS. Studies of
J Neurol
1997;145:183–185.
201. Cramer
H, Sci
Warter
JM, Renaud B. Analysis of neurotransmitter
depression,A,
electrophysiology
and cerebrospinal
184.dementia,
Gonzalez-Quevedo
Garcia JC, Fernandez
R, Fernandezfluid
CarandDeMaggio
adenosine AJ,
3’,5’-monophosphate
in the CSF of is
203.metabolites
Loeffler DA,
Juneau PL, et al. Ceruloplasmin
monoamine
metabolites
in patients
with Parkinson’s
disease.
patients
withinextrapyramidal
motorindisorders.
Adv disease
Neurol 1984;
increased
cerebrospinal fluid
Alzheimer’s
but not
taya L. Monoamine
metabolites
in normal
human cerebrospinal
J Neurol
Sciin1995;133:73–78.
40:431–435.
fluid and
degenerative diseases of the central nervous system.
Parkinson’s disease. Alzheimer Dis Assoc Disord 1994;8:190–
Bol Estud
Biol 1993;41:13–19.
202. Jimenez-Jimenez
FJ, Rubio JC, Molina JA, et al. Cerebrospinal
183. LeWitt
PA, Med
Galloway
MP, Matson W, et al. Markers of dopa197.
metabolism
in Parkinson’s
disease.
Parkinson
Study
185.mine
Strittmatter
M, Hamann
GF, Strubel
D, The
Cramer
H, Schimrigk
levels
in patients
with
Parkinson’s
disease.
204.fluid
Edercarnitine
U, Leitner
B, Kirchmair
R, et
al. Levels
and proteolytic
Group.
Neurology 1992;42:2111–2117.
J Neurol
Sci 1997;145:183–185.
processing
of chromogranin A and B and secretogranin II in
K. Somatostatin-like
immunoreactivity, its molecular forms and
184. Gonzalez-Quevedo
A, Garcia in
JC,aged
Fernandez
R, Fernandez
cerebrospinal
fluid in AJ,
neurological
diseases.
J Neural Transm
monoaminergic metabolites
and demented
patientsCarwith
203. Loeffler
DA, DeMaggio
Juneau PL,
et al. Ceruloplasmin
is
Parkinson’s
disease--effect
of L-Dopa.
Neural cerebrospinal
Transm 1996;
increased
in cerebrospinal fluid in Alzheimer’s disease but not
taya
L. Monoamine
metabolites
in normalJ human
1998;105:39–51.
103:591–602.
fluid
and in degenerative diseases of the central nervous system.
disease.T,Alzheimer
Dis Assoc
205.Parkinson’s
Isobe C, Murata
Sato C, Terayama
Y. Disord
Increase1994;8:190–
of oxidized/
Estud Med
1993;41:13–19.
197.
total coenzyme Q-10 ratio in cerebrospinal fluid in patients with
186.Bol
Kanemaru
K, Biol
Mitani
K, Yamanouchi H. Cerebrospinal fluid
185. Strittmatter
M, acid
Hamann
D, Cramer
H, Schimrigk
Parkinson’s
disease.
J Clin Neurosci
2007;14:340–343.
homovanillic
levelsGF,
areStrubel
not reduced
in early
corticobasal
204. Eder
U, Leitner
B, Kirchmair
R, et al.
Levels and proteolytic
Neurosci
Lett 1998;245:121–122.
of chromogranin
B and secretogranin
II in
K.degeneration.
Somatostatin-like
immunoreactivity,
its molecular forms and
206.processing
Ernst A, Cramer
H, StrubelAD,and
Kuntzmann
F, Schoenenberger
cerebrospinal
fluid of
in DSIPneurological
diseases. J Neural
Transm
metabolites
and demented
patients
with
GA. Comparison
(delta sleep-inducing
peptide)
and P187.monoaminergic
Moser A, Scholz
J, NobbeinF,aged
Vieregge
P, Bohme
V, Bamberg
Parkinson’s
disease--effect
of L-Dopa. J inNeural
Transm
1996;
1998;105:39–51.
DSIP-like (phosphorylated) immunoreactivity in cerebrospinal
H. Presence
of N-methyl-norsalsolinol
the CSF:
correlations
103:591–602.
fluidC,
of Murata
patientsT,with
dementia Y.
of Increase
Alzheimer
multiwith dopamine metabolites of patients with Parkinson’s disease.
205. Isobe
Satosenile
C, Terayama
of type,
oxidized/
infarct
syndrome,
hydrocephalus
and ParkinJ Neurol Sci
total
coenzyme
Q-10 communicating
ratio in cerebrospinal
fluid in patients
with
186. Kanemaru
K, 1995;131:183–189.
Mitani K, Yamanouchi H. Cerebrospinal fluid
son’s disease.
J Neurol
Parkinson’s
disease.
J Clin1987;235:16–21.
Neurosci 2007;14:340–343.
acid levels
are not reduced
in early corticobasalL,
188.homovanillic
Krygowska-Wajs
A, Szczudlik
A, Antkiewicz-Michaluk
degeneration.
1998;245:121–122.
207.Ernst
Waragai
M, WeiH,J,Strubel
Fujita M,
al. Increased
level of DJ-1 in
Romanska I,Neurosci
Vetulani Lett
J. Salsolinol,
3-O-methyl-dopa and homo206.
A, Cramer
D, et
Kuntzmann
F, Schoenenberger
the Comparison
cerebrospinal
sporadic
Parkinson’s
disease.
vanillic
in J,the
cerebrospinal
fluidP, of
Parkinson
patients.
GA.
of fluids
DSIP- of
(delta
sleep-inducing
peptide)
and BioP187. Moser
A, acid
Scholz
Nobbe
F, Vieregge
Bohme
V, Bamberg
chem Biophys
Res Communimmunoreactivity
2006;345:967–972.
Neurochir
Pol 1997;31:875–885.
DSIP-like
(phosphorylated)
in cerebrospinal
H.Neurol
Presence
of N-methyl-norsalsolinol
in the CSF: correlations
of patients
with senile
dementia
of Alzheimer
type, multidopamine metabolites
of patientsBD,
withCurzon
Parkinson’s
disease.
208.fluid
Hagihara
M, Mihara
R, Togari
A, Nagatsu
T. Dipeptidyl-amino189.with
Godwin-Austen
RB. Kantamaneni
G: Comparison
infarct
syndrome,
communicating
hydrocephalus
andinParkinJ Neurol
Scifrom
1995;131:183–189.
peptidase
II in human
cerebrospinal
fluid: changes
patients
of benefit
L-dopa in Parkinsonism with increase of amine
son’s
J Neurol
1987;235:16–21.
withdisease.
Parkinson’s
disease.
Biochem Med Metab Biol 1987;37:
metabolites in theA,CSF.
J Neurol A,
Neurosurg
Psychiatry 1971;34:
188. Krygowska-Wajs
Szczudlik
Antkiewicz-Michaluk
L,
360–365.
219–223. I, Vetulani J. Salsolinol, 3-O-methyl-dopa and homo207. Waragai
M, Wei J, Fujita M, et al. Increased level of DJ-1 in
Romanska
cerebrospinal
Parkinson’s
disease.
BioacidDowson
in the JH,
cerebrospinal
209.theBoll
MC, Sotelo J,fluids
OteroofE, sporadic
Alcaraz-Zubeldia
M, Rios
C. Reduced
190.vanillic
Pullar IA,
Ahmed R, fluid
ChowofR,Parkinson
Gillinghampatients.
FJ. Biochem
Biophysactivity
Res Commun
2006;345:967–972.
Neurol
Neurochir
Pol 1997;31:875–885.
ferroxidase
in the cerebrospinal
fluid from patients with
chemical
investigations
in Parkinsonism. A study of the metaboParkinson’s
disease.R,
Neurosci
1999;265:155–158.
lites of the biogenic
amines in the
lumbar
CSF.
Neurol
208. Hagihara
M, Mihara
Togari Lett
A, Nagatsu
T. Dipeptidyl-amino189. Godwin-Austen
RB. Kantamaneni
BD,
Curzon
G: Confin
Comparison
II inMulder
humanC,cerebrospinal
fluid:
changes
patients
of1972;34:143–148.
benefit from L-dopa in Parkinsonism with increase of amine
210.peptidase
Kuiper MA,
van Kamp GJ,
Scheltens
P, in
Wolters
EC.
with
Parkinson’sfluid
disease.
Biochem
Metab with
Biol Parkinson’s
1987;37:
the CSF.
J Neurol
NeurosurgG.Psychiatry
1971;34:
Cerebrospinal
ferritin
levels Med
of patients
191.metabolites
Cheng FC,inKuo
JS, Chia
LG, Dryhurst
Elevated 5-S-cystei360–365.
219–223.
disease, Alzheimer’s disease, and multiple system atrophy.
nyldopamine/homovanillic acid ratio and reduced homovanillic
1424
MOLLENHAUER
209.
Boll
MC, Sotelo
J, Otero
E, Alcaraz-Zubeldia
M, Rios C. Reduced
J Neural
Transm
Park Dis
Dement SectB.1994;7:109–114.
acid IA,
in cerebrospinal
fluid: possible
for andFJ.
potential
190. Pullar
Dowson JH, Ahmed
R, Chowmarkers
R, Gillingham
Bioinsights investigations
into the pathoetiology
of Parkinson’s
J Neural
in A,
theVidailhet
cerebrospinal
from patients
with
chemical
in Parkinsonism.
A studydisease.
of the metabo211.ferroxidase
Dexter DT,activity
Carayon
M, et fluid
al. Decreased
ferritin
levTransm
Parkinson’s
Neuroscidisease.
Lett 1999;265:155–158.
lites
of the1996;103:433–446.
biogenic amines in the lumbar CSF. Confin Neurol
els in braindisease.
in Parkinson’s
J Neurochem 1990;55:16–20.
1972;34:143–148.
210.
MA,K,Mulder
C, vanK,Kamp
GJ, Scheltens
P, Wolters
EC.
212.Kuiper
Aoyama
Matsubara
Kobayashi
S. Aging
and oxidative
Cerebrospinal
fluid ferritin
levels ofpalsy.
patients
Parkinson’s
stress in progressive
supranuclear
Eur with
J Neurol
2006;13:
191. Cheng FC, Kuo JS, Chia LG, Dryhurst G. Elevated 5-S-cysteidisease,
89–92. Alzheimer’s disease, and multiple system atrophy.
nyldopamine/homovanillic acid ratio and reduced homovanillic
DIAGNOSTICS IN MOVEMENT
1423
Park Dis
Dement Sect
acid inDISORDERS
cerebrospinal fluid: possible markers for and potential
213.J Neural
Gomez Transm
JM, Aguilar
M, Navarro
MA,1994;7:109–114.
Ortola J, Soler J. SecreMovement
Vol. 24,ferritin
No. 10,lev2009
insights into the pathoetiology of Parkinson’s disease. J Neural
211. Dexter
DT,growth
Carayonhormone
A, Vidailhet
etDisorders,
al. Decreased
tion of
and M,
thyroid-stimulating
hormone
in
Transm 1996;103:433–446.
elspatients
in brainwith
in Parkinson’s
disease.
J Neurochem
1990;55:16–20.
dementia. Clin
Investig
1994;72:489–493.
bert ML, Langlias PJ,
192. Kuhn W, Muller T, Gerlach M, et al. Depression in Parkinson’s
214. Sjogren M, Minthon L, Davidsson P, et al. CSF levels of tau,
etic acid in CSF. Difdisease: biogenic amines in CSF of ‘‘de novo’’ patients. J Neubeta-amyloid(1-42) and GAP-43 in frontotemporal dementia,
a of the Alzheimer’s
ral Transm 1996;103:1441–1445.
other types of dementia and normal aging. J Neural Transm
2000;107:563–579.
193. Zhou G, Shoji H, Yamada S, Matsuishi T. Decreased betaMovement
Disorders, Vol. 24,
No. 10, 2009
monoamine metabolite
phenylethylamine in CSF in Parkinson’s disease. J Neurol Neu215. Kuhn W, Muller T, Grosse
H, Rommelspacher
H. Elevated
levisease. Arch Neurol14
rosurg Psychiatry 1997;63:754–758.
els of harman and norharman in cerebrospinal fluid of parkinsonian patients. J Neural Transm 1996;103:1435–1440.
194. Botez MI, Young SN. Biogenic amine metabolites and thiamine
in cerebrospinal fluid in heredo-degenerative ataxias. Can J
Cerebrospinal fluid
216. Isobe C, Murata T, Sato C, Terayama Y. Increase of total hoHuntington’s disease.
mocysteine concentration in cerebrospinal fluid in patients with
Neurol Sci 2001;28:134–140.
Alzheimer’s disease and Parkinson’s disease. Life Sci 2005;77:
195. Abdo WF, van de Warrenburg BP, Munneke M, et al. CSF
1836–1843.
analysis differentiates multiple-system atrophy from idiopathic
bo H, Muramoto S,
late-onset cerebellar ataxia. Neurology 2006;67:474–479.
A in parkinsonian
217. Blum-Degen D, Muller T, Kuhn W, Gerlach M, Przuntek H,
AND C. TRENKWALD
234. Williams A, B
Aging and CSF
1246.
235. Kahle PJ, Jakow
tau and neuron
Neurology 2000
236. Yamada T, Ch
Concentration
from progressiv
Jpn J Psychiatry
237. de Jong D, Jan
nal fluid amylo
between Alzhei
A Biol Sci Med
238. Rosengren LE,
C. Patients wit
degenerative d
protein in CSF.
MOLLENHAUER
Aging and oxidative
ur J Neurol 2006;13:
ola J, Soler J. Secremulating hormone in
72:489–493.
l. CSF levels of tau,
otemporal dementia,
ng. J Neural Transm
cher H. Elevated levnal fluid of parkinso435–1440.
Increase of total hofluid in patients with
se. Life Sci 2005;77:
ach M, Przuntek H,
kin-6 are elevated in
de novo Parkinson’s
–20.
uhn W. Interleukin-6
relate to severity of
98;98:142–144.
89–92.
1246.
1424
B.Ortola
MOLLENHAUER
213. Gomez JM, Aguilar M, Navarro MA,
J, Soler J. Secre-AND C.
235.TRENKWALDER
Kahle PJ, Jakowec M, Teipel SJ, et al. Combined assessment of
tion of growth hormone and thyroid-stimulating hormone in
patients with dementia. Clin Investig 1994;72:489–493.
214.Aoyama
Sjogren K,
M, Matsubara
Minthon L,K,Davidsson
et Aging
al. CSFand
levels
of tau,
212.
KobayashiP, S.
oxidative
beta-amyloid(1-42)
and GAP-43palsy.
in frontotemporal
dementia,
stress
in progressive supranuclear
Eur J Neurol 2006;13:
other types of dementia and normal aging. J Neural Transm
89–92.
2000;107:563–579.
213. Gomez
JM, Aguilar M, Navarro MA, Ortola J, Soler J. Secre215.tion
Kuhn
Mullerhormone
T, Grosse
H, thyroid-stimulating
Rommelspacher H. Elevated
of W,
growth
and
hormone levin
els of harman
and norharman
in cerebrospinal
fluid of parkinsopatients
with dementia.
Clin Investig
1994;72:489–493.
nian patients.
J Neural
1996;103:1435–1440.
214. Sjogren
M, Minthon
L, Transm
Davidsson
P, et al. CSF levels of tau,
216.beta-amyloid(1-42)
Isobe C, Murata T,and
SatoGAP-43
C, Terayama
Y. Increase ofdementia,
total hoin frontotemporal
mocysteine
concentration
in cerebrospinal
in patients
with
other
types of
dementia and
normal aging.fluid
J Neural
Transm
2000;107:563–579.
Alzheimer’s disease and Parkinson’s disease. Life Sci 2005;77:
1836–1843.
215. Kuhn
W, Muller T, Grosse H, Rommelspacher H. Elevated lev217.els
Blum-Degen
D, Muller
T, Kuhn
W, Gerlachfluid
M, ofPrzuntek
of harman and
norharman
in cerebrospinal
parkinso-H,
Riederer
P. Interleukin-1
beta 1996;103:1435–1440.
and interleukin-6 are elevated in
nian
patients.
J Neural Transm
the cerebrospinal
andIncrease
de novoofParkinson’s
216. Isobe
C, Murata T,fluid
SatoofC,Alzheimer’s
Terayama Y.
total hodisease patients.
NeurosciinLett
1995;202:17–20.
mocysteine
concentration
cerebrospinal
fluid in patients with
218.Alzheimer’s
Muller T, Blum-Degen
D, Przuntek disease.
H, KuhnLife
W.Sci
Interleukin-6
disease and Parkinson’s
2005;77:
levels in cerebrospinal fluid inversely correlate to severity of
1836–1843.
Parkinson’s disease.
Acta
1998;98:142–144.
217. Blum-Degen
D, Muller
T,Neurol
Kuhn Scand
W, Gerlach
M, Przuntek H,
219.Riederer
Gomez-Tortosa
E, Gonzalo
S, et al.areCerebrospinal
P. Interleukin-1
beta I,
andFanjul
interleukin-6
elevated in
the
cerebrospinal
fluid of Alzheimer’s
and decompared
novo Parkinson’s
fluid
markers in dementia
with lewy bodies
with Alzheimerpatients.
disease. Neurosci
Arch Neurol
disease
Lett2003;60:1218–1222.
1995;202:17–20.
220.Muller
Montine
Quinn JF,D,Zhang
J, et H,
al. Kuhn
Isoprostanes
and related
218.
T, KS,
Blum-Degen
Przuntek
W. Interleukin-6
products
of lipid peroxidation
in neurodegenerative
diseases.
levels
in cerebrospinal
fluid inversely
correlate to severity
of
Chem Physdisease.
Lipids 2004;128:117–124.
Parkinson’s
Acta Neurol Scand 1998;98:142–144.
219.
E, Gonzalo
I, FanjulE,S,et et
Cerebrospinal
221.Gomez-Tortosa
Balducci C, Pierguidi
L, Persichetti
al. al.
Lysosomal
hydrolasesmarkers
in cerebrospinal
fluid
from
Parkinson’s
disfluid
in dementia
with
lewysubjects
bodies with
compared
with Alzease. Mov
Disord
2007;22:1481–1484.
heimer
disease.
Arch
Neurol 2003;60:1218–1222.
222.Montine
AlimontiKS,
A, Quinn
Bocca JF,
B, Pino
F, Forte G,and
Sancesario
220.
ZhangA,J,Ruggieri
et al. Isoprostanes
related
G. Elemental
profile
of cerebrospinal
fluid in patients diseases.
with Parproducts
of lipid
peroxidation
in neurodegenerative
Chem
Physdisease.
Lipids J2004;128:117–124.
kinson’s
Trace Elem Med Biol 2007;21:234–241.
223.Balducci
Qureshi C,
GA,
QureshiL,AA,
Memon E,SA,
Parvez
SH. Impact
221.
Pierguidi
Persichetti
et al.
Lysosomal
hydro-of
selenium,
iron, copper
andfrom
zincsubjects
in on/off
Parkinson’s
patients
lases
in cerebrospinal
fluid
with
Parkinson’s
dison L-dopa
therapy.
J Neural Transm Suppl 2006:229–236.
ease.
Mov Disord
2007;22:1481–1484.
224.Alimonti
Forte G, A,
Bocca
B, B,
Senofonte
et al. Trace
and major
elements
222.
Bocca
Pino A,O,Ruggieri
F, Forte
G, Sancesario
G.in Elemental
profile
of cerebrospinal
patients
with
Parwhole blood,
serum,
cerebrospinalfluid
fluidinand
urine of
patients
with Parkinson’s
disease.
Neural
2004;111:1031–
kinson’s
disease. J Trace
ElemJ Med
BiolTransm
2007;21:234–241.
1040. GA, Qureshi AA, Memon SA, Parvez SH. Impact of
223. Qureshi
225.selenium,
Jimenez-Jimenez
FJ, Molina
JA, in
Aguilar
et al. Cerebrospiiron, copper
and zinc
on/offMV,
Parkinson’s
patients
nalL-dopa
fluid levels
of Jtransition
metals Suppl
in patients
with Parkinson’s
on
therapy.
Neural Transm
2006:229–236.
disease.
J Neural
1998;105:497–505.
224. Forte
G, Bocca
B, Transm
Senofonte
O, et al. Trace and major elements
226.inGazzaniga
GC, serum,
Ferrarocerebrospinal
B, Camerlingo
M, and
Casto
L, Viscardi
M,
whole blood,
fluid
urine
of patients
Mamoli
A. A case
control
study ofTransm
CSF copper,
iron and
with
Parkinson’s
disease.
J Neural
2004;111:1031–
manganese in Parkinson disease. Ital J Neurol Sci 1992;13:239–
1040.
243.
225. Jimenez-Jimenez
FJ, Molina JA, Aguilar MV, et al. Cerebrospilevels of transition
metals
in patients
Parkinson’s
227.nal
Ilicfluid
T, Jovanovic
M, Jovicic
A, Tomovic
M.with
Oxidative
stress
and Parkinson’s
disease. 1998;105:497–505.
Vojnosanit Pregl 1998;55:463–468.
disease.
J Neural Transm
228.Gazzaniga
Kjellin KG.
CSFB,iron
in patients
dis226.
GC,The
Ferraro
Camerlingo
M, with
Castoneurological
L, Viscardi M,
eases. Acta
Neurol
1967;43:299–313.
Mamoli
A. A
case Scand
control
study of CSF copper, iron and
Parkinson
Ital J Neurol
1992;13:239–
229.manganese
Bostrom F,inHansson
O,disease.
Gerhardsson
L, et al.Sci
CSF
Mg and Ca
243.
as diagnostic markers for dementia with Lewy bodies. NeurobiolT,Aging
2008. M, Jovicic A, Tomovic M. Oxidative stress
227. Ilic
Jovanovic
Parkinson’s
disease.
Vojnosanit
Pregl
1998;55:463–468.
230.and
Polinsky
RJ, Holmes
KV,
Brown RT,
Weise
V. CSF acetylcholinesterase
are reduced
multiple
atrophy diswith
228. Kjellin
KG. levels
The CSF
iron in in
patients
withsystem
neurological
autonomic
failure. Scand
Neurology
1989;39:40–44.
eases.
Acta Neurol
1967;43:299–313.
231.Bostrom
Sandyk F,
R, Hansson
Snider SR.
CSF Met-enkephalin
levelsMgin and
Parkin229.
O, Gerhardsson
L, et al. CSF
Ca
disease.markers
Neurology
asson’s
diagnostic
for 1985;35:776–777.
dementia with Lewy bodies. NeuroAging
232.biol
Moser
A, 2008.
Kompf D. Presence of methyl-6,7-dihydroxy-1,2,3,4tetrahydroisoquinolines,
the neurotoxin
isoquino230. Polinsky
RJ, Holmes KV,derivatives
Brown RT,ofWeise
V. CSF acetylcholine, in parkinsonian
Life Scisystem
1992;50:1885–1891.
linesterase
levels are lumbar
reducedCSF.
in multiple
atrophy with
failure.
Neurology
1989;39:40–44.
233.autonomic
Fujishiro K,
Hagihara
M, Takahashi
A, Nagatsu T. Concentrations ofR,neopterin
and CSF
biopterin
in the cerebrospinal
fluid of
231. Sandyk
Snider SR.
Met-enkephalin
levels in Parkinpatients
withNeurology
Parkinson’s
disease. Biochem Med Metab Biol
son’s
disease.
1985;35:776–777.
1990;44:97–100.
232. Moser
A, Kompf D. Presence of methyl-6,7-dihydroxy-1,2,3,4tetrahydroisoquinolines, derivatives of the neurotoxin isoquinoline, in parkinsonian lumbar CSF. Life Sci 1992;50:1885–1891.
233. Fujishiro K, Hagihara M, Takahashi A, Nagatsu T. ConcentraAND C. TRENKWALDER
tions of neopterin and biopterin in the cerebrospinal fluid of
Movement
Disorders,
Vol. 24, No. 10,
2009 Biochem Med Metab Biol
patients
with Parkinson’s
disease.
1990;44:97–100.
234. Williams A, Ballenger J, Levine R, Lovenberg W, Calne D.
Aging and CSF hydroxylase cofactor. Neurology 1980;30:1244–
1246.
235. Kahle PJ, Jakowec M, Teipel SJ, et al. Combined assessment of
Movement
Disorders,
Vol. 24,
No. 10,
2009 in Alzheimer’s disease CSF.
tau and
neuronal
thread
protein
Neurology 2000;54:1498–1504.
236. Yamada T, Chong JK, Asahina M, Koguchi Y, Hirayama K.
Concentration of neural thread protein in cerebrospinal fluid
from progressive supranuclear palsy and Parkinson’s disease.
Jpn J Psychiatry Neurol 1993;47:631–635.
237. de Jong D, Jansen RW, Kremer BP, Verbeek MM. Cerebrospinal fluid amyloid beta42/phosphorylated tau ratio discriminates
between Alzheimer’s disease and vascular dementia. J Gerontol
A Biol Sci Med Sci 2006;61:755–758.
238. Rosengren LE, Karlsson JE, Karlsson JO, Persson LI, Wikkelso
C. Patients with amyotrophic lateral sclerosis and other neurodegenerative diseases have increased levels of neurofilament
protein in CSF. J Neurochem 1996;67:2013–2018.
239. Brettschneider J, Petzold A, Sussmuth SD, et al. Neurofilament
heavy-chain NfH(SMI35) in cerebrospinal fluid supports the differential diagnosis of Parkinsonian syndromes. Mov Disord
2006;21:2224–2227.
240. Jolkkonen J, Hartikainen P, Soikkeli R, Bissette G, Nemeroff C,
Riekkinen P. A correlation study of CSF neuropeptides in Alz-
tau and neuronal thread protein in Alzheimer’s disease CSF.
Neurology 2000;54:1498–1504.
236.Williams
Yamada A,
T, Chong
JK,J,Asahina
Koguchi Y,W,
Hirayama
234.
Ballenger
Levine M,
R, Lovenberg
Calne D.K.
Aging
and CSF hydroxylase
cofactor.
Neurology
1980;30:1244–
Concentration
of neural thread
protein
in cerebrospinal
fluid
1246.
from progressive supranuclear palsy and Parkinson’s disease.
Jpn J PJ,
Psychiatry
1993;47:631–635.
235. Kahle
JakowecNeurol
M, Teipel
SJ, et al. Combined assessment of
B. Mollenhauer
andMM.
C. disease
Trenkwalder
237.tau
de and
Jong neuronal
D, Jansenthread
RW, Kremer
BP,
Verbeek
Cerebrospiprotein
in Alzheimer’s
CSF.
nal fluid amyloid
beta42/phosphorylated tau ratio discriminates
Neurology
2000;54:1498–1504.
betweenT,
Alzheimer’s
andM,
vascular
dementia.
J Gerontol
236. Yamada
Chong JK,disease
Asahina
Koguchi
Y, Hirayama
K.
A Biol Sci Med
2006;61:755–758.
Concentration
of Sci
neural
thread protein in cerebrospinal fluid
238.from
Rosengren
LE, Karlsson
JE, Karlsson
JO, Parkinson’s
Persson LI, Wikkelso
progressive
supranuclear
palsy and
disease.
C. JPatients
withNeurol
amyotrophic
lateral sclerosis and other neuroJpn
Psychiatry
1993;47:631–635.
diseases
increased
levelsMM.
of neurofilament
237. dedegenerative
Jong D, Jansen
RW, have
Kremer
BP, Verbeek
Cerebrospiprotein
CSF. J beta42/phosphorylated
Neurochem 1996;67:2013–2018.
nal
fluid in
amyloid
tau ratio discriminates
239.between
Brettschneider
J, Petzold
A, and
Sussmuth
SD,dementia.
et al. Neurofilament
Alzheimer’s
disease
vascular
J Gerontol
NfH(SMI35)
in cerebrospinal fluid supports the difAheavy-chain
Biol Sci Med
Sci 2006;61:755–758.
ferential diagnosis
of JE,
Parkinsonian
syndromes.
Mov
Disord
238. Rosengren
LE, Karlsson
Karlsson JO,
Persson LI,
Wikkelso
C.2006;21:2224–2227.
Patients with amyotrophic lateral sclerosis and other neuro240.degenerative
Jolkkonen J, diseases
Hartikainen
P, Soikkeli
Bissette
Nemeroff C,
have
increasedR,levels
of G,
neurofilament
Riekkinen
P. AJ correlation
of CSF neuropeptides in Alzprotein
in CSF.
Neurochemstudy
1996;67:2013–2018.
heimer’s and J,Parkinson’s
1991;19:97–
239. Brettschneider
Petzold A, disease.
SussmuthNeuropeptides
SD, et al. Neurofilament
102.
heavy-chain
NfH(SMI35) in cerebrospinal fluid supports the dif241.ferential
Dupont E,
Christensen
SE, Hansen syndromes.
AP, de FineMov
Olivarius
diagnosis
of Parkinsonian
DisordB,
Orskov H. Low cerebrospinal fluid somatostatin in Parkinson
2006;21:2224–2227.
disease: an
irreversible P,abnormality.
Neurology
1982;32:312–
240. Jolkkonen
J, Hartikainen
Soikkeli R, Bissette
G, Nemeroff
C,
314.
Riekkinen
P. A correlation study of CSF neuropeptides in AlzParkinson’s
disease. MF,
Neuropeptides
242.heimer’s
Beal MF,and
Growdon
JH, Mazurek
Martin JB. 1991;19:97–
CSF somatostatin-like immunoreactivity in dementia. Neurology 1986;36:
102.
294–297.
241. Dupont
E, Christensen SE, Hansen AP, de Fine Olivarius B,
somatostatin
in Parkinson
243.Orskov
Poewe H.
W, Low
Benkecerebrospinal
T, Karamat E,fluid
Schelosky
L, Wagner
M, Sperk
disease:
irreversible abnormality.
Neurology
1982;32:312–
G. CSF an
somatostatin-like
immunoreactivity
in dementia
of Parkinson’s disease. J Neurol Neurosurg Psychiatry 1990;53:1105–
314.
1106.MF, Growdon JH, Mazurek MF, Martin JB. CSF somato242. Beal
in dementia.
244.statin-like
Espino A,immunoreactivity
Calopa M, Ambrosio
S, OrtolaNeurology
J, Peres J,1986;36:
Navarro
294–297.
MA. CSF somatostatin increase in patients with early parkinsonian syndrome.
Transm
Park Dis L,
Dement
Sect
243. Poewe
W, Benke JT,Neural
Karamat
E, Schelosky
Wagner
M, 1995;9:
Sperk
G.189–196.
CSF somatostatin-like immunoreactivity in dementia of Pardisease. J FJ,
Neurol
Neurosurg
Psychiatry
1990;53:1105–
245.kinson’s
Jimenez-Jimenez
Molina
JA, Vargas
C, et al.
Normal cere1106.
brospinal fluid levels of insulin in patients with Parkinson’s disease. J A,
Neural
Transm
2000;107:445–449.
244. Espino
Calopa
M, Ambrosio
S, Ortola J, Peres J, Navarro
CSF somatostatin
increase
in patients
with early
parkinso246.MA.
Sundquist
J, Forsling ML,
Olsson
JE, Akerlund
M. Cerebrospinian
J Neural
Transm Park
Dis Dement disorders
Sect 1995;9:
nal syndrome.
fluid arginine
vasopressin
in degenerative
and
189–196.
other neurological diseases. J Neurol Neurosurg Psychiatry
1983;46:14–17. FJ, Molina JA, Vargas C, et al. Normal cere245. Jimenez-Jimenez
247.brospinal
Nappi G,fluid
Petraglia
F, insulin
Martignoni
E, Facchinetti
F, Bonodis-G,
levels of
in patients
with Parkinson’s
ease.
J Neural
Transm
2000;107:445–449.
Genazzani
AR.
beta-Endorphin
cerebrospinal fluid decrease in
untreated J,parkinsonian
patients.
1985;35:1371–1374.
246. Sundquist
Forsling ML,
OlssonNeurology
JE, Akerlund
M. Cerebrospi248.nal
Jolkkonen
JT, Soininen
HS, Riekkinen
PJ. beta-Endorphin-like
fluid arginine
vasopressin
in degenerative
disorders and
immunoreactivity
cerebrospinal
fluid of
patients with
Alzheiother
neurological indiseases.
J Neurol
Neurosurg
Psychiatry
1983;46:14–17.
mer’s disease and Parkinson’s disease. J Neurol Sci 1987;77:
153–159.
247. Nappi
G, Petraglia F, Martignoni E, Facchinetti F, Bono G,
249.Genazzani
Nutt JG, AR.
Mroxbeta-Endorphin
EA, Leeman cerebrospinal
SE, Williams fluid
AC, decrease
Engel WK,
in
Chase TN.
Substance P
in human
cerebrospinal
fluid: reductions
untreated
parkinsonian
patients.
Neurology
1985;35:1371–1374.
in peripheral
andRiekkinen
autonomicPJ.
dysfunction.
Neurology
248. Jolkkonen
JT, neuropathy
Soininen HS,
beta-Endorphin-like
1980;30:1280–1285.
immunoreactivity
in cerebrospinal fluid of patients with Alzhei250.mer’s
Litvandisease
I, Berrettini
WH, Atack disease.
JR, Chase
TN. CSF
and
and Parkinson’s
J Neurol
Scigalanin
1987;77:
neuropeptide Y immunoreactivity in progressive supranuclear
153–159.
palsy.JG,
Acta
Neurol
1992;86:204–206.
249. Nutt
Mrox
EA,Scand
Leeman
SE, Williams AC, Engel WK,
TN.GA,
Substance
in human
cerebrospinal
fluid: reductions
251.Chase
Qureshi
Baig S,PBednar
I, Sodersten
P, Forsberg
G, Siden
Increasedneuropathy
cerebrospinal
concentration
of nitrite
in ParinA.peripheral
andfluid
autonomic
dysfunction.
Neurology
kinson’s disease. Neuroreport 1995;6:1642–1644.
1980;30:1280–1285.
250.
Berrettini
Atack JR,N,
Chase
TN. CSF
252.Litvan
ShuklaI, R,
Rajani WH,
M, Srivastava
Barthwal
MK,galanin
Dikshitand
M.
IN
neuropeptide
Y immunoreactivity
inCSF
progressive
supranuclear
Nitrite and malondialdehyde
content
in DIAGNOSTICS
cerebrospinal
fluid of
palsy.
Actawith
Neurol
Scand 1992;86:204–206.
patients
Parkinson’s
disease. Int J Neurosci 2006;116:
1391–1402.
251. Qureshi
GA, Baig S, Bednar I, Sodersten P, Forsberg G, Siden
253.A.Molina
JA, Jimenez-Jimenez
Navarro JA, of
et nitrite
al. CerebrospiIncreased
cerebrospinal fluidFJ,concentration
in Parnal fluiddisease.
nitrate levels
in patients
with Parkinson’s disease. Acta
kinson’s
Neuroreport
1995;6:1642–1644.
NeurolR,
Scand
1996;93:123–126.
252. Shukla
Rajani
M, Srivastava N, Barthwal MK, Dikshit M.
254.Nitrite
Baumann
Dauvilliers Y,content
MignotinE,cerebrospinal
Bassetti CL.fluid
Normal
and CR,
malondialdehyde
of
CSF hypocretin-1
(orexin disease.
A) levels
Lewy
patients
with Parkinson’s
Int inJ dementia
Neurosci with
2006;116:
bodies associated with excessive daytime sleepiness. Eur Neurol
1391–1402.
2004;52:73–76.
255. Martinez-Rodriguez JE, Seppi K, Cardozo A, et al. Cerebrospinal fluid hypocretin-1 levels in multiple system atrophy. Mov
Disord 2007;22:1822–1824.
256. Van Everbroeck B, Dobbeleir I, De Waele M, De Deyn P,
Martin JJ, Cras P. Differential diagnosis of 201 possible
Creutzfeldt-Jakob disease patients. J Neurol 2004;251:298–
304.
257. Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF
14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob
disease. Neurology 2000;55:811–815.
258. Burkhard PR, Sanchez JC, Landis T, Hochstrasser DF. CSF
detection of the 14-3-3 protein in unselected patients with dementia. Neurology 2001;56:1528–1533.
259. Tschampa HJ, Neumann M, Zerr I, et al. Patients with Alzheimer’s disease and dementia with Lewy bodies mistaken for
Creutzfeldt-Jakob disease. J Neurol Neurosurg Psychiatry 2001;
71:33–39.
260. Botella-Lopez A, Burgaya F, Gavin R, et al. Reelin expression
and glycosylation patterns are altered in Alzheimer’s disease.
Proc Natl Acad Sci USA 2006;103:5573–5578.
261. Mollenhauer B, Bibl M, Trenkwalder C, et al. Follow-up investigations in cerebrospinal fluid of patients with dementia with
Lewy bodies and Alzheimer’s disease. J Neural Transm 2005;
MOVEMENT DISOR
272. Mitani K, Furi
protein in cor
44–46.
273. Hampel H, Bue
phosphorylated
heimer disease:
Gen Psychiatry
274. Vanderstichele H
performance and
TAU181P assay
and dementia w
1472–1480.
275. Wada-Isoe K, K
tic markers for
and MIBG card
33–37.
276. Mogi M, Hara
Nagatsu T. Tum
both in the brai
nian patients. Ne
277. Vermes I, Steur
centration of ce
kinson’s diseas
15 1252–1254.
278. Tohgi H, Abe T
thine concentrat
vascular dement
mentia, and Pa
Dement Sect 19
279. Jimenez-Jimenez
fluid
hypocretin-1
levels in
multiple
systemof atrophy.
performance
clinical
utility ofstudy.
the INNOTEST
PHOSPHOand MIBG and
cardiac
scintigraphy
J Neurol Sci
2007;260:
257.nal
Zerr
I, Pocchiari
M, Collins
S, et
al. Analysis
EEG andMov
CSF
Disord
TAU181P
33–37. assay for discrimination between Alzheimer’s disease
14-3-32007;22:1822–1824.
proteins as aids to the diagnosis of Creutzfeldt-Jakob
dementia
with Lewy
bodies. Clin
Chem Lab Med
256. Van
Everbroeck
B, 2000;55:811–815.
Dobbeleir I, De Waele M, De Deyn P,
disease.
Neurology
276.and
Mogi
M, Harada
M, Riederer
P, Narabayashi
H, 2006;44:
Fujita K,
1472–1480.
JJ, PR,
CrasSanchez
P. Differential
diagnosis
of 201 possible
Nagatsu T. Tumor necrosis factor-alpha (TNF-alpha) increases
258.Martin
Burkhard
JC, Landis
T, Hochstrasser
DF. CSF
Creutzfeldt-Jakob
diseaseprotein
patients.
J Neurol patients
2004;251:298–
275. Wada-Isoe
Kitayama
Nakaso
K, Nakashima
K. Diagnosboth in theK,brain
and inM,the
cerebrospinal
fluid from
parkinsodetection of the 14-3-3
in unselected
with de304.
ticnian
markers
forNeurosci
diagnosing
with Lewy bodies: CSF
patients.
Lett dementia
1994;165:208–210.
mentia. Neurology 2001;56:1528–1533.
MIBGI, cardiac
scintigraphy
J NeurolC.Sci
2007;260:
257.
I, Pocchiari
M, CollinsM,S,Zerr
et al.I, Analysis
of EEG
andAlzheiCSF
277.and
Vermes
Steur EN,
Jirikowskistudy.
GF, Haanen
Elevated
con259.Zerr
Tschampa
HJ, Neumann
et al. Patients
with
33–37.
14-3-3
as aids
to the with
diagnosis
Creutzfeldt-Jakob
centration of cerebrospinal fluid tissue transglutaminase in Parmer’s proteins
disease and
dementia
Lewy ofbodies
mistaken for
運動障害の鑑別診断における神経化学的バイオマーカー
disease.
Neurology disease.
2000;55:811–815.
276. Mogi
M, Harada
Riedererapoptosis.
P, Narabayashi
H, Fujita
K,
kinson’s
disease M,
indicating
Mov Disord
2004;19:
Creutzfeldt-Jakob
J Neurol Neurosurg Psychiatry 2001;
Nagatsu
T. Tumor necrosis factor-alpha (TNF-alpha) increases
258. Burkhard
1252–1254.
71:33–39.PR, Sanchez JC, Landis T, Hochstrasser DF. CSF
in H,
the Abe
brainT,and
in the cerebrospinal
of theA,
14-3-3
protein
in unselected
with de278.both
Tohgi
Takahashi
S, Kikuchi T.fluid
Thefrom
urateparkinsoand xan260.detection
Botella-Lopez
Burgaya
F, Gavin
R, et al. patients
Reelin expression
nian
NeurosciinLett
mentia.
Neurology 2001;56:1528–1533.
thinepatients.
concentrations
the1994;165:208–210.
cerebrospinal fluid in patients with
and glycosylation
patterns are altered in Alzheimer’s disease.
277. Vermes
Steur EN,ofJirikowski
GF, Haanen
C. Elevated
con259. Tschampa
Neumann
Zerr I, et al. Patients with AlzheivascularI, dementia
the Binswanger
type, Alzheimer
type
deProc Natl HJ,
Acad
Sci USAM,
2006;103:5573–5578.
centration
of cerebrospinal
fluid tissue
transglutaminase
in Pardisease B,
and
dementia
with Lewy
mistakeninvesfor
mentia, and
Parkinson’s disease.
J Neural
Transm Park
Dis
261.mer’s
Mollenhauer
Bibl
M, Trenkwalder
C, etbodies
al. Follow-up
kinson’s
disease
indicating apoptosis. Mov Disord 2004;19:
Creutzfeldt-Jakob
disease. J fluid
Neurol
Psychiatry
2001;
Dement Sect
1993;6:119–126.
tigations in cerebrospinal
of Neurosurg
patients with
dementia
with
71:33–39.
279.1252–1254.
Jimenez-Jimenez FJ, Molina JA, Hernanz A, et al. CerebrospiLewy bodies and Alzheimer’s disease. J Neural Transm 2005;
278. Tohgi
H, Abe
S, patients
Kikuchiwith
T. The
urate anddisease.
xan260. Botella-Lopez
nal fluid
levelsT,ofTakahashi
thiamine in
Parkinson’s
112:933–948. A, Burgaya F, Gavin R, et al. Reelin expression
thine
concentrations
in the cerebrospinal fluid in patients with
patternsM,areBorggreve
altered inF, Alzheimer’s
disease.
Neurosci
Lett 1999;271:33–36.
262.and
De glycosylation
Deyn PP, Hiramatsu
et al. Superoxide
disdementia
Binswanger
Alzheimer
deProc
Natlactivity
Acad Sci
2006;103:5573–5578.
280.vascular
Buhmann
C, Arlt of
S, the
Kontush
A, et al.type,
Plasma
and CSFtype
markers
mutase
in USA
cerebrospinal
fluid of patients with dementia
mentia,
and Parkinson’s
Transmdisease
Park Dis
261. Mollenhauer
B, Bibl
M, Trenkwalder
C, etAlzheimer
al. Follow-up
of oxidative
stress are disease.
increasedJ inNeural
Parkinson’s
and
and some other
neurological
disorders.
DisinvesAssoc
Dement
Sectby1993;6:119–126.
tigations
in cerebrospinal fluid of patients with dementia with
influenced
antiparkinsonian medication. Neurobiol Dis 2004;
Disord 1998;12:26–32.
279. Jimenez-Jimenez
FJ, Molina JA, Hernanz A, et al. Cerebrospibodies
and Alzheimer’s
disease.Y,J etNeural
Transmof2005;
15:160–170.
263.Lewy
Aoyama
K, Matsubara
K, Fujikawa
al. Nitration
manfluid levelsB,ofTrenkwalder
thiamine in patients
with
disease.
112:933–948.
281.nal
Mollenhauer
C, Cullen
V, Parkinson’s
et al. A platform
for
ganese superoxide dismutase in cerebrospinal fluids is a marker
Neurosci
Lett 1999;271:33–36.
262. De
PP, Hiramatsu M, oxidative
Borggrevestress
F, et inal.neurodegenerative
Superoxide disthe quantification
of alpha-synuclein in cerebrospinal fluid: eviforDeyn
peroxynitrite-mediated
280. Buhmann
S, Kontush
A, et
Plasma and CSF Neurodemarkers
mutase
activity
in cerebrospinal
fluid of patients with dementia
dence forC,a Arlt
potential
biomarker
foral.synucleinopathies.
diseases.
Ann Neurol
2000;47:524–527.
ofgenerative
oxidativeDiseases
stress are
increased
Parkinson’s
someB,other
neurological
Alzheimer
Dis forms
Associn
2007;4
(Suppl in
1):1–350
(P463).disease and
264.and
Borroni
Gardoni
F, Parnettidisorders.
L, et al. Pattern
of Tau
antiparkinsonian
Dis 2004;
Disord
1998;12:26–32.
282.influenced
Mogi M, by
Harada
M, Kojimamedication.
K, et al. Neurobiol
Beta 2-microglobulin
CSF is
altered in progressive supranuclear palsy. Neurobiol
15:160–170.
263. Aoyama
K, Matsubara K, Fujikawa Y, et al. Nitration of mandecrease in cerebrospinal fluid from parkinsonian patients. NeuAging 2007;30:34–40.
281. Mollenhauer
B, Trenkwalder C, Cullen V, et al. A platform for
superoxide
cerebrospinal
fluidsJellinger
is a marker
rosci Lett 1989;104:241–246.
265.ganese
Lins H,
Wichart dismutase
I, Bancherin C,
Wallesch CW,
KA,
quantification
of alpha-synuclein
fluid:
evifor
peroxynitrite-mediated
oxidative
stress inbeta
neurodegenerative
Rosler
N. Immunoreactivities
of amyloid
peptide((1-42))
283.the
Verbeek
MM, Abdo
WF, De Jong inD,cerebrospinal
Horstink MW,
Kremer
dence
for a potential
biomarker for
Neurodediseases.
BP, Bloem
BR. Cerebrospinal
fluidsynucleinopathies.
Abeta42 levels in
multiple
and totalAnn
tauNeurol
protein2000;47:524–527.
in lumbar cerebrospinal fluid of patients
generative
DiseasesMov
2007;4
(Suppl2004;19:238–240;
1):1–350 (P463). author reply
264. Borroni
B, Gardoni
F, Parnetti
L, et al. Pattern
of Tau
forms
in
system atrophy.
Disord
with normal
pressure
hydrocephalus.
J Neural
Transm
2004;
282. Mogi
M, Harada M, Kojima K, et al. Beta 2-microglobulin
CSF
is altered in progressive supranuclear palsy. Neurobiol
240–231.
111:273–280.
cerebrospinal
from parkinsonian
patients.
Neu2007;30:34–40.
266.Aging
Bibl M,
Mollenhauer B, Esselmann H, et al. CSF diagnosis of
284.decrease
HanssoninO,
Zetterberg fluid
H, Buchhave
P, Londos
E, Blennow
rosci
Lett 1989;104:241–246.
265. Lins
H, Wichart
I, Bancher
C, Wallesch
CW,bodies.
Jellinger
KA,
Alzheimer’s
disease
and dementia
with Lewy
J Neural
K, Minthon
L. Association between CSF biomarkers and inRosler
Immunoreactivities of amyloid beta peptide((1-42))
283. Verbeek
Abdo WF,
De Jong
D, Horstink
MW, cognitive
Kremer
cipient MM,
Alzheimer’s
disease
in patients
with mild
TransmN.2006;113:1771–1778.
BP,
Bloem BR.a Cerebrospinal
fluidLancet
Abeta42Neurol
levels 2006;5:228–
in multiple
total L,
tauLanari
proteinA,inAmici
lumbar
cerebrospinal
fluid of patients
impairment:
follow-up study.
267.and
Parnetti
S, Gallai
V, Vanmechelen
E, Hulsystem
with
hydrocephalus.
Neural Transm
2004;
234. atrophy. Mov Disord 2004;19:238–240; author reply
staertnormal
F. CSFpressure
phosphorylated
tau is aJ possible
marker for
dis111:273–280.
criminating Alzheimer’s disease from dementia with Lewy
285.240–231.
Mollenhauer B, Steinacker P, Bahn E, et al. Serum Heart-Type
266. Bibl
M, Mollenhauer
Esselmann H,Study
et al.Group.
CSF diagnosis
284. Hansson
O, ZetterbergProtein
H, Buchhave
P, Londos E,Fluid
Blennow
Fatty Acid-Binding
and Cerebrospinal
Tau:
bodies.
Phospho-TauB,International
Neurol of
Sci
Alzheimer’s
disease and dementia with Lewy bodies. J Neural
K,Marker
Minthon
L. Association
between
CSF
biomarkers
and inCandidates
for Dementia
with
Lewy
Bodies. Neurode2001;22:77–78.
cipient
Alzheimer’s
disease in patients with mild cognitive
2006;113:1771–1778.
generative
Diseases 2007;4:366–375.
268.Transm
Tschampa
HJ, Schulz-Schaeffer W, Wiltfang J, et al. Decreased
follow-up particle-based
study. Lancet flow
Neurol
2006;5:228–
267. Parnetti
L, Lanari
A, Amici
S, Gallai
Vanmechelen
E, HulCSF amyloid
beta42
and normal
tauV,levels
in dementia
with
286.impairment:
Vignali DA. aMultiplexed
cytometric
assays.
234.
staert
CSF phosphorylated
tau is a possible marker for disJ Immunol Methods 2000;243:243–255.
LewyF.bodies.
Neurology 2001;56:576.
Lewy
285.
B, Steinacker
P, Bahn
E, et al. Serum
Heart-TypeL.
269.criminating
MollenhauerAlzheimer’s
B, Bibl M, disease
Wiltfangfrom
J, etdementia
al. Total with
tau protein,
287.Mollenhauer
Constantinescu
R, Zetterberg
H, Holmberg
B, Rosengren
Fatty
Protein
Cerebrospinalfluid:
Fluid
bodies.
Phospho-Tau
International
Study
Group. Neurol Sci
phosphorylated
tau (181p)
protein,
beta-amyloid(1-42),
and
LevelsAcid-Binding
of brain related
proteinsand
in cerebrospinal
An Tau:
aid in
Marker
Candidates
for Dementia
with Lewydisorders.
Bodies. ParkinsonNeurode2001;22:77–78.
beta-amyloid(1-40) in cerebrospinal fluid of patients with dethe differential
diagnosis
of parkinsonian
generative
2007;4:366–375.
268. Tschampa
HJ, Lewy
Schulz-Schaeffer
Wiltfang
et al.
Decreased
mentia with
bodies. ClinW,Chem
Lab J,Med
2006;44:192–
ism Relat Diseases
Disord 2008;15:205–212.
CSF
286.
DA.H,
Multiplexed
flow
assays.
195.amyloid beta42 and normal tau levels in dementia with
288.Vignali
Zetterberg
Ruetschi U,particle-based
Portelius E, et
al. cytometric
Clinical proteomics
J in
Immunol
Methods 2000;243:243–255.
bodies. Neurology
270.Lewy
Engelborghs
S, Maertens2001;56:576.
K, Vloeberghs E, et al. Neuropsychoneurodegenerative
disorders. Acta Neurol Scand 2008;118:1–
269. Mollenhauer
B, Bibl M,correlates
Wiltfang ofJ, CSF
et al.biomarkers
Total tauinprotein,
287. Constantinescu
R, Zetterberg H, Holmberg B, Rosengren L.
logical and behavioural
demen11.
phosphorylated
tau International
(181p) protein,
beta-amyloid(1-42), and
of brain
related proteins
in cerebrospinal
fluid:Competence
An aid in
tia. Neurochemistry
2006;48:286–295.
289.Levels
Lewczuk
P, Kornhuber
J, Wiltfang
J. The German
1426
B. disorders.
MOLLENHAUER
in cerebrospinal
fluid degeneration
of patients with
the
parkinsonian
271.beta-amyloid(1-40)
Urakami K, Nakashima
K. Corticobasal
and deproNetdifferential
Dementias:diagnosis
Standardofoperating
procedures
for Parkinsonthe neuro- AND C. TRENKWALD
mentia
with
Lewy bodies.
Clin Chem Labmarker.
Med 2006;44:192–
ism
Relat Disord
2008;15:205–212.
gressive
supranuclear
palsy--biochemical
Rinsho Shinchemical
dementia
diagnostics. J Neural Transm 2006;113:
195.
288. Zetterberg
H, Ruetschi U, Portelius E, et al. Clinical proteomics
keigaku 2002;42:1162–1164.
1075–1080.
270. Engelborghs S, Maertens K, Vloeberghs E, et al. Neuropsychoneurodegenerative
disorders.
Neurol Scand
2008;118:1–
290.inMollenhauer
B, Krastins
B, Acta
Trenkwalder
C, Schlossmacher
294. Mehta PD, Pirtt
logical and behavioural correlates of CSF biomarkers in demen11.
MG, Sarracino DA. Proteome analysis of cerebrospinal fluid
Amyloid beta pr
tia. Neurochemistry International 2006;48:286–295.
289. Lewczuk
Kornhuber J,AWiltfang
Themarker
German
Competencein
by mass P,spectrometry:
platformJ.for
development
spinal fluid and
DIAGNOSTICS IN MOVEMENT
DISORDERS
271. Urakami
K, Nakashima K. Corticobasal degeneration and1425
proNet
Dementias: Standard
operating
procedures
for (Suppl
the neurosynucleinopathies.
Movement
Disorders
2006;21
15):
Neurosci Lett 20
Movement
Vol. 24, No.
10, 2009
gressive supranuclear palsy--biochemical marker. Rinsho Shinchemical
J Disorders,
Neural Transm
2006;113:
P780. dementia diagnostics.
295. Huang RP. Cyto
keigaku 2002;42:1162–1164.
291.1075–1080.
Lewczuk P, Esselmann H, Groemer TW, et al. Amyloid beta
264:215–231.
A, et al. Cerebrospi272. Mitani K, Furiya Y, Uchihara T, et al. Increased CSF tau
peptides in cerebrospinal fluid as profiled with surface enhanced
296. Ray S, Britschgi
inson’s disease. Acta
protein in corticobasal degeneration. J Neurol 1998;245:
laser desorption/ionization time-of-flight mass spectrometry:
tion of clinical A
44–46.
evidence of novel biomarkers in Alzheimer’s disease. Biol Psyproteins. Nat Me
Bassetti CL. Normal
273. Hampel H, Buerger K, Zinkowski R, et al. Measurement of
chiatry 2004;55:524–530.
297. Hennecke G, Sch
Movement
Vol.and
24, No.
10, 2009
ementia with Lewy
phosphorylated tau epitopes in the differential diagnosis of Alz292. Peskind ER, Riekse R, Quinn
JF, Disorders,
et al. Safety
acceptability
developing tool fo
eepiness. Eur Neurol
heimer disease: a comparative cerebrospinal fluid study. Arch
of the research lumbar puncture. Alzheimer Dis Assoc Disord
298. Tabchy A, Hous
1426
B. MOLLENHAUER AND C. TRENKWALDER
Gen Psychiatry 2004;61:95–102.
2005;19:220–225.
report card from
A, et al. Cerebrospi274. Vanderstichele H, De Vreese K, Blennow K, et al. Analytical
293. Irizarry MC. Biomarkers of Alzheimer disease in plasma. Neuprogression in H
ystem atrophy. Mov
performance and clinical utility of the INNOTEST PHOSPHOroRx 2004;1:226–234.
14:649–650.
assayB,forKrastins
discrimination
between Alzheimer’s
disease
290.TAU181P
Mollenhauer
B, Trenkwalder
C, Schlossmacher
294. Mehta PD, Pirttila T, Patrick BA, Barshatzky M, Mehta SP.
and
dementia
withDA.
Lewy
bodies. Clin
Chem
Med 2006;44:
ele M, De Deyn P,
MG,
Sarracino
Proteome
analysis
of Lab
cerebrospinal
fluid
Amyloid beta protein 1-40 and 1-42 levels in matched cerebro1472–1480.
is of 201 possible
by mass spectrometry: A platform for marker development in
spinal fluid and plasma from patients with Alzheimer disease.
urol 2004;251:298–
275. Wada-Isoe
K, Kitayama
M, Nakaso
K, Nakashima
Diagnossynucleinopathies.
Movement
Disorders
2006;21K.(Suppl
15):
Neurosci Lett 2001;304:102–106.
ticP780.
markers for diagnosing dementia with Lewy bodies: CSF
295. Huang RP. Cytokine protein arrays. Methods Mol Biol 2004;
MIBG P,
cardiac
scintigraphy
study. TW,
J Neurol
2007;260:
sis of EEG and CSF
291.and
Lewczuk
Esselmann
H, Groemer
et al.Sci
Amyloid
beta
264:215–231.
33–37.
of Creutzfeldt-Jakob
peptides in cerebrospinal fluid as profiled with surface enhanced
296. Ray S, Britschgi M, Herbert C, et al. Classification and prediclaser M,
desorption/ionization
time-of-flight
mass H,spectrometry:
tion of clinical Alzheimer’s diagnosis based on plasma signaling
276. Mogi
Harada M, Riederer
P, Narabayashi
Fujita K,
evidenceT.ofTumor
novel necrosis
biomarkers
in Alzheimer’s
disease. increases
Biol Psyproteins. Nat Med 2007;13:1359–1362.
Nagatsu
factor-alpha
(TNF-alpha)
ochstrasser DF. CSF
chiatry
2004;55:524–530.
297. Hennecke G, Scherzer CR. RNA biomarkers of Parkinson’s disease:
both
in the
brain and in the cerebrospinal fluid from parkinsoed patients with de292.nian
Peskind
ER, Neurosci
Riekse R,Lett
Quinn
JF, et al. Safety and acceptability
developing tool for new therapies. Biomarkers Med 2008;2:41–53.
patients.
1994;165:208–210.
of the research
lumbar
puncture.
Alzheimer
DisElevated
Assoc Disord
298. Tabchy A, Housman D. Huntington’s disease: A transcriptional
277. Vermes
I, Steur EN,
Jirikowski
GF,
Haanen C.
conPatients with Alzhei2005;19:220–225.
report card from the peripheral blood: can it measure disease
centration
of cerebrospinal fluid tissue transglutaminase in Parbodies mistaken for
293.kinson’s
Irizarry MC.
Biomarkers
Alzheimer Mov
diseaseDisord
in plasma.
Neuprogression in Huntington’s disease? Eur J Hum Genet 2006;
disease
indicatingof apoptosis.
2004;19:
urg Psychiatry 2001;
roRx 2004;1:226–234.
14:649–650.
1252–1254.
278. Tohgi H, Abe T, Takahashi S, Kikuchi T. The urate and xanal. Reelin expression
thine concentrations in the cerebrospinal fluid in patients with
Alzheimer’s disease.
vascular dementia of the Binswanger type, Alzheimer type de578.
mentia, and Parkinson’s disease. J Neural Transm Park Dis
al. Follow-up invesDement Sect 1993;6:119–126.
with dementia with
279. Jimenez-Jimenez FJ, Molina JA, Hernanz A, et al. CerebrospiNeural Transm 2005;16
nal fluid levels of thiamine in patients with Parkinson’s disease.
Neurosci Lett 1999;271:33–36.
t al. Superoxide dis280. Buhmann C, Arlt S, Kontush A, et al. Plasma and CSF markers
tients with dementia
of oxidative stress are increased in Parkinson’s disease and
lzheimer Dis Assoc
influenced by antiparkinsonian medication. Neurobiol Dis 2004;
15:160–170.
al. Nitration of man-
傍腫瘍性運動障害
Paraneoplastic Movement Disorders
*
Robin Grant, MB, ChB, MD, FRCP and Francesc Graus, MD
*
Edinburgh Centre for Neuro-Oncology, Western General Hospital, Edinburgh, United Kingdom
傍腫瘍性運動障害は癌の転移によるのではなく,自己免
する臨床的な特徴としては,発症が急であること,重症
疫性機序で起こる,稀に見られる合併症である。傍腫
であること,進行が早いこと,治療に抵抗すること,そ
瘍性運動障害でよくみられるのは,小脳症候群,オプソ
して傍腫瘍性以外の病因では考えられないほど広汎な
クローヌス・ミオクローヌス症候群,大脳基底核障害,
神経学的症状を呈することにある。典型的な症状を示す
stiff person 症候群,神経性筋強直症である。通常,こ
患者や,傍腫瘍性抗体を有して疑わしい症状を呈する
れらの症候群は癌と診断される前に発現し,単一あるい
患者では,癌を検索すべきである。最初の検索で腫瘍
は複数の血清抗体を伴うことが多い。原因となる多くの
がみつからなかった場合には,時間を置いて再度スク
抗 体 が 認 識 さ れ つ つ あ る(Hu,Yo,Ri,CV2,
リーニングするのが望ましい。本症に最も良く伴う癌は,
amphiphysin,Ma,Ta,Tr,NMDA,mGluR1,PCA2,
肺小細胞癌,乳癌,婦人科領域の癌,精巣癌,リンパ腫,
ANNA-3,VGCCA)
。抗体が存在する場合は,基礎疾患
胸腺腫である。早期発見と早期治療によって神経学的
として癌がある可能性が高く,抗体の種類はある特定の
改善が得られる場合があり,癌の予後も改善する可能
腫瘍と密接に結びついている。傍腫瘍性の病因を示唆
性がある。予後は,
腫瘍の種類と治療反応性に依存する。
Movement Disorders Vol. 24, No. 12, 2009, pp. 1715–1724
Key Word 傍腫瘍性,小脳性,オプソクローヌス,ミオクローヌス,舞踏病,パーキンソン,stiff person
傍腫瘍性神経症候群は癌の転移によらない,自己免疫
性の合併症で,発症率は全癌患者の 1%未満と稀である。
中枢神経系(central nervous system; CNS)自己抗体が同
定された患者の一部では,運動障害が認められる。
る抗神経抗体は,細胞内に標的があり,おそらく病因で
はないと考えられる。
アポトーシスを起こした腫瘍細胞から放出される腫瘍
抗原は末梢リンパ節を灌流する T リンパ球に提示され,
CNS 傍腫瘍性症候群では,神経抗原に対する抗体が血
これが複雑な免疫応答のきっかけとなり,その結果 CNS
清および脳脊髄液(cerebrospinal fluid; CSF)中に高レベ
内で類似抗原を発現しているニューロンが攻撃されると
ルに検出されることが多い(ただし常に認められるわけ
考えられる 2。
このような機序の例外として,
稀ではあるが,
ではない)
。どの抗体が検出されたかにより,基礎疾患と
P/Q 型電位依存性カルシウムチャネル抗体(基礎疾患が
しての癌がどのような癌であるかを予測でき,またどの
肺小細胞癌の場合)
,あるいは mGluR1 グルタミン酸受容
部位の癌かを推定するのに大きな助けとなる場合がある。
体抗体(基礎疾患がホジキン病の場合)が関与する純粋
しかしどのような神経症候群を呈するかは特異的でない
型小脳変性症例がある 3,4。また,基礎疾患に卵巣奇形腫
ことが多い 1。癌神経抗原(onconeural antigen)は,CNS
がある場合には,N- メチル -D- アスパラギン酸受容体
または末梢神経系ニューロンに発現している抗原と同一
(N-methyl-D-aspartate receptor; NMDAR)抗体が脳炎を引
ないしは関連性があるが,正確な免疫学的・病理学的発
き起こす直接の病因となることがあり,これは治療に反
生機序は未だ不明である。CNS 傍腫瘍性症候群に関連す
応する可能性がある 5。
17
傍腫瘍性運動障害
傍腫瘍性神経症候群の診断に関
するエビデンス
も明らかでない場合には,PET スキャンが腫瘍の原発部
約 70%の症例では,癌と診断される前に神経学的所見
ド療法,免疫グロブリン静注(intravenous injection of
位の特定に役立つであろう 7。早期に傍腫瘍性と診断され
た場合には,すべての患者に対症療法〔例えばステロイ
immunoglobulin; ivIg)
,血漿交換〕を行うべきである 8。
が認められている。傍腫瘍性症候群の診断基準は国際的
に受け入れられ,
合意に達している(Figure 1 参照)6。
「典
傍腫瘍性小脳変性症
型的」および「非典型的」な症状も定義されている。典
型的な症候群は,脳脊髄炎,辺縁系脳炎,亜急性小脳変
臨床像
性症,オプソクローヌス・ミオクローヌス,亜急性感覚
性末梢神経障害(subacute sensory neuronopathy)と慢性
傍腫瘍性小脳変性症は最も頻度の高い CNS 傍腫瘍性
消化管偽閉塞症,Lambert-Eaton 筋無力症候群(Lambert-
症候群の 1 つである。患者は亜急性小脳性運動失調症を
Eaton Myasthenic Syndrome; LEMS)
,皮膚筋炎である。傍
呈し,数週間ないし数ヵ月かけて進行して最終的に 6 ヵ
腫瘍性神経症候群に典型的な,あるいは疑わしい症状が
月以内に安定化するが,患者には重度の身体能力障害が
認められた場合には,癌の検索を急ぐべきである(Figure
残る。小脳性運動失調症の 40%は非対称性で,しばしば
1)
。癌がみつかった場合には,血清抗体の同定結果の如
構音障害,上肢の協調障害,眼振を伴う。通常,眼振は
何にかかわらず,傍腫瘍性神経症候群であると確信して
下向眼振であるが,滑動性追従眼球運動の消失やオプソ
よい。非典型的な症候群であっても,腫瘍が特定されて
クローヌスがみられることもある 9,10。
抗体が存在すれば,
その診断は「確実(definite)
」である。
小脳性運動失調症の症状には次の 4 パターンがある。
傍腫瘍性神経症候群が疑われるが,癌がみつからない場
a. 小脳失調以外に,診察で比較的びまん性の脳脊髄炎
合には,臨床的ジレンマが生じる。典型的な症候群を伴
の徴候(例えば,痙攣,気分の変化,人格変化,記
う患者の血清で「性質が十分に明らかにされている(well
憶障害,眼振,舞踏病)を伴うか,辺縁系脳炎または
characterised)
」抗体が同定されれば,病因が傍腫瘍性で
感覚性ニューロパチーの併存を認める。血清および
あることの裏付けとなる(Table 1)
。
CSF 中に抗 Hu 抗体が認められる場合が多く,通常,
腫瘍のスクリーニング検査として胸部・腹部 CT スキャ
基礎疾患として肺癌が存在する 9-11。
ンを行うが,必要に応じて骨盤超音波検査とマンモグラ
b. 女性に発症する純粋型小脳症候群では一般に抗 Yo 抗
フィーも行う。スクリーニング結果が陰性で,他の診断
体がみられ,基礎疾患として乳癌あるいは婦人科領
神経症候群
典型的
腫瘍あり
癌神経抗体
の有無
確実
非典型的
腫瘍なし
癌神経抗体
なし
腫瘍なし
癌神経抗体
あり
癌の危険性高
性質が十分に
明らかにされている
癌神経抗体あり
可能性あり
確実
腫瘍あり
癌神経抗体
なし
性質がある程度
明らかにされている
癌神経抗体あり
可能性あり
癌治療後の改善
もしくは
癌神経抗体あり
可能性あり
確実
Figure 1 傍腫瘍性神経症候群の診断根拠のフローチャート(Graus F, et al: J Neurol Neurosurg Psychiat 2004, 75: 1135-1140)
18
41.5
128
Ma2/Ta
Amphiphysin
AchR
Other
Membrane
NMDAR
Synaptic
Membrane
Nuclear
Cytoplasmic
Cytoplasmic
Synaptic
Nuclear
Cytoplasmic
Cyotplasmic
Nuclear
Membrane
65, 67
Site
Nuclear
VGCCA
GAD 65
VGKCA
Various
290
66
CV2/CRMP-5
ZIC4 and ANNA-3
PCA-2
34, 52, 62
PCA-1 (anti-Yo)
unknown
55, 80
ANNA-2 (anti-Ri)
Tr
34–40
Antibody
ANNA-1 (anti-Hu)
Staining pattern
Postsynaptic Neuromuscular
junction
Neuropile
None
Cerebellar Purkinje cells, dots
in molecular layer
CNS nuclei
Cerebellar Purkinje cells/other
neurones
Central presynaptic terminals
Neuropile
Central presynaptic
terminals
CNS nuclei
Oligodendrocyte,
neurons
Cerebellar Purkinje
cell and axons
CNS nuclei
CNS nuclei 1 peripheral
neurones
Myasthenia
Oro-facial dyskinesias,c
Muscle rigidity, dystonia
PCD
SPS, PCD, extrapyramidal
Neuromyotonia
PCD
PCD
PCD
SPS, spinal myoclonusb
PSP, Parkinsonism
PCD, chorea
PCD, chorea
OMS, PCD
Thymoma, Renal
SCLC, Thymoma
None (90%)
SCLC
None (50%)
Ovary/testicular
Teratoma (50%)
None (50%)
Thymoma
Associated cancer
Lung (86%)
Other (12%)
None (2%)
Lung (46%)
Breast (32%)
Other (13%)
None (<9%)
Ovary/breast (90%)
Other (8%)
None (2%)
Lung (60%)
Thymoma (13%)
Extrathoracic (23%)
None (4%)
Testis (53%)
Lung (21%)
Other (14%)
None (12%)
Breast (mainly)
Lung, ovary
None (20%)
Hodgkin
None (2%)
Lung (90%)
Lung (90%)
Movement disorder
PCD, OMS,a epilepsy
partialis continuans,b chorea
Nil
Encephalitis
LEMS
PEM, BSE
PLE
PEM, PSN
Nil
Nil
PEM, PSN
PLE
PEM, PSN
Nil
BSE
PEM, PLE, PSN
Associated
paraneoplastic
syndromes
例外的な患者。オプソクローヌス・ミオクローヌス運動失調症(opsoclonus
myoclonus
OMA)および肺小細胞癌(small
Occasional patients. Most patients with opsoclonus myoclonus ataxia (OMA) and
small cellataxia;
lung cancer
(SCLC) are seronegative. cell lung cancer; SCLC)患者の大部分は血清抗体
b
Only a few case reports described.
陰性である。
c
b Dyskinesias are part of a more complex encephalopathic syndrome.
わずか数例の症例報告のみ。
ANNA,
antinuclear neuronal antibody; CNS, central nervous system; PCD, paraneoplastic cerebellar degeneration; OMS, opsoclonus myoclonus syndrome; PEM, paraneoplastic encephac
ジスキネジアは,より複雑な脳症症候群の一部である。
lomyelitis;
PLE, paraneoplastic limbic encephalitis; PSN, paraneoplastic sensory neuropathy; Tr, anti-Purkinje cell antibody-Tr; BSE, brain stem encephalitis; PCA, anti-Purkinje cell antibody;
CV2,
crossveinless-2; CRMP5, collapsing
response mediator
protein-5; PSP, progressive
supranuclear palsy; SPS, stiff person syndrome; ZIC4,
zinc finger protein; GAD,
glutamic
ANNA
=神経細胞抗核抗体,CNS
=中枢神経系,PCD
=傍腫瘍性小脳変性症,OMS
=オプソクローヌス・ミオクローヌス症候群,PEM
=傍腫瘍性脳脊髄炎,PLE
=傍腫瘍性
acid decarboxylase; VGKC, voltage-gated potassium channel; SCLC, small cell lung carcinoma; VGCC, voltage-gated calcium channel; LEMS, Lambert eaton myasthenic syndrome;
辺縁系脳炎,PSN
=傍腫瘍性感覚性ニューロパチー,Tr
-Tr,BSE =脳幹脳炎,PCA
= crossveinless-2,CRMP5
=
NMDA
GluR, N-methyl-D-aspartate
type glutamate receptor;=抗プルキンエ細胞抗体
NMDAGluR1, N-Methyl-D-aspartate
glutamate receptor =抗プルキンエ細胞抗体,CV2
type 1; AchR, acetylcholine receptor;
Ma/Ta, a family of proteins
collapsing in
response
protein-5,PSP =進行性核上性麻痺,SPS = stiff person 症候群,ZIC4 =ジンクフィンガー蛋白質,GAD =グルタミン酸脱炭酸酵素,VGKC =電位依存
expressed
neuronsmediator
and testes.
性カリウムチャネル,SCLC =肺小細胞癌,VGCC =電位依存性カルシウムチャネル,LEMS = Lambert-Eaton 筋無力症候群,NMDA GluR = N- メチル -D- アスパラギン酸型グル
タミン酸受容体,NMDA GluR1 = N- メチル -D- アスパラギン酸型グルタミン酸受容体 1 型,AchR =アセチルコリン受容体,Ma/Ta =ニューロンと精巣に発現する蛋白質ファミリー
aa
Associated with PNS
and autoimmune
syndromes
Partially characterized
antibodies
Well characterised
Molecular
Wt (kD)
TABLE 1. Paraneoplastic
antibodies and their clinical accompaniments
Table 1 傍腫瘍性抗体とその臨床的関連性
R. Grant and F. Graus
PARANEOPLASTIC DISORDER
1717
Movement Disorders, Vol. 24, No. 12, 2009
19
傍腫瘍性運動障害
域の癌を伴う。患者の 90%は車椅子生活となる。
生じることがある。多系統萎縮症や遺伝性成人発症型運
c. 純粋型小脳症候群(症例の 93%)はホジキンリンパ
動失調症は,数ヵ月ないし数年という,はるかに緩徐な
腫が確認された患者にみられ,男性のほうが女性より
経過をたどるのが一般的である。
も多い(3:1)
。小脳症候群が腫瘍診断に先行するの
MRI は通常早期には正常で,症候群が進展する後期に
はわずか 30%である 。血清検査で抗体が認められ
なると小脳萎縮がみられる。症例の 80%で CSF に異常が
ない場合もあるが,CSF 中に抗 Tr 抗体が検出される
みられ,約 1/3 に蛋白質の軽度増加やオリゴクローナル
こともある 12。ホジキンリンパ腫では,稀に腫瘍が治
バンドが認められる 10,14。胸部,腹部,骨盤部 CT による
癒して何年も経過したのちに mGluR1 に対する自己抗
予備的検索で腫瘍がみつからなかった場合には,傍腫瘍
体(autoantibody against mGluR1; mGluR1-Ab)が認め
性抗体の同定が診断に役立つ。血清抗体が陽性であれば,
られる症例もある 。
運動失調症の病因が傍腫瘍性であることが裏付けられ,
10
9
d. LEMS を随伴する小脳症候群(あるいは,LEMS の臨
床所見がなく,電位依存性カルシウムチャネル抗体
より詳細な評価あるいは経過観察すべき,原発の可能性
が高い腫瘍を指摘できる。
を伴う小脳症候群)
。通常これらの症例では,基礎疾
管理および予後
患として肺小細胞癌がみられる。
通常,患者は数週間ないし数ヵ月間かけて神経学的に悪
病因
化し,重度の身体能力障害となり安定化する。治療による
病理学的所見は小脳プルキンエ細胞のびまん性の消失
神経学的回復の確率ならびに全体的な予後は,抗体と癌の
で,周囲の星状グリア細胞の反応性増殖と血管周囲への
種類に左右される。傍腫瘍性小脳性運動失調症を全体と
リンパ球浸潤(cuffing)を伴う。脳脊髄炎の一部として
して見ると,患者の 14%が改善し,32%が症状が安定し
本症候群が認められる場合には,さらに広汎な CNS の炎
てしまい,54%が増悪する。改善した患者は,いずれも基
症性変化が報告されている 。傍腫瘍性小脳変性症には
礎疾患としての癌に対する抗腫瘍療法によりもとの癌が完
数多くの様々な抗体が関係している(Table 1)
。傍
全寛解に到達した。抗腫瘍療法(免疫抑制療法を併用し
腫瘍性小脳性運動失調症患者 137 例を対象とした研究で
てもしなくても)を受けた患者の生存期間は有意に延長し
は,38%が抗 Yo 抗体を有し,36%が抗 Hu 抗体,14%が
た〔ハザード比(hazard ratio; HR)0.3,95%信頼区間
抗 Tr 抗体,12%が抗 Ri 抗体,4%が抗 mGluR1 抗体を有
(confidence interval; CI)0.1 ~ 0.6,p = 0.004〕9。抗 Yo 抗
13
9,14-16
していた。肺癌を合併した小脳性運動失調症患者では,
体あるいは抗Hu抗体関連の小脳性運動失調症に対しては,
39 例中 16 例(41%)で P/Q 型電位依存性カルシウムチャ
抗腫瘍療法や免疫抑制療法は一般に有効ではない 9,15,16,22。
ネル抗体が上昇していたが,この 16 例のうち LEMS の
ただし,稀に奏効例も報告されている 23。抗 Hu 抗体関連
臨床所見を示したのは 7 例のみであった 3。抗 Hu 抗体は
小脳性運動失調症を呈する肺小細胞癌における生存期間
39 例中 9 例(23%)で認められたが,抗 CV2/CRMP5 抗
の中央値は約 7 ヵ月である。抗 Ri 抗体関連小脳性運動失
体,あるいは ANNA-3,PCA-2,amphiphysin などの抗体
調症の症例では,50%が治療により神経学的に改善し,生
陽性者は少なかった
存期間の中央値は 69 ヵ月であった 9。抗 Tr 症候群では,
。同一患者にこれらの抗体のい
3,17-21
くつかが存在する場合もしばしばみられる。
15%で小脳症状の寛解が報告されているが,寛解するのは
通常,比較的若い患者である。小脳失調の症候群と抗体
診断
成人発症の亜急性小脳性運動失調症の鑑別診断は多岐
が存在しても,リンパ腫がみつからないか,腫瘍が良好に
治療できた場合には,小脳症候は消失しうる 12。
にわたる。クロイツフェルト - ヤコブ病や一部の感染性
オプソクローヌス・ミオクロー
ヌス症候群
疾患が類似の病態を示す場合がある。アルコールに関連
した小脳性運動失調症や,Wernicke Korsakoff 症候群,
ビタミン B12 欠乏症,葉酸欠乏症などの欠乏症は亜急性
の運動失調の経過をとりうる。甲状腺機能低下症や橋本
甲状腺炎などの内分泌疾患も,亜急性の小脳失調徴候を
20
臨床像
オプソクローヌス・ミオクローヌス症候群(Opsoclonus-
R. Grant and F. Graus
Myoclonus Syndrome; OMS)は,不随意かつ非律動性で,
て出現する場合がある。結合組織病,炎症性疾患,連鎖
全方向に振幅の大きな共同性サッケードが認められる無
球菌感染後疾患は傍腫瘍性 OMS に類似した症状を呈し,
秩序な眼球運動と,ミオクローヌスを伴う稀な症候群で
いずれの疾患でも精神医学的所見を随伴する可能性があ
ある。ミオクローヌスは持続時間が短く,自発的で,通
る。リチウム,アミトリプチリン過量投与,シクロスポリ
常刺激感受性でもある筋収縮(jerk)で,四肢や口蓋・顔
ン毒性,タリウムなどの薬剤によるものを含め,中毒性な
面・喉頭あるいは呼吸筋に認められる。通常,本症候群
いし代謝性脳症も OMS を引き起こすことがある。少数例
は亜急性に発症し,速やかに進行する 24。
ではあるが,糖尿病患者の高浸透圧性昏睡でも OMS をき
OMS の原因は発症時年齢により異なる。小児では,
たすとの報告がある。他の原因が除外されれば,傍腫瘍
OMS は 6 ヵ月~ 3 歳 の 女 児 の 発 症 頻 度 が 最も高 い。
性 OMS の可能性は非常に高くなる。小児では,全例に対
OMS の発症前に明らかな感染エピソードがなければ,傍
し基礎疾患としての神経堤腫瘍の検索が必要である。抗
腫瘍性 OMS を疑うべきである。50%を超える症例で神
体検査の結果は陰性であることが多い。成人では,画像
経芽細胞腫が確認されているが,その症状は感染後 OMS
検査によって肺小細胞癌,乳癌,または稀ではあるがそ
や特発性 OMS と区別できない。自然に寛解する場合もあ
の他の癌(腎癌,胃癌,甲状腺癌,膵癌,卵巣癌,リン
るが,
再発も多い
。70 ~ 80%の小児に神経学的後遺症,
パ腫,胸腺腫,成人神経芽細胞腫,肉腫)が検出される
認知あるいは行動関連の後遺症が長期にわたって残る。
場合がある 28-36。ただし,成人症例では癌の初回検索結果
成人では,ほとんどの症例で OMS が腫瘍の診断に先行
はほとんどが陰性である。患者が 50 歳を超えており,認
する。器質的疾患または感染性の原因を除外すると,
知もしくは行動所見を呈する場合には,傍腫瘍性抗体の
OMS は特発性か傍腫瘍性のいずれかである 。年齢中央
血清検査が特に有用となる。さらに,広範な傍腫瘍性脳
値は,ある比較研究では傍腫瘍性群が 66 歳,特発性群
脊髄炎の一部としてオプソクローヌス・ミオクローヌス運
が 40 歳で,傍腫瘍性群には 50 歳未満の患者はいなかっ
動失調症(opsoclonus myoclonus ataxia; OMA)が存在する
た 。傍腫瘍性群ではほぼ例外なく脳症がみられ,一部
場合には,抗 Ri 抗体がしばしば同定される 36。抗 Ri 抗
の症例は重度かつ致命的であった。ほとんどの症例で
体は,肺癌,乳癌,子宮頸癌,膀胱癌に伴う事が多い 36。
25,26
27
28
CSF および MRI 脳スキャン所見は完全に正常であるが,
少数例で脳幹と小脳に非特異的変化が認められている 28。
管理および予後
発症は亜急性で,きわめて重症で,患者の 30%は 1 ヵ
病因
月以内に車椅子生活となることが多いが,オプソクロー
傍腫瘍性 OMS 症例の半数では,脳幹または小脳に病
ヌスは自然寛解する場合もあれば,再発と寛解を繰り返
理学的変化は認められていない。ただし,小脳萎縮と血
す経過をとる場合もある。小児では,症例の 70 ~ 80%
管周囲へのリンパ球浸潤(cuffing)を示す症例が報告さ
で著しい神経障害,認知障害,行動障害が長期に残り,
れている
これらは腫瘍を治療しても改善しない 25,26。ただし,神経
。オプソクローヌスは脳幹のオムニポーズ
29,30
ニューロンの障害が原因であると考えられている 31。
芽 細 胞 腫 に 伴う OMS では,副 腎 皮 質 刺 激 ホ ル モン
OMS の抗体は小児ではめったに検出されないが,一部の
(adrenocorticotropic hormone; ACTH)や高用量デキサメ
患児はプルキンエ細胞の細胞質と結合する IgM および
タゾンパルス療法 37,ivIg または血漿交換 38,39 による治
IgG 抗体をもっている。腫瘍周囲の著明なリンパ球浸潤
療で,良好な臨床的軽快が得られたとの報告が多数ある。
から,腫瘍抗原に対する T 細胞依存性応答とそれに続く
オプソクローヌスが消失しても,正式な検査を行うと,
B 細胞活性化が裏付けられる
追従眼球運動の異常や,程度は低いものの衝動性眼球運
。特異的自己抗原は同
32-34
定されていない。
動が持続して認められる 26。傍腫瘍性 OMS の成人では,
特に特発性の場合に自然軽快や免疫療法への反応がみら
診断
れることがある 27。抗 CD20 モノクローナル抗体のリツ
小児では,軽度のウイルス性脳炎に罹患した後に OMS
キシマブは,補助療法として有用な場合がある 40。成人
が生じる場合がある 24,35。成人では,中脳出血,視床出血,
患者の生存期間は,基礎疾患の腫瘍の反応性とその腫瘍
もしくは腫瘍(例えば,
非ホジキンリンパ腫,
腎癌)に伴っ
の予後に左右される。
21
傍腫瘍性運動障害
単独ミオクローヌス(オプソクローヌスを伴わな
い)
診断
舞踏病,片側バリスム,ジストニアを引き起こす他の
単独ミオクローヌス(オプソクローヌスを伴わない)は,
原因,特に血管障害,感染症(HIV など)
,全身性エリテ
傍腫瘍性症候群の所見の 1 つとして生じることがある。
マトーデス(systemic lupus erythematosus; SLE)
,代謝性
抗 amphiphysin 抗体をもつ患者の 6%は,臀部,脊柱,四
疾患,薬剤(ラモトリジン,メタドン,リチウムなど)を
肢または横隔膜にミオクローヌスを有し,振戦,ジスト
除外しなければならない 45。舞踏病,片側バリスム,ジ
ニア,舞踏病,筋強剛など,その他の運動障害を併発す
ストニアを引き起こす血管性または構造的な病変は,通
ることもある 。Amphiphysin 関連のミオクローヌスで,
常,画像検査により除外できる。MRI スキャンは正常ま
基礎疾患の腫瘍として最も頻度が高いのは,肺癌(64%)
,
たは軽微な大脳基底核異常を示す。ただし,占拠性病変
乳癌(32%)
,黒色腫(4%)である。傍腫瘍性の固有脊
がみられる症例も報告されている 43。場合によっては,
髄性ミオクローヌス(propriospinal myoclonus)が甲状腺
MRI 所見から腫瘍の疑いが浮上することもある。そのた
乳頭癌に伴い発症した事が報告されている。いずれの抗
め,一部の症例では生検も行われている 46。CSF は正常
体も同定されていない 42。
または蛋白質増加を伴う軽度の白血球増多を示し,オリ
41
ゴクローナルバンドが認められる場合もある 47。
傍腫瘍性大脳基底核障害
抗体陽性の頻度が最も高いのは,抗 CRMP5/CV2 抗体
である。この抗体が同定されたとき,基礎疾患の腫瘍と
傍腫瘍性大脳基底核障害は稀であるが,一般に次の型
してよくみられるのが,肺癌(81%)
,腎癌,胸腺腫,リ
に分けられる。すなわち,初発症状が運動障害で後によ
ンパ腫である 46,48。抗 CRMP5 抗体陽性患者 121 例を対
り広汎な CNS 傍腫瘍性症候群となる運動過多型と,しば
象とした研究では,大部分の患者で多巣性の神経学的徴
しば発熱・意識レベルの低下・痙攣・その他の所見を伴
候が認められた 20。舞踏病は患者の 11%で認められたが,
う急性で重症の運動減少型である。
最も多い所見は末梢ニューロパチー(47%)
,自律神経
ニューロパチー(31%)
,小脳性運動失調症(26%)
,亜
臨床像
急性認知症(25%)
,神経筋接合部障害(12%)
,脳神経
傍腫瘍性の舞踏病,片側バリスム,ジスキネジア,ジ
ニューロパチー(17%)であった。傍腫瘍性舞踏病と抗
ストニアが報告されている。正確な発症率を示すことは
CRMP5/CV2 抗体は,辺縁系脳炎 44 と視神経炎 18 に併存
できないが,発症はきわめて稀である。通常,亜急性に
する形で認められている。抗 NMDAR 抗体は,卵巣また
生じ,重度で,急速に進行し,しばしば薬剤抵抗性である。
は精巣奇形腫を有し口腔顔面ジスキネジアとジストニア
傍腫瘍性神経症候群で抗 CRMP5/CV2 抗体陽性の症例で
を伴う脳炎症例の一部で同定されている 49。
は,通常,舞踏病が初発症状であると同時に最も顕著な
症状でもある(69%)
。非対称性または一側性である場合
管理および予後
が多いが(31%)
,進行すると 87.5%の患者でより広汎な
舞踏病,ジストニア,ジスキネジアは,通常の治療に
CNS 障害がみられるようになる 。傍腫瘍性大脳基底核
は抵抗性の場合が多い。早期に診断された場合には,メ
運動障害を呈する全例で,脳脊髄炎関連の自己抗体がみ
チルプレドニゾロン,ivIg あるいは血漿交換による治療
られる。また,精神障害や行動障害 ,辺縁系脳炎 ,
が妥当であろう。腫瘍に対する化学療法またはメチルプ
視神経炎
レドニゾロン静注で,大脳基底核の症状も改善したと思
18
43
45
44
を伴う場合もある。
われる症例も存在する 44,49,50。
病因
非定型パーキンソン病症状
病理学的所見としては,他の傍腫瘍性神経症候群と同
様に,血管周囲炎とミクログリア活性化が認められてい
る。片側バリスムを呈した一例では,MRI で異常が認め
られた大脳基底核の生検で,限局性の脳炎性変化が明ら
かにされた 。
46
22
臨床像
傍腫瘍性の原因によるパーキンソニズムはいかなる
CNS 傍腫瘍性脳脊髄炎でも生じうるが,非常に稀である
R. Grant and F. Graus
Stiff person 症候群
(Table 1 参照)
。脳幹病変は患者の 53%で認められる 51。
垂直性注視麻痺はよくみられ(60%)
,時に完全外眼筋麻
痺を伴う。一部の患者に運動機能低下,重度筋強剛ある
いは蠟屈症を伴う緊張病様所見や,閉眼,発語減少の傾
向が認められた
臨床像
Stiff person 症候群(stiff person syndrome; SPS)は,体
。本症候群は,頭痛,発熱,不安な
幹の筋強剛と間欠的かつ有痛性の攣縮を特徴とする稀な
どのウイルス性感染症の前駆症状に似た症状の後に発症
疾患である。自己免疫性,傍腫瘍性,特発性の 3 つの病
することが多く,自律神経不安定症,低換気,高体温を
型が報告されている。SPS は男性よりも女性に多い
(30%:
続 発 する場 合もあり,筋 強 剛,しかめ 顔,腹 部 収 縮
70%)
。SPS の類型(variant)には,stiff limb 症候群,
(abdominal contraction)
,間欠性ジストニアを伴う 。経
jerking stiff person 症候群,筋強剛とミオクローヌスを伴
過観察中に急速に進行し,原因不明の発熱,末梢ニュー
う進行性脳炎(progressive encephalitis with rigidity and
ロパチー,CSF 異常を示した後,潜在性の B 細胞リンパ
myoclonus; PERM)がある 59。体幹の屈曲を妨げる腰部
腫が検出された亜急性核上性麻痺の症例が報告されてい
脊柱過前彎がみられる場合がある。症状は変動し,睡眠
る 。この男性患者は重度神経障害に伴った合併症のた
中は改善するが,ストレッチング,情動あるいは感覚性
め死亡した。肺がん患者に合併した,パーキンソニズム
刺激によって誘発される。転倒や骨折の原因となりうる
や多系統萎縮症の症例も報告されている
攣縮やミオクローヌス反射を併発する場合がある。疼痛
51-53
52
54
。
55-57
を伴うこともある。経過は緩徐であるが確実に進行する。
病因
SPS 症例の 50 ~ 90%では,グルタミン酸脱炭酸酵素
運動減少型の大脳基底核障害の病因は,他の脳脊髄炎
(glutamic acid decarboxylase; GAD)に対する自己抗体が
の場合と同様に考えられており,
,大脳基底核の変性が
陽性である。抗 GAD 抗体陽性 SPS と器官特異的自己免
いっそう強調されているだけである 55-56。
疫性疾患(例えば,原発性インスリン依存性糖尿病)と
の合併がよく見られるが,他の自己免疫的な障害がみら
診断
れない腎癌症例も報告されている 60。
傍腫瘍性の運動減少型大脳基底核障害の鑑別診断で
SPS 全体としてみると,基礎疾患の癌と合併するのは,
は,癌の直接的影響,水頭症,感染症,血管性パーキン
症例の約 5%である。傍腫瘍性でない症例と傍腫瘍性の
ソニズムまたは進行性核上性麻痺を考慮する 。精神状
症例とを臨床的に鑑別する信頼性の高い方法はないが,
態の変化,筋強剛,自律神経失調症の三徴候は,セロト
通常,傍腫瘍性 SPS は抗 amphiphysin 抗体を伴う 41。あ
ニン症候群,致死性緊張病あるいは抗精神病薬による悪
る研究では,患者 13 例中 4 例(31%)が腫瘍と合併して
性症候群に類似すると考えられる。MRI では,傍腫瘍性
おり,この 4 例のうち 3 例が抗 amphiphysin 抗体をもっ
脳脊髄炎の最大 3/4 の症例に非特異的な大脳基底核の変
ていた 61。傍腫瘍性 SPS の発症は特徴的に速やかであり,
化を認める。
一肢のみが侵され,診断が困難な場合もある。本症では,
58
傍腫瘍性の病因と判断する糸口となるのは,亜急性の
脳脊髄ニューロパチーの一部として、一側または両側の
発症,数週間または数ヵ月間で急速に進行する経過,な
上肢のみが侵される場合や,感覚性ニューロパチーを伴
らびに症例の 86%でみられる CSF の炎症性変化である 20。
う場合も比較的多いと考えられる。抗 amphiphysin 抗体は,
傍腫瘍性自己抗体検査は,もし陽性であれば,原因を確
筋強剛を伴う進行性脳脊髄炎でも報告されている 62。この
定し,腫瘍原発巣の部位を推定することができる。運動
疾患は,筋強剛,異常姿勢,有痛性の筋攣縮およびミオ
減少型の症状はしばしば抗 Ma2 抗体関連脳炎患者に特徴
クローヌスを特徴とし,脳幹および脊髄の炎症を伴う 62。
的な所見となりうる。若年男性に抗 Ma2 抗体が存在する
場合には,精巣腫瘍の検索を行うべきである 53。
病因
いくつ か の 研 究 で 感 覚 運 動 皮 質のγ - アミノ酪 酸
管理および予後
(gamma amino butyric acid; GABA)の低下が見出され,
Ma2 関連脳炎患者の約 30%は腫瘍に対する治療,ある
いは免疫療法に反応する 。
51
責任抗原が同定されているかどうかにかかわらず,本症
候群には抑制性 GABA 経路が障害されていることが示唆
23
傍腫瘍性運動障害
されている 63。このように運動系での中枢性抑制が減弱
縮・線維束性収縮症候群(cramp fasciculation syndrome)
することで,体幹と四肢の筋肉に有痛性攣縮が生じる。
あるいは CNS 所見も認められる Morvan 症候群をきたし
血管周囲炎や,前庭神経核と脊髄のニューロン消失が認
うる自己免疫性の病態である。これらの 3 つの病態はい
められる場合もある 。本症候群の徴候を示すラットの
ずれも胸腺腫と合併することがあり,傍腫瘍性のことも
CNS では IgG 結合が証明された 。抗 GAD IgG を傍脊椎
ありうる 69。神経性筋強直症は末梢神経興奮性亢進症の
部に投与すると,腓腹筋に持続的な収縮が誘発された 65。
最も一般的な病型で,遺伝性の場合も後天性の場合もあ
amphiphysin に対する抗体を有する SPS をラットに移すこ
る 70。後天性の病型は,自己免疫性の場合(糖尿病や慢
とができた。すなわち,ヒトの SPS に類似した攣縮を伴
性炎症性脱髄性ニューロパチーなどの後天性ニューロパ
う用量依存性の硬直を誘導できた 。この知見は,上記
チーに伴う)
,薬剤 / 毒素誘発性の場合,あるいは胸腺腫
抗体の直接的な病因的役割を裏付けている 。
やその他の腫瘍に関連する傍腫瘍性の場合がある。本疾
41
64
64
66
患ではミオキミア〔
「虫を入れた袋(bag of worms)
」と形
診断
容される,筋の持続的でうねるような運動〕
,強直を伴う
筋電図検査(electromyography; EMG)で随意運動時の
有痛性攣縮,手足攣縮,筋収縮後の弛緩障害(偽性筋強
ような持続活動電位が認められ,体幹筋で最も顕著であ
直症)が認められる。運動により増悪する遠位筋の硬直,
れば,臨床的に SPS が支持される。持続時間 50 ~ 60 ミ
体重減少,脊柱後彎,構音障害あるいは嚥下障害がみら
リ秒の群化放電が,5 ~ 6 Hz で数多く見られ,それらが
れる場合もある。運動は睡眠中も持続し,全身麻酔下で
攣縮により中断されている。SPS の 80%では CSF 中にオ
も軽快しない 70。Morvan 症候群では,神経性筋強直症に
リゴクローナルバンドが認められる。MRI スキャンは正
加え,幻覚,錯乱,不眠などの精神症状が認められる。
常所見を示す場合が多い。抗 amphiphysin 抗体は,傍腫
これらの病態の症例の 40%に抗電位依存性カリウム
瘍性と推定される症例を選び出すのに役立つが,この抗
チャネル(voltage gated potassium channel; VGKC)抗体
体は本病態に特異的ではない。抗 amphiphysin 抗体が血
が認められる。これらの抗体を有する症例のうち,25%
清中に検出された場合でも,実際に SPS を呈するのは女
もの患者に基礎疾患として腫瘍が認められている。胸腺
性 で は 39 %, 男 性 で は 12 % に す ぎ な い 。 抗
腫であることが多いが,肺癌,腎癌,リンパ腫あるいは
amphiphysin 抗体は主として乳癌に伴うが,肺癌や腎癌,
形質細胞腫の場合もある 71-74。傍腫瘍性の神経性筋強直
さらに胸腺腫での報告もある。女性では潜在性の乳癌を,
症は,しばしば自律神経障害(50%は多汗症を有する)
喫煙者では肺癌を検索するのが望ましい。
や感覚症状(33%)を随伴する。
管理および予後
病因
41
ベンゾジアゼピンあるいは GABA 作動性の抑制作用を
抗体は筋からのカリウム流出を減少させ,静止膜電位
増強する薬剤(例えば,バクロフェン,チザニジン,ク
を低下させて神経性筋強直性の放電を生じる 71,75。臨床
ロニジン)は攣縮を軽減するが,基礎にある病態には影
的な神経性筋強直症をマウスへ受動的に伝達することが,
響を及ぼさない。ステロイド,免疫グロブリン G 静注
神経性筋強直症患者から精製された IgG を注入すること
(intravenous injection of immunoglobulin G; ivIgG)
,血漿
で達成され,臨床的な病態が認められている 75。
交換,リツキシマブは,本病態を治療する目的で使用さ
れている 62,63,65,66。腎癌患者に対する ivIg と腎摘出術,乳
癌治療,胸腺腫に対する胸腺摘出術については,臨床的
な有効性が報告されている
。
67,68
診断
標準的な運動神経伝導検査の刺激後にしばしば後放電
がみられ,針 EMG では持続性の運動単位活動電位の発
火が認められる。最もよくみられる異常放電は,線維束
傍腫瘍性末梢神経興奮性亢進症
臨床像
末梢神経興奮性亢進症は,神経性筋強直症,有痛性攣
24
性収縮,二重放電または多重放電,ミオキミア性放電で
ある。抗 VGKC 抗体の血清検査は行うべきである。抗
VGKC 抗体は傍腫瘍性の病因に特異的なわけではない。
抗 VGKC 抗体は,本症候群の自己免疫型では 1/3 を超え
5. Dalmau J, Tüzün E, Wu HY, et al. Paraneoplastic anti-N-methylD-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol 2007;61:25–36.
6. Graus F, Delattre JY, Antoine JC, et al. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol
Neurosurg Psychiatry 2004;75:1135–1140.
7. Linke R, Schroeder M, Helmberger T, Voltz R. Antibody positive paraneoplastic neurological syndromes: value of CT and
R. Grant and F. Graus
PET for tumor diagnosis. Neurology 2004;63:282–286
8. Vedeler CA, Antoine JC, Giometto B, et al. Management of paraneoplastic neurological syndromes: report of an EFNS Task
Force. Eur J Neurol 2006;13:682–690.
る患者で認められる。ただし,
基礎疾患に胸腺腫があると,
9. Shams’ili S, Grefkens J, de Leeuw B, et al. Paraneoplastic cere75
これらの抗体をもつ患者は 80%に達する 。腰椎穿刺で
bellar degeneration associated with antineuronal antibodies: analysis of 50 patients. Brain 2003;126:1409–1418.
オリゴクローナルバンドが認められる場合もある。胸部 /
10. Hammack JE, Kotanides H, Rosenblum MK, Posner JB. Paraneoplastic cerebellar degeneration: clinical and immunological find腹部の CT/MRI スキャンによって症例の 25%で腫瘍,特
ings in 21 patients with Hodgkin’s disease. Neurology 1992;42:
1938–1943.
に胸腺腫,肺癌,腎癌,リンパ腫 / 形質細胞腫が同定さ
11. Nakao YK, Motomura M, Fukudome T, et al. Seronegative Lambert-Eaton myasthenic syndrome: study of 110 Japanese patients.
れる。抗 Hu 抗体陽性の肺小細胞癌患者の一例で,傍腫
Neurology 2002;59:1773–1775.
12. Bernal F, Shams’ili S, Rojas I, et al. Anti-Tr antibodies as
瘍性末梢神経興奮性亢進症(paraneoplastic peripheral
markers of paraneoplastic cerebellar degeneration and Hodgkin’s
nerve hyperexcitability; PPNH)が認められ,基礎疾患とし
disease. Neurology 2003;60:230–234.
13. Mason WP, Graus F, Lang B, et al. Small cell lung cancer, paraてホジキンリンパ腫や形質細胞腫を有し抗体陰性の患者
neoplastic cerebellar degeneration and Lambert-Eaton Myasthenic Syndrome. Brain 1997;120:1279–1300.
でも PPNH が報告されている 73,75,76。
14. Petersen K, Rosenblum MK, Kotanides H, Posner JB. Paraneoplastic cerebelaar degeneration: a clinical analysis of 55 anti-Yo
antibody positive patients. Neurology 1992;42:1931–1937.
15. Lucchinetti CF, Kimmel DW, Lennon VA. Paraneoplastic and
管理および予後
oncologic profiles of patients seropositive for type 1 antineuronal
PPNH/ 筋強直症の症状は,フェニトイン,カルバマゼ
nuclear auto-antibodies. Neurology 1998;50:652–657.
16. Graus F, Keime-Guibert F, Rene R, et al. Anti-Hu associated
ピン,ガバペンチン,ダントロレンナトリウムで改善可
paraneoplastic encephalomyelitis: analysis of 200 patients. Brain
2001;124:1138–1148.
能である。また,基礎疾患の腫瘍に対する治療,免疫グ
17. Chan KH, Vernino S, Lennon VA. ANNA-3 antineuroanl nuclear
antibody: marker of lung cancer related autoimmunity. Ann Neuロブリン・血漿交換・ステロイドおよびアザチオプリンに
rol 2001;50:301–311.
18. Vernino S, Tuite P, Adler CH, et al. Paraneoplastic chorea assoよる免疫療法でも,筋強直症は軽快する可能性がある 77。
ciated with CRMP-5 neuronal autoantibody and lung carcinoma.
胸腺腫の予後は良好である 78。胸腺腫の大部分はステー
Ann Neurol 2002;51:625–630.
19. de la Sayette V, Bertran F, Honnorat J, Schaeffer S, Iglesias S,
ジⅠないしステージⅠ
Ⅰであり,患者の 80%は 20 年間生存
Defer G. Paraneoplastic cerebellar syndrome and optic neuritis
with anti-cv2 antibodies. Arch Neurol 1998;55:405–408.
79
する 。基礎疾患に癌のある症例の生存期間は,その腫
PARANEOPLASTIC20.DISORDER
1723
Yu Z, Kryzer TJ, Griesmann GE, Kim K, Benarroch EE, Lennon
VA. CRMP-5 neuronal autoantibody: marker of lung cancer and
瘍が治療可能かどうかに左右される。
thymoma-related autoimmunity Ann Neurol 2001;49:146–154.
21. Honnorat J, Antoine JC, Derrington E, Aguera M, Belin MF.
neoplastic syndromes, has advised on other important literaAntibodies to a paraneoplastic neurological syndromes. J Neurol
ture, and advised on design and content of the article in subNeurosurg Psychiatry 1996;61:270–276.
著者の役割
sequent drafts.
PARANEOPLASTIC22.
DISORDER
1723
Uchya M, Graus F, Rene R, Delattre JY. Intravenous immunoR. Grant は,本論文の構想の立案,現在入手可能な文献の
globulin treatment in paraneoplastic neurological syndromes with
antineuronal autoantibodies. J Neurol Neurosurg Psychiatry 1996;
検索,本総説の初稿の作成を担当した。F. Graus は傍腫瘍性
60:388–392.
21. Honnorat
J, Antoine JC, Derrington E, Aguera M, Belin MF.
neoplastic syndromes, REFERENCES
has advised on other important litera症候群の幅広い論文執筆経験があり,他の重要文献について
23.Antibodies
Counsell C,
M, Grantneurological
R. Reversalsyndromes.
of subacuteJ paraneoto McLeod
a paraneoplastic
Neurol
ture, and advised on design and content of the article in subplastic cerebellar
with intravenous immunoglobulin.
Neurosurg
Psychiatrysyndrome
1996;61:270–276.
1. Pittock
SJ, Kryzer TJ, Lennon
VA. Paraneoplastic antibodies
sequent
drafts.
アドバイスするとともに,第
2 稿以降では論文のデザインと
NeurolM,
1994;44:1184–1185.
22. Uchya
Graus F, Rene R, Delattre JY. Intravenous immunocoexist and predict cancer, not neurological syndrome. Ann Neu24.globulin
Wong A.
An update
on opsoclonus.neurological
Curr Opin syndromes
Neurol 2007;20:
treatment
in paraneoplastic
with
内容について助言した。
rol 2004;56:715–719.
25–31.
antineuronal
autoantibodies. J Neurol Neurosurg Psychiatry 1996;
2. Roberts WK, Darnell RB. Neuroimmunology of paraneoplastic
25.60:388–392.
Rudnick E, Khakoo Y, Antunes NL, et al. Opsoclonus-Myocloneurological degenerations.
Curr Opin Immunol 2004;16:616–622.
REFERENCES
REFERENCES
nus-Ataxia
syndromeM,inGrant
neuroblastoma:
outcome
and
23. Counsell
C, McLeod
R. Reversal clinical
of subacute
paraneo3. Graus F, Lang B, Pozo-Rosich P, Saiz A, Casamitjana R, Vinantineuronal
antibodies-a
report
the children’s
cancer group
plastic
cerebellar
syndrome
withfrom
intravenous
immunoglobulin.
cent A.SJ,P/QKryzer
type calcium
channel
in paraneoplastic
1. Pittock
TJ, Lennon
VA.antibodies
Paraneoplastic
antibodies
study. 1994;44:1184–1185.
Med Pediatr Oncol 2001;36:612–622.
Neurol
cerebellar
degeneration
lung cancer.syndrome.
NeurologyAnn
2002;59:
coexist
and predict
cancer,with
not neurological
Neu26.Wong
Mitchell
WG,update
Davalos-Gonzalez
Y, Curr
Brumm
VL,
et al. 2007;20:
Opsoclo24.
A. An
on opsoclonus.
Opin
Neurol
764–766.
rol
2004;56:715–719.
nus-ataxia caused by childhood neuroblastoma: developmental
25–31.
Coesmans
M,Darnell
SillevisRB.
Smitt
PA, Linden DJ, et
Mechanisms
2.4.Roberts
WK,
Neuroimmunology
of al.
paraneoplastic
and neurological
sequelae.
Pediatrics
2002;109:86–98.
25. Rudnick
E, Khakoo
Y, Antunes
NL, et
al. Opsoclonus-Myoclounderlying cerebellar
motor
deficits
to mGluR1-autoantibodneurological
degenerations.
Curr
Opin due
Immunol
2004;16:616–622.
27.nus-Ataxia
Bataller L,syndrome
Graus F, inSaiz
A, Vilchez JJ.
Clinical
outcome
neuroblastoma:
clinical
outcome
andin
ies. Ann
NeurolB,2003;53:325–336.
3. Graus
F, Lang
Pozo-Rosich P, Saiz A, Casamitjana R, Vinadult onset antibodies-a
idiopathic orreport
paraneoplastic
opsoclonus-myoclonus.
antineuronal
from the children’s
cancer group
5.cent
Dalmau
J, Tüzün
Wu HY,
et al. antibodies
Paraneoplastic
anti-N-methylA. P/Q
type E,
calcium
channel
in paraneoplastic
Brain Med
2001;124:437–443.
study.
Pediatr Oncol 2001;36:612–622.
D-aspartate
receptor encephalitis
with ovarian
teracerebellar
degeneration
with lung associated
cancer. Neurology
2002;59:
28.Mitchell
Ohara S,WG,
Iijima
N, Hayashida K,Y,Oide
T, Katai
Autopsy
case
26.
Davalos-Gonzalez
Brumm
VL, S.
et al.
Opsoclotoma. Ann Neurol 2007;61:25–36.
764–766.
of opsoclonus-myoclonus-ataxia
and cerebellar cognitive
affecnus-ataxia
caused by childhood neuroblastoma:
developmental
Graus F, Delattre
JY, Smitt
Antoine
et al. DJ,
Recommended
diagnos4.6.Coesmans
M, Sillevis
PA,JC,
Linden
et al. Mechanisms
tiveneurological
syndrome associated
with small2002;109:86–98.
cell carcinoma of the lung.
and
sequelae. Pediatrics
tic criteriacerebellar
for paraneoplastic
neurological
syndromes. J Neurol
underlying
motor deficits
due to mGluR1-autoantibodMov Disord
2007;22:1320–1324.
27. Bataller
L, Graus
F, Saiz A, Vilchez JJ. Clinical outcome in
Neurosurg
Psychiatry
2004;75:1135–1140.
ies.
Ann Neurol
2003;53:325–336.
29.adult
Baetsonset
J, Pals
P, Bergmans
B, et al. Opsoclonus-myoclonus
synidiopathic
or paraneoplastic
opsoclonus-myoclonus.
Linke R,
Schroeder
M, HY,
Helmberger
T, Voltz R. anti-N-methylAntibody posi5.7.Dalmau
J, Tüzün
E, Wu
et al. Paraneoplastic
drome:
a colinicopathological confrontation. Acta Neurol Belg
Brain
2001;124:437–443.
tive paraneoplastic
syndromes:with
value
of CTteraand
D-aspartate
receptor neurological
encephalitis associated
ovarian
2006;106:142–146.
28. Ohara
S, Iijima N, Hayashida K, Oide T, Katai S. Autopsy case
PET Ann
for tumor
diagnosis.
Neurology 2004;63:282–286
toma.
Neurol
2007;61:25–36.
30.ofGiordana
MT, Soffietti R, Schiffer
Paraneoplastic
opsoclonus:
opsoclonus-myoclonus-ataxia
andD.cerebellar
cognitive
affecVedeler
CA, Antoine
JC, Giometto
al. Management
of par6.8.Graus
F, Delattre
JY, Antoine
JC, etB,
al.etRecommended
diagnosa neuropathologic
study with
of two
cases.
Neuropathol
tive
syndrome associated
small
cellClin
carcinoma
of the1989;8:
lung.
aneoplastic
syndromes:
report
of an EFNS
Task
tic
criteria forneurological
paraneoplastic
neurological
syndromes.
J Neurol
295–300.
Mov
Disord 2007;22:1320–1324.
Force. EurPsychiatry
J Neurol 2006;13:682–690.
Neurosurg
2004;75:1135–1140.
31.Baets
RidleyJ, A,
Kennard
C, Scholtz
JA, Summers
29.
Pals
P, Bergmans
B, etCL,
al.Büttner-Ennever
Opsoclonus-myoclonus
synShams’ili
S, Grefkens
de Leeuw B,
al. Paraneoplastic
cere7.9.Linke
R, Schroeder
M, J,Helmberger
T, et
Voltz
R. Antibody posiB, Turnbull
A. Omnipause neurons
in two cases
opsoclonus
drome:
a colinicopathological
confrontation.
Acta of
Neurol
Belg
bellar
degeneration neurological
associated with
antineuronal
antibodies:
tive
paraneoplastic
syndromes:
value
of CT analand
associated with oat cell carcinoma of the lung. Brain 1987;110:
2006;106:142–146.
ysis for
of 50
patients.
BrainNeurology
2003;126:1409–1418.
PET
tumor
diagnosis.
2004;63:282–286
1699–1709.
30. Giordana
MT, Soffietti R, Schiffer D. Paraneoplastic opsoclonus:
10.
Hammack
Kotanides
H, Rosenblum
Posner JB. Paraneo8. Vedeler
CA,JE,
Antoine
JC, Giometto
B, et MK,
al. Management
of par32.aPranzatelli
MR, Tate
ED,
A, et
al. Neuropathol
Screening for1989;8:
autoanneuropathologic
study
ofWheeler
two cases.
Clin
plastic cerebellar
degeneration:
clinical
and of
immunological
findaneoplastic
neurological
syndromes:
report
an EFNS Task
tibodies in children with opsoclonus myoclonus ataxia. Pediatr
295–300.
ings inEur
21J patients
with Hodgkin’s disease. Neurology 1992;42:
Force.
Neurol 2006;13:682–690.
NeurolA,2002;27:384–387.
31. Ridley
Kennard C, Scholtz CL, Büttner-Ennever JA, Summers
1938–1943.
9. Shams’ili
S, Grefkens J, de Leeuw B, et al. Paraneoplastic cere33.B,Bataller
L, A.
Rosenfeld
MR,neurons
Graus in
F, two
Vilchez
NK,
Turnbull
Omnipause
casesJJ,of Cheung
opsoclonus
11.bellar
Nakaodegeneration
YK, Motomura
M, Fukudome
T, et al. Seronegative
Lamassociated
with antineuronal
antibodies: analDalmau J.with
Autoantigen
diversity of
in the
the lung.
opsoclonus-myoclonus
associated
oat cell carcinoma
Brain 1987;110:
bert-Eaton
myasthenic
study of 110 Japanese patients.
ysis
of 50 patients.
Brainsyndrome:
2003;126:1409–1418.
syndrome. Ann Neurol 2003;53:347–353.
1699–1709.
NeurologyJE,
2002;59:1773–1775.
10. Hammack
Kotanides H, Rosenblum MK, Posner JB. Paraneo34.Pranzatelli
Caviness JN,
PA,
LaytonA,DD,
TJ. for
Theautoanmove32.
MR,Forsyth
Tate ED,
Wheeler
et al.McPhee
Screening
12.plastic
Bernalcerebellar
F, Shams’ili
S, Rojasclinical
I, et al.
antibodies
degeneration:
andAnti-Tr
immunological
find-as
ment disorder
of adult
opsoclonus.
Mov
Disord 1995;10:22–27.
tibodies
in children
with
opsoclonus
myoclonus
ataxia. Pediatr
markers
paraneoplastic
cerebellardisease.
degeneration
and Hodgkin’s
ings
in 21ofpatients
with Hodgkin’s
Neurology
1992;42:
35.Neurol
Martino
D, Giovannoni G. Autoaggressive immune mediated
2002;27:384–387.
disease. Neurology 2003;60:230–234.
1938–1943.
movement
33. Bataller
L, disorders.
Rosenfeld Adv
MR,Neurol
Graus2005;96:320–335.
F, Vilchez JJ, Cheung NK,
13.Nakao
MasonYK,
WP,Motomura
Graus F, Lang
B, et al. Small
cellSeronegative
lung cancer,Lampara11.
M, Fukudome
T, et al.
36.Dalmau
Pittock SJ,
Lucchinetti CF,
LennoninVA.
nuclear auJ. Autoantigen
diversity
the Antineuronal
opsoclonus-myoclonus
neoplastic myasthenic
cerebellar syndrome:
degeneration
Lambert-Eaton
Myasbert-Eaton
studyand
of 110
Japanese patients.
toantibodyAnn
typeNeurol
2: paraneoplastic
accompaniments. Ann Neurol
syndrome.
2003;53:347–353.
thenic Syndrome.
Brain 1997;120:1279–1300.
Neurology
2002;59:1773–1775.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
25
adult onset idiop
Brain 2001;124:4
Ohara S, Iijima N
of opsoclonus-my
tive syndrome as
Mov Disord 2007
Baets J, Pals P, B
drome: a colinic
2006;106:142–146
Giordana MT, So
a neuropathologic
295–300.
Ridley A, Kennar
B, Turnbull A. O
associated with o
1699–1709.
Pranzatelli MR, T
tibodies in childr
Neurol 2002;27:3
Bataller L, Rose
Dalmau J. Autoa
syndrome. Ann N
Caviness JN, For
ment disorder of
Martino D, Giov
movement disorde
Pittock SJ, Lucch
toantibody type 2
2003;53:580–587.
Ertle F, Behnisch
blastoma related
high dose dexame
365–608.
Yiu VW, Kovith
pheresis as an eff
drome. Pediatr Ne
Armstrong MB,
opsoclonus-myocl
Pediatr Neurol 20
Bell J, Moran C,
neuroblatoma and
2008;50:370–371.
Pittock SJ, Lucch
munity: paraneop
96–107.
Attarian H, Apple
with papillary thy
Muehlschlegel S,
Fernandez HH. P
tz R. Antibody posis: value of CT and
3:282–286
Management of parof an EFNS Task
Paraneoplastic cereonal antibodies: anal18.
, Posner JB. Paraneoimmunological findNeurology 1992;42:
l. Seronegative Lam10 Japanese patients.
nti-Tr antibodies as
ration and Hodgkin’s
ell lung cancer, paraambert-Eaton Myas0.
Posner JB. Paraneonalysis of 55 anti-Yo
42:1931–1937.
. Paraneoplastic and
r type 1 antineuronal
652–657.
. Anti-Hu associated
f 200 patients. Brain
antineuroanl nuclear
immunity. Ann Neu-
oplastic chorea assoand lung carcinoma.
haeffer S, Iglesias S,
me and optic neuritis
55:405–408.
enarroch EE, Lennon
r of lung cancer and
2001;49:146–154.
26
29. Baets J, Pals P, Bergmans B, et al. Opsoclonus-myoclonus synintratubular germ cell neoplasm of the testes. Mov Disord 2007;
drome: a colinicopathological confrontation. Acta Neurol Belg
22:728–731.
2006;106:142–146.
53. Pruss H, Voltz R, Flath B, et al. Anti-Ta associated paraneoplas30. Giordana MT, Soffietti R, Schiffer D. Paraneoplastic opsoclonus:
tic encephalitis with occult testicular intratubular germ cell neoa neuropathologic study of two cases. Clin Neuropathol 1989;8:
plasia. J Neurol Neurosurg Psychiatry 2007;78:651–652.
295–300.
54. Tan JH, Goh BC, Tambyah PA, Wilder-Smith E. Paraneoplastic
31. Ridley A, Kennard C, Scholtz CL, Büttner-Ennever JA, Summers
progressive supranuclear palsy in a patient with B cell lymB, Turnbull A. Omnipause neurons in two cases of opsoclonus
phoma. Parkinsonism Relat Disord 2005;11:187–191.
傍腫瘍性運動障害
associated with oat cell carcinoma of the lung. Brain 1987;110:
55. Fahn S, Brin MF, Dwork AJ, Weiner WJ, Goetz CG, Rajput AH.
1699–1709.
Case 1, 1996: rapidly progressive Parkinsonism, incontinence,
32. Pranzatelli MR, Tate ED, Wheeler A, et al. Screening for autoanimpotency, and levodopa-induced moaning in a patient with multibodies in children with opsoclonus myoclonus ataxia. Pediatr
tiple myeloma. Mov Disord 1996;11:298–310.
Neurol 2002;27:384–387.
56. Golbe LI, Miller DC, Duvoisin RC. Paraneoplastic degeneration
33. Bataller L, Rosenfeld MR, Graus F, Vilchez JJ, Cheung NK,
of the substantia nigra with dystonia and Parkinsonism. Mov DisDalmau J. Autoantigen diversity in the opsoclonus-myoclonus
ord 1989;4:147–152.
syndrome. Ann Neurol 2003;53:347–353.
57. Schluter E, Domm S, Erdag S. A case of rapidly progressive
34. Caviness JN, Forsyth PA, Layton DD, McPhee TJ. The movemultiple system degeneration: morphological findings and pathoment disorder of adult opsoclonus. Mov Disord 1995;10:22–27.
genic implications. Acta Neuropathol 2002;103:395–300.
35. Martino D, Giovannoni G. Autoaggressive immune mediated
58. Josephs KA, Ishizawa T, Tsuboi Y, Cookson N, Dickson DW. A
movement disorders. Adv Neurol 2005;96:320–335.
clinicopathological study of vascular progressive supranuclear
36. Pittock SJ, Lucchinetti CF, Lennon VA. Antineuronal nuclear aupalsy: a multi-infarct disorder presenting as progressive supranutoantibody type 2: paraneoplastic accompaniments. Ann Neurol
clear palsy. Arch Neurol 2002;59:1597–1601.
2003;53:580–587.
59. Meinck HM, Thompson PD. Stiff man syndrome and related
37. Ertle F, Behnisch W, Ali Al Mulla N, et al. Treatment of neuroconditions. Mov Disord 2002;17:853–866.
1724
R. GRANT
F. GRAUS
blastoma related opsoclonus-myoclonus-ataxia syndrome
with AND 60.
McHugh JC, Murray B, Renganathan R, Connolly S, Lynch T.
high dose dexamethasone pulses. Pediatr Blood Cancer 2007;45:
GAD antibody positive stiff person syndrome in a patient with
365–608.
renal cell carcinoma. Mov Disord 2007;22:1343–1346.
presenting
with obsessive-compulsive
disorder.
61. Grimaldi LM, Martino G, Braghi S, Quattrini A, Furlan R, Bosi
38. Yiu
VW, Kovithavongs
T, McGonigle and
LF, behavioural
Ferreira P. PlasmaMov Disord
E, Comi G. Heterogeneity of autoantibodies in stiff man synpheresis
as an2005;20:1523–1527.
effective treatment for opsoclonus-myoclonus syn44. drome.
Kinirons
P, Fulton
A,2001;24:72–74.
Keoghan M, Brennan P, Farrell M. Paradrome. Ann Neurol 1993;34:57–64.
Pediatr
Neurol
neoplastic limbic
encephalitis
chorea
associated
with
62. Ishii A, Hayashi A, Ohkoshi N, Matsuno S, Shoji S. Progressive
39. Armstrong
MB, Robertson
PL,(PLE)
CastleandVP.
Delayed,
recurrent
CRMP-5 neuronal antibody.
Neurology
2003;61:1623–1624.
encephalomyelitis with rigidity associated with anti-amphiphysin
opsoclonus-myoclonus
syndrome
responding
to plasmapheresis.
45. Pediatr
MartinoNeurol
D, Giovannoni
G. Anti-basal Ganglia antibodies and
antibodies. J Neurol Neurosurg Psychiatry 2004;75:661–662.
2005;33:365–367.
theirJ,relevance
movement
disorders.
Curr Opin
63. Levy LM, Levy-Reis I, Fijii M, Dalakis MC. Brain gamma ami40. Bell
Moran C,toBlatt
J. Response
to rituximab
in Neurol
a child 2004;
with
17:425–432. and opsoclonus myoclonus. Pediatr Blood Cancer
nobutyric acid changes in Stiff Person Syndrome. Arch Neurol
neuroblatoma
46. 2008;50:370–371.
Kujawa KA, Niemi VR, Tomasi MA, Mayer NW, Cochran E,
2005;62:970–974.
Goetz CG.
Ballistic–choreic
movements
the presentingautoimfeature
64. Sommer C, Weishaupt A, Brinkhoff J, et al. Paraneoplastic stiff41. Pittock
SJ, Lucchinetti
CF, Parisi
JE, et al.asAmphiphysin
of renal paraneoplastic
cancer. Arch Neurol
2001;58:1133–1135.
person syndrome: passive transfer to rats by means of IgG antimunity:
accompaniments.
Ann Neurol 2005;58:
47. 96–107.
Stich O, Jarius S, Kleer B, Rasiah C, Voltz R, Rauer S. Specific
bodies to amphiphysin. Lancet 2005;365:1406–1411.
antibodyH,index
in theG,
cerebrospinal
fluid
from patientsmyoclonus
with cen65. Manto MU, Laute MA, Aguera M, Rogemond V, Pandolfo M, Hon42. Attarian
Applebee
von Lepel A.
Paraneoplastic
1724
R. GRANT
tral and
peripheral
paraneoplastic
neurological
syndromes.
J Neu-AND F. GRAUS
norat J. Effects of anti-glutamic acid decarboxylase antibodies assowith
papillary
thyroid
carcinoma. Eur
Neurol 2007;58:182–183.
roimmunol 2007;183:220–224.
ciated with neurological diseases. Ann Neuol 2007;61:544–551.
43. Muehlschlegel
S, Okun MS, Foote KD, Coco D, Yachnis AT,
48. Fernandez
Samii A, HH.
Dahlen
DD, Spencechorea
AM, with
Maronian
NC, Kraus EE,
66. Dalakas MC. Advances in the pathogenesis and treatment of
Paraneoplastic
leukoencephalopathy
Lennon VA.
movementand
disorder
in a patient
with
patients LM,
with Martino
Stiff Person
Syndrome.
Curr Neurol
Neurosci
Rep
presenting
withParaneoplastic
obsessive-compulsive
behavioural
disorder.
61. Grimaldi
G, Braghi
S, Quattrini
A, Furlan
R, Bosi
Movement
Disorders,
Vol. 24, No. 12,
non-Hodgkin’s
lymphoma and CRMP-5 autoantibody. Mov DisMov
Disord 2005;20:1523–1527.
E,2008;8:45–55.
Comi
G. Heterogeneity
of 2009
autoantibodies in stiff man synord 2003;18:1156–1158.
67.drome.
Essalmi
L,Neurol
Meaux-Ruault
N, Hafsaoui C, Gil H, Curlier E,
44. Kinirons
P, Fulton A, Keoghan M, Brennan P, Farrell M. ParaAnn
1993;34:57–64.
49.neoplastic
Sansing LH,
Tuzun
E, Ko MW,
Baccon
Lynchassociated
DR, Dalmau
Dupond
JL. Stiff
withS,thymoma.
Efficacy of
limbic
encephalitis
(PLE)
and J,
chorea
withJ.
62. Ishii
A, Hayashi
A, person
Ohkoshisyndrome
N, Matsuno
Shoji S. Progressive
Disorders,
Vol. 24,receptor
No. 12, 2009
A patientneuronal
with encephalitis
associated
with NMDA
antithymectomy. Revwith
Medrigidity
Interne associated
2007;28:627–630.
CRMP-5
antibody.Movement
Neurology
2003;61:1623–1624.
encephalomyelitis
with anti-amphiphysin
bodies. Nat
Clin Pract Neurol
2007;3:291–296.
68.antibodies.
Wessig C,J Neurol
Klein R,
Schneider
MF, Toyka
KV, Naumann M,
45. Martino
D, Giovannoni
G. Anti-basal
Ganglia antibodies and
Neurosurg
Psychiatry
2004;75:661–662.
50.their
Croteau
D, Owainati
A, Dalmau
J, Rogers
Response
canSommer
Neuropathology
andDalakis
binding MC.
studies
in anti-amphiphyrelevance
to movement
disorders.
CurrLR.
Opin
Neurol to
2004;
63. Levy
LM,C.
Levy-Reis
I, Fijii M,
Brain
gamma amicer therapy in a patient with a paraneoplastic choreiform disorsin associated
person
Neurology
2003;61:195–198.
17:425–432.
nobutyric
acid stiff
changes
in syndrome.
Stiff Person
Syndrome.
Arch Neurol
der. Neurology
2001;57:719–722.
69.2005;62:970–974.
Newsom-Davis J. Neuromyotonia. Rev Neurol 2004;160:S85–S89.
46. Kujawa
KA, Niemi
VR, Tomasi MA, Mayer NW, Cochran E,
51.Goetz
Dalmau
Graus F, Villarejo
A, et al. as
Clinical
analysis feature
of anti70.Sommer
Gutmann
Gutmann A,
L. Brinkhoff
MyokymiaJ,and
Neuromyotonia.
NeuCG.J,Ballistic–choreic
movements
the presenting
64.
C,L,Weishaupt
et al.
Paraneoplastic Jstiffencephalitis.
Brain 2004;127:1831–1844.
rol 2004;251:138–142.
ofMa2-associated
renal cancer. Arch
Neurol 2001;58:1133–1135.
person
syndrome: passive transfer to rats by means of IgG anti52.Stich
Matsumoto
L, S,
Yamamoto
T, Higashihara
al. Severe
hypo71.bodies
Hart IK,
Maddison P,Lancet
Newsom-Davis
J, et al. Autoantibodies
47.
O, Jarius
Kleer B, Rasiah
C, VoltzM,
R, et
Rauer
S. Specific
to amphiphysin.
2005;365:1406–1411.
kinesia caused
anti-Ma2
encephalitis
associated
with
bilateral
detected
expressed
potassium
channels are
implicated
neuantibody
index inbythe
cerebrospinal
fluid from
patients
with
cen65. Manto
MU,toLaute
MA, Aguera
M, Rogemond
V, Pandolfo
M,inHonintratubular
germ paraneoplastic
cell neoplasm neurological
of the testes.syndromes.
Mov Disord
2007;
romyotonia.
Neurol 1997;41:238–246.
tral
and peripheral
J Neunorat
J. EffectsAnn
of anti-glutamic
acid decarboxylase antibodies asso22:728–731.
72.ciated
Hart with
IK, Maddison
Newsom-Davis
J, 2007;61:544–551.
Vincent A, Mills KR.
roimmunol
2007;183:220–224.
neurologicalP,diseases.
Ann Neuol
53.Samii
Pruss A,
H, Voltz
FlathSpence
B, et al.AM,
Anti-Ta
associated
Phenotypic
of peripheral
nerve hyperexcitability.
48.
DahlenR,DD,
Maronian
NC, paraneoplasKraus EE,
66. Dalakas
MC.variants
Advances
in the pathogenesis
and treatmentBrain
of
tic encephalitis
with occultmovement
testicular intratubular
cellwith
neo2002;125;1887–1895.
Lennon
VA. Paraneoplastic
disorder in agerm
patient
patients
with Stiff Person Syndrome. Curr Neurol Neurosci Rep
plasia. J Neurol
Neurosurgand
Psychiatry
73.2008;8:45–55.
Caress JB, Abend WK, Preston DC, Logigian EL. A case of
non-Hodgkin’s
lymphoma
CRMP-52007;78:651–652.
autoantibody. Mov Dis54.ord
Tan2003;18:1156–1158.
JH, Goh BC, Tambyah PA, Wilder-Smith E. Paraneoplastic
Hodgkins
producing
neuromyotonia.
67. Essalmi
L, lymphoma
Meaux-Ruault
N, Hafsaoui
C, Gil Neurology
H, Curlier1997;
E,
progressive
supranuclear
palsyBaccon
in a patient
with
cell lym49:258–259.
49. Sansing
LH, Tuzun
E, Ko MW,
J, Lynch
DR,BDalmau
J.
Dupond
JL. Stiff person syndrome with thymoma. Efficacy of
Relatassociated
Disord 2005;11:187–191.
74.thymectomy.
Zifko U, Drlcek
U, Machacek
E, et al. Syndrome of continuous
Aphoma.
patient Parkinsonism
with encephalitis
with NMDA receptor antiRev Med
Interne 2007;28:627–630.
55.bodies.
Fahn S,Nat
Brin
MF,
Dwork
AJ,2007;3:291–296.
Weiner WJ, Goetz CG, Rajput AH.
muscle C,
fiber
activity
and plasmacytoma
withKV,
IgMNaumann
paraproteineClin
Pract
Neurol
68. Wessig
Klein
R, Schneider
MF, Toyka
M,
Case 1,D,1996:
rapidly
progressive
Parkinsonism,
incontinence,
mia. Neurology
1994;44:560–561.
50. Croteau
Owainati
A, Dalmau
J, Rogers
LR. Response
to canSommer
C. Neuropathology
and binding studies in anti-amphiphyimpotency,
anda levodopa-induced
moaning in achoreiform
patient with
mul75.sin
Hart
IK, Waters
C, Vincent
A, et Neurology
al. Autoantibodies
detected to
cer
therapy in
patient with a paraneoplastic
disorassociated
stiff person
syndrome.
2003;61:195–198.
tipleNeurology
myeloma.2001;57:719–722.
Mov Disord 1996;11:298–310.
expressed potassium
channels are
implicated
in neuromyotonia.
der.
69. Newsom-Davis
J. Neuromyotonia.
Rev
Neurol 2004;160:S85–S89.
56.Dalmau
Golbe LI,
MillerF,DC,
Duvoisin
RC.al.Paraneoplastic
degeneration
Ann Neurol
1997;41:238–246.
51.
J, Graus
Villarejo
A, et
Clinical analysis
of anti70. Gutmann
L, Gutmann
L. Myokymia and Neuromyotonia. J Neuof the substantia
nigra with Brain
dystonia
and Parkinsonism. Mov Dis76.rol
ToepferM,
Schroeder M, Unger JM, Lochmüller H, Pongratz D,
Ma2-associated
encephalitis.
2004;127:1831–1844.
2004;251:138–142.
ord 1989;4:147–152.
Müller-Felber
W. Neuromyotonia,
myoclonus,
neuropa52. Matsumoto
L, Yamamoto T, Higashihara M, et al. Severe hypo71. Hart
IK, Maddison
P, Newsom-Davis
J, et al. sensory
Autoantibodies
57.kinesia
Schluter
E, Domm
S, Erdag
S. A case
of rapidly
thyand cerebellar
symptoms
in achannels
patient with
antibodies to
caused
by anti-Ma2
encephalitis
associated
withprogressive
bilateral
detected
to expressed
potassium
are implicated
in neuroneumultiple system
findings
and 2007;
pathonal neucleoprotein
antibodies
(anti-Hu). Clin Neurol Neurosurg
intratubular
germ degeneration:
cell neoplasm morphological
of the testes. Mov
Disord
romyotonia.
Ann Neurol
1997;41:238–246.
genic implications. Acta Neuropathol 2002;103:395–300.
1999;101:207–209.
22:728–731.
72. Hart
IK, Maddison P, Newsom-Davis J, Vincent A, Mills KR.
58.Pruss
Josephs
KA, Ishizawa
Y, Cookson
N, Dickson
DW. A
77.Phenotypic
Alessi G, De
ReuckofJ,peripheral
De Bleeker
J, Vancayzeele
S. Successful
53.
H, Voltz
R, Flath T,
B, Tsuboi
et al. Anti-Ta
associated
paraneoplasvariants
nerve
hyperexcitability.
Brain
study testicular
of vascular
progressive
supranuclear
immunoglobulin treatment in a patient with neuromyotonia. Clin
ticclinicopathological
encephalitis with occult
intratubular
germ
cell neo2002;125;1887–1895.
palsy:JaNeurol
multi-infarct
disorder
presenting
as progressive supranuNeurolJB,
Neurosurg
plasia.
Neurosurg
Psychiatry
2007;78:651–652.
73. Caress
Abend 2000;102;173–175.
WK, Preston DC, Logigian EL. A case of
clear
Neurol 2002;59:1597–1601.
78.Hodgkins
Tormoehlen
LM, Pascuzzi
Thymoma, myasthenia
gravis
54. Tan
JH,palsy.
Goh Arch
BC, Tambyah
PA, Wilder-Smith E. Paraneoplastic
lymphoma
producingRM.
neuromyotonia.
Neurology 1997;
59.progressive
Meinck HM,
Thompsonpalsy
PD. Stiff
syndrome
and other paraneoplastic syndromes. Haematol Oncol Clin North
supranuclear
in a man
patient
with B and
cell related
lym49:258–259.
conditions.
Mov Disord
2002;17:853–866.
Am 2008;22:509–526.
phoma.
Parkinsonism
Relat
Disord 2005;11:187–191.
74. Zifko
U, Drlcek U, Machacek E, et al. Syndrome of continuous
60.Fahn
McHugh
JC,MF,
Murray
B,AJ,
Renganathan
Connolly
S, Lynch
79.muscle
Blumberg
Port JL,and
Weksler
B, et al. Thymoma:
a multivariate
55.
S, Brin
Dwork
Weiner WJ,R,Goetz
CG, Rajput
AH.T.
fiberD,activity
plasmacytoma
with IgM paraproteineGAD1,antibody
positiveprogressive
stiff personParkinsonism,
syndrome in incontinence,
a patient with
analysis
of factors
predicting survival. Ann Thorac Surg 1995;60:
Case
1996: rapidly
mia.
Neurology
1994;44:560–561.
renal cell carcinoma.
Mov Disordmoaning
2007;22:1343–1346.
908–913.
impotency,
and levodopa-induced
in a patient with mul75. Hart
IK, Waters C, Vincent A, et al. Autoantibodies detected to
tiple myeloma. Mov Disord 1996;11:298–310.
expressed potassium channels are implicated in neuromyotonia.
56. Golbe LI, Miller DC, Duvoisin RC. Paraneoplastic degeneration
Ann Neurol 1997;41:238–246.
of the substantia nigra with dystonia and Parkinsonism. Mov Dis76. ToepferM, Schroeder M, Unger JM, Lochmüller H, Pongratz D,
ord 1989;4:147–152.
Müller-Felber W. Neuromyotonia, myoclonus, sensory neuropa57. Schluter E, Domm S, Erdag S. A case of rapidly progressive
thyand cerebellar symptoms in a patient with antibodies to neuromultiple system degeneration: morphological findings and pathonal neucleoprotein antibodies (anti-Hu). Clin Neurol Neurosurg
genic implications. Acta Neuropathol 2002;103:395–300.
1999;101:207–209.
58. Josephs KA, Ishizawa T, Tsuboi Y, Cookson N, Dickson DW. A
77. Alessi G, De Reuck J, De Bleeker J, Vancayzeele S. Successful
clinicopathological study of vascular progressive supranuclear
immunoglobulin treatment in a patient with neuromyotonia. Clin
palsy: a multi-infarct disorder presenting as progressive supranuNeurol Neurosurg 2000;102;173–175.
clear palsy. Arch Neurol 2002;59:1597–1601.
78. Tormoehlen LM, Pascuzzi RM. Thymoma, myasthenia gravis
59. Meinck HM, Thompson PD. Stiff man syndrome and related
and other paraneoplastic syndromes. Haematol Oncol Clin North
conditions. Mov Disord 2002;17:853–866.
Am 2008;22:509–526.
60. McHugh JC, Murray B, Renganathan R, Connolly S, Lynch T.
79. Blumberg D, Port JL, Weksler B, et al. Thymoma: a multivariate
romyotonia. Ann
72. Hart IK, Maddiso
Phenotypic varian
2002;125;1887–18
73. Caress JB, Aben
Hodgkins lympho
49:258–259.
74. Zifko U, Drlcek
muscle fiber activ
mia. Neurology 1
75. Hart IK, Waters
expressed potassi
Ann Neurol 1997
76. ToepferM, Schroe
Müller-Felber W.
thyand cerebellar
nal neucleoprotei
1999;101:207–209
77. Alessi G, De Reu
immunoglobulin t
Neurol Neurosurg
78. Tormoehlen LM,
and other paraneo
Am 2008;22:509–
79. Blumberg D, Port
analysis of factors
908–913.
セロトニンとパーキンソン病:
運動機能,気分,精神疾患との関連
Serotonin and Parkinson’s Disease: On Movement, Mood, and Madness
*
Susan H. Fox, MRCP, PhD, Rosalind Chuang, MD, and Jonathan M. Brotchie, PhD
*
Movement Disorders Clinic, McL 7–421, University of Toronto, Toronto Western Hospital, Toronto, Ontario, Canada
近年,パーキンソン病(Parkinson’
s disease; PD)に
することや,他の神経伝達物質系(ドパミン,GABA,
おいてセロトニン(5-hydroxytryptamine; 5-HT)が果
グルタミン酸など)の調節に果たす 5-HT の潜在的機能
たしうる多面的役割に対する理解が深まってきた。PD
への理解が深まったことで,PD の運動症状と非運動症
に関する初期の病理学的研究では,脳組織における
状への効果が期待できるセロトニン作動薬の開発に大き
5-HT の非選択的な減少が証明されたが,ジスキネジア
な力が注がれるようになった。ただし,未解決の問題も
や気分障害などの併存疾患との相互関係についてはほ
いくつか残されている。今後は,5-HT 神経伝達の変化
とんど明らかにされなかった。また,セロトニン作動薬
とあらゆる臨床症状との相互関係に焦点を当て,病理学
による治療はレボドパ(L—ドパ)に比べて有効性が低い
的ならびに in vivo イメージングの両面から研究する必
との知見もあり,最近までこの分野はほとんど無視され
要がある。
てきた。脳内には 5-HT 受容体サブタイプが多数存在
Movement Disorders Vol. 24, No. 9, 2009, pp. 1255–1266
SEROTONIN AND PARKINSON’S DISEASE
1257
Key Word パーキンソン病,セロトニン,5-HT,ジスキネジア,抑うつ,不安,精神病,便秘
Table
1 臨床で利用可能なドパミン受容体アゴニストの
受容体に対する相対的親和性
TABLE
1. Relative affinity of clinically available dopamine 5-HT
receptor
agonists for 5-HT receptors
Dopamine agonist
Non ergoline
Ergoline
Ropinirole
Pramipexole
Apomorphine
Cabergoline
Pergolide
Bromocriptine
Lisuride
5-HT1A
5-HT1B
5-HT1D
5-HT2A
5-HT2B
5-HT2C
1
1
1
1
11
11
111
0/1
0/1
1
1
1
1
1
1
1
1
11
1
11
111
0/1
0/1
1
11
1
1
11
0/1
0/1
1
11
11
1
22
0/1
0/1
1
1
1
1
11
1 5 agonist; 2 5 antagonist; 0 5 no activity;
0/1 5 low +=低活性,+~++++=+が多いほど効力が高い(Reference
activity;
1 toET
1111
1258
S.H.
FOX
AL. 5 increased potency (adapted from ref. 31). 31 より引用)
+=アゴニスト,-=アンタゴニスト,0
=活性なし,0/
Table 2 PD の運動症状とレボドパ誘発性ジスキネジアに関するセロトニン作動薬の評価
TABLE
2. Serotonergic
drugs evaluated for motor symptoms and levodopa-induced dyskinesia in PD
tive affinity for 5-HT1A receptors31 (Table 1). To date,
5-HT Drugs in the Treatment of
Effective on
the most well-defined clinical effect relatedEffective
to thison5levodopa-induced Parkinsonian Tremor
action
of
HT binding property
the 5-HT2B-agonist
Drug
5-HTissubtype
PD motor
symptoms
dyskinesia
One
motor feature of PD that Comments
may be mediated in
some
ergoline
DAs
that
has
been
linked
to
the
potenpart
Clinical
observations
Reduces PD tremor
Yesby 5-HT is tremor.
Mirtazapine
also binds
to non 5-HTsuggest
Mirtazapine
5-HT1A agonist; 5-HT2,
tially serious but5-HT
rare
problem of restrictive cardiac
receptors including
acetylcholine and
3 antagonist
tremor
in
PD
is
less
responsive
to
dopaminergic
drugs
noradrenaline
valulopathy.32,33 Lisuride is a 5-HT2B antagonist and,
than
rigidity
and
bradykinesia.
A
PET
study
in
Reduces tremor; no34
Yes
Practical issues with regulatory monitoring
Clozapine
5-HT2A/2C receptor
as such, has not been
reported to cause this
problem.
advanced patients with PD showed a 27% reduction in
antagonist
worsening
of PD
5-HT2B receptors
and mg) midbrain
receptor on cardiac
At lowvalves,
doses (25–50
No
No studies
have been preformed using
Quetiapine
5-HTare
2A/2C located
raphe 5-HT
1A binding potential compared
35 seen
adverse effects
higher doses of quetiapine (>50mg/d)
their stimulationantagonist
results in fibroblast no
mitogenesis.
with
healthy controls,
a trial
change
that correlated
with
No worsening
Possible
Single
in 10 patients
with PD
Buspirone
5-HT1A agonist
48
Pleuropulmonary
and
retroperitoneal fibrosis
also
Early
tremor
but not withSarizotan
bradykinesia
or rigidity.
Potential have
to worsen
Non significant
also has dopamine
D2 antagonist
Sarizotan
5-HT
1A agonist
and possibly
been reported to be caused by 5-HT2B,parkinsonism
binding.
Largewas
placebo
loss compared
of 5-HTtotransporter
binding
alsoeffect
noted in the
placebo
(development has now stopped)
5-HT2A, receptor binding activity.36,37
thalamus
in
drug
naı̈ve
patients
with
PD
with
tremor
Unknown
Possible
Preliminary reports to date; on
going
study
Pimavanserin
5-HT2A inverse agonist
Clinical experience
would suggest that ergoline
compared with those without; however, after 17
DAs, particularly lisuride, induce more psychiatric
months follow-up, this difference was not significant.49
side-effects than nonergoline DAs, although this has
Mirtazapine, an antidepressant with multiple mechanot untreated
been shown
in randomized
clinical
trialsof(RCTs).
the
MPTP-lesioned
primate
model
PD, 5in
serotonin-rich
than5-HT
in dopamine-rich
5-HT2
nisms
of actions, grafts
including
1A agonist andgrafts—
Such
findings may be related to greater 5-HT 54
binding
PostHT
an
correlated
with the
dopaminerandeffect
5-HTthat
actions,
candegree
reduceofparkinsonian
1A receptors are upregulated in the putamen.
3 antagonist
64
50
of
ergoline
versus
nonergoline
(Table
1). either
Howmortem
studies
in patients
with DAs
PD have
shown
gic
degeneration.
(Table 2). In addition, the atypical antipsytremors
55studies have reported impulse control disorever,
some
Otherclozapine,
potential which
areas binds
whereto5-HT
agonists
may
no change or increased 5-HT1A receptors in the neoreceptors,
chotic
5-HT
1A2A/2C
ders, incompared
particularwith
pathological
gambling,
in 56patients
Thus,
receptor
cortex
age-matched
controls.
reduce
LID include
postsynaptic
5-HT1A
The mechanism
of action
or
also
suppresses
tremor.51
27
進行性核上性麻痺における小脳病変:臨床病理学的研究
Cerebellar Involvement in Progressive Supranuclear Palsy: A Clinicopathological Study
*
Masato Kanazawa, MD, Takayoshi Shimohata, MD, PhD, Yasuko Toyoshima, MD, PhD, Mari Tada, MD, Akiyoshi Kakita, MD, PhD, Takashi
Morita, MD, PhD, Tetsutaro Ozawa, MD, PhD, Hitoshi Takahashi, MD, PhD, and Masatoyo Nishizawa, MD, PhD
*
Department of Neurology, Brain Research Institute, Niigata University, Niigata, Japan
進行性核上性麻痺(progressive supranuclear palsy;
質徴候を呈する残りの 4 例は,分類不能 PSP と判断さ
PSP)の多様な臨床型についてはこれまでも議論がなさ
れた。このうち,3 例は小脳性運動失調症が初発および
れ, 現 在 は, 古 典 的 な Richardson 症 候 群
主要症状であった。特記すべき点として,プルキンエ細
(Richardson’
s syndrome; RS)と PSP- パーキンソニ
胞のタウ陽性封入体は,小脳性運動失調症のない患者
ズム(progressive supranuclear palsy-Parkinsonism;
よりも,小脳性運動失調症のある患者で観察される頻度
PSP-P)に分類されている。本研究では,PSP の臨床
が有意に高かった。小脳性運動失調症のあるすべての
病理学的な多様性を検討するため,病理学的に証明さ
患者は,小脳性運動失調症のない患者に比べ,グリオー
れた連続 22 例の日本人 PSP 患者をレトロスペクティ
シスを伴う神経細胞脱落が多く,小脳歯状核内のコイル
ブに解析した。臨床像は疾患経過の初期段階と経過中
体(coiled body)の密度も高かった。本研究により,
の任意の時点で検討した。グリオーシスを伴う神経細胞
日本人患者を対象として,PSP の幅広い臨床病理学的
脱落とタウ病変の病理学的重症度も評価した。臨床像
所見を明示した。小脳性運動失調症は PSP 診断の除外
に 基 づ き,10 例 の 患 者 は RS に 分 類 さ れ,8 例 は
基準の一つに含まれているが,本研究により,PSP 患
PSP-P に分類された。小脳性運動失調症または大脳皮
者は小脳性運動失調症を呈することが実証された。
Movement Disorders Vol. 24, No. 9, 2009, pp. 1312–1318
Key Word 進行性核上性麻痺,脊髄小脳失調症,パーキンソン病,パーキンソン性障害
PSP: A DISTINCT PHENOTYPE WITH CEREBELLAR ATAXIA
1315
2 発症から
年以内の
PSPwithin
患者の臨床像
TABLE 2.Table
Clinical
features of2 PSP
patients
2 yr of disease onset
Clinical feature
RS
PSP-P
Unclassifiable PSP
Number
Male(%)
Age at onset (yr)
Age at death (yr)
Disease duration (yr)
Supranuclear vertical gaze palsy
Gait disturbance
Falls
Postural instability
Cognitive decline
Asymmetric onset
L-dopa responsiveness
Tremor
Cerebellar ataxia
Cerebral cortical signs
10
80.0
69.3 6 8.0
74.4 6 8.4
5.2 6 2.3a
6/10 (60.0%)
9/10 (90.0%)
10/10 (100%)
6/9 (66.7%)
5/9 (55.6%)
1/10 (10.0%)
0/5 (0%)
0/10 (0%)
0/10 (0%)
0/10 (0%)
8
50.0
64.0 6 9.4
74.9 6 9.9
10.8 6 2.6
1/6 (25.0%)
7/7 (100%)
2/7 (28.6%)
1/6 (16.7%)
1/8 (12.5%)
6/8 (75.0%)
5/6 (83.3%)
5/8 (62.5%)
0/6 (0%)
0/8 (0%)
4
75.0
69.0 6 4.2
73.8 6 3.6
4.8 6 1.0a
2/4 (50.0%)
3/4 (75.0%)
3/4 (75.0%)
2/4 (50.0%)
1/4 (25.0%)
2/4 (50.0%)
NA
0/4 (0%)
3/4 (75.0%)
2/4 (50.0%)
a aP < 0.01 vs. patients with PSP-P. RS, Richardson’s syndrome; PSP-P, progressive supranuclear palsyPSP-P 患者との比較で p < 0.01。RS = Richardson 症候群,PSP-P =進行性核上性麻痺 - パーキンソニ
parkinsonism; NA, not administered.
ズム,NA =投与せず
28
pathological severities of the cerebellar dentate nucleus
and cerebellar cortex between 3 patients with cerebellar ataxia (Patients 1–3) and the remaining patients
without cerebellar ataxia. The disease durations for the
patients with and without cerebellar ataxia were 4.3 6
0.6 years and 7.6 6 3.7 years, respectively (P 5
0.14). All 3 patients with cerebellar ataxia revealed
more severe neuronal loss with gliosis (Fig. 1A, Table
4) and higher densities of CBs (Fig. 1B, Table 4) in
PSP-P patients. Two of the 3 patients with cerebellar
ataxia showed a small number of TAs, while 3 of the
19 patients without cerebellar ataxia showed mild pathology of TAs in the cerebellar dentate nucleus (P 5
0.12). In the cerebellar sections of patients with cerebellar ataxia, we found granular immuno-reactivity for
AT8 antibody in the cytoplasm of a small proportion
of the Purkinje cells (Fig. 1C,D). By Gallyas–Braak
silver staining, we confirmed argyrophilic profiles (Fig.
parkinsonism; NA, not administered.
pathological severities of the cerebellar dentate nucleus
and cerebellar cortex between 3 patients with cerebelM. KANAZAWA
ET AL.
lar ataxia (Patients
1–3) and the
remaining patients
without cerebellar ataxia. The disease durations for the
patients with and without cerebellar ataxia were 4.3 6
0.6 years and 7.6 6 3.7 years, respectively (P 5
0.14). All 3 patients with cerebellar ataxia revealed
more severe neuronal loss with gliosis (Fig. 1A, Table
4) and higher densities of CBs (Fig. 1B, Table 4) in
the cerebellar dentate nucleus compared with RS and
PSP-P patients. Two of the 3 patients with cerebellar
ataxia showed a small number of TAs, while 3 of the
19 patients without cerebellar ataxia showed mild pathology of TAs in the cerebellar dentate nucleus (P 5
Abstract
0.12). In the cerebellar sections of patients with
cerebellar ataxia, we found granular immuno-reactivity for
AT8 antibody in the cytoplasm of a small proportion
of the Purkinje cells (Fig. 1C,D). By Gallyas–Braak
silver staining, we confirmed argyrophilic profiles (Fig.
1E), with variable intensity, of the tau-labeled granular
TABLE
3. Clinical
of patients
with unclassifiable PSP within 2 yr of disease onset
Table
3 分類不能
PSPfeatures
患者の発症
2 年以内および疾患経過中の任意の時点における臨床像
and at any time during the disease course
Patient
1
2
3
4
First 2 yr
Sex
F
M
M
Age at onset (yr)
64
72
73
Supranuclear vertical gaze palsy
2
1
1
Gait disturbance
1
1
1
Falls
1
1
1
Postural instability
1
1
2
Cognitive decline
2
2
1
Asymmetric onset
1
2
1
L-dopa responsiveness
NA
NA
NA
Tremor
2
2
2
Cerebellar ataxia
T>L
T<L
T>L
Cerebral cortical signs
2
2
1
Entirenucleus
disease(A,
course
1.
Histopathological features of the cerebellar dentate
B) and cortex (C–E) of PSP patients with cerebellar ataxia. Neuronal
Disease
durationimage
(yr) of a tau-immunostained 5section showing two
4 labeled Purkinje4
nd gliosis (A), and scattered coiled bodies (B) are seen.
Low-power
Supranuclear
vertical gaze granular,
palsy
1 (D), and argyrophilic
1 (E) profiles in1
C: arrows). High-power magnifications of Purkinje cells
(arrows) demonstrating
tau-positive
Gait disturbance
1 100 lm in A and
1 B, 500 lm in C,1
toplasm. A: hematoxylin–eosin stain; B–D: AT8 immunostain;
E: Gallyas–Braak silver stain. Bars 5
Falls issue, which is available at www.interscience.wiley.com.]
1
1
1
5 lm in D and E. [Color figure can be viewed in the online
Postural instability
1
1
1
decline
1
2
1
sions. The Purkinje cells with the inclusionsCognitive
were
gorized
as
having
PSP-P.
These
patients
showed
no
L-dopa responsiveness
NA
NA
NA
nk. Interestingly, we saw such inclusions inTremor
all 3
gender differences and 2
a long disease2duration com-2
Cerebellar ataxiapared with the RS patients,
T 5 L which is
T<
L
T>L
nts with cerebellar ataxia, whereas we encounconsistent
with
Cerebral cortical signs
2
23
1
only 5 out of the 19 patients without cerebellar
the findings reported in a previous study. It was difficult=男性,F
toM,differentiate
theseT, patients
from
the ataxia.
patients
a (P 5 0.036).
NA,
not administrated;
male;
and F, female;
truncal ataxia;
L, limb
NA
=投与せず,M
=女性,T
=体幹運動失調症,L
=四肢運動失調症
with PD early in the disease course, although we could
e finally compared the pathological severities of
eventually differentiate them because the PSP-P
recentral gyrus between the 2 patients with cerebral
patients also developed supranuclear vertical gaze
cal signs and 19 patients without them. The disease
palsy several years after the disease onset, which is
ion for the patients with cerebral cortical signs was
consistent with previous descriptions.5 Supranuclear
6 1.4 years, vs. 7.4 6 3.7 years for the patients
out cerebral cortical signs (P 5 0.38). Both patients
cerebral cortical signs revealed superficial spongiond moderate neuronal loss with gliosis (P 5 0.071),
Table
4 4.RSCerebellar
患者,PSP-P
患者,小脳性運動失調症を
TABLE
dentate
nucleus in RS, PSP-P, and
higher densities of CBs (P 5 0.071) in the precen伴う
PSP 患者の小脳歯状核
PSP
patients
with cerebellar ataxia
gyrus, whereas only 4 of 19 patients without cereSevere
Moderate
Mild
Absent
cortical signs revealed such severe pathology (Fig.
Neuronal loss with gliosis
B). We also evaluated the density of TAs in the preRS
(N 5 10)
3
6
1
0
al gyrus and found that both patients with cerebral
PSP-P
(N 5 8)
4
2
2
0
cal signs had very high TA density, whereas 7 of
PSP-Cbll
(N 5 3)
3
0
0
0
Densities of coiled bodies
9 patients without cerebral cortical signs had very
RS
(N 5 10)
0
1
4
5
TA density (P 5 0.17).
DISCUSSION
Clinicopathological Features of PSP-P
ur study demonstrates that approximately one–third
e PSP patients in our Japanese cohort were cate-
PSP-P
PSP-Cbll
(N 5 8)
(N 5 3)
0
1
0
1
3
1
M
67
2
2
2
2
2
2
NA
2
2
1
6
1
2
1
2
2
NA
2
2
1
Movement Disorders, Vol. 24, No. 9, 2009
5
0
The differences in pathological severities of neuronal loss with
RS 患者,PSP-P 患者,小脳性運動失調症を伴う PSP 患者におけ
gliosis and densities of coiled bodies evaluated using the semiquantiるグリオーシスを伴う神経細胞脱落とコイル体(coiled
tative four-point scale among RS, PSP-P, and PSP patientsbody)の密
with cerebellar ataxia are shown.
度による病理学的重症度の差を,4
段階の半定量的尺度を用いて評
PSP-Cbll, PSP patients with cerebellar ataxia.
価した。
PSP-Cbll =小脳性運動失調症を伴う PSP 患者
ent Disorders, Vol. 24, No. 9, 2009
29
パーキンソン病患者の衝動性障害・強迫性障害に関する
質問票の妥当性検討
Validation of the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease
*, **, ***, ****
Daniel Weintraub, MD, Staci Hoops, BA, Judy A. Shea, PhD, Kelly E. Lyons, PhD, Rajesh Pahwa, MD, Erika D. Driver-Dunckley,
MD, Charles H. Adler, MD, PhD, Marc N. Potenza, MD, PhD, Janis Miyasaki, MD, MEd, FRCPC, Andrew D. Siderowf, MD, MSCE, John E.
Duda, MD, Howard I. Hurtig, MD, Amy Colcher, MD, Stacy S. Horn, DO, Matthew B. Stern, MD, and Valerie Voon, MD
*
Department of Psychiatry, University of Pennsylvania, Philadelphia, Pennsylvania, USA
Department of Neurology, University of Pennsylvania, Philadelphia, Pennsylvania, USA
***
Parkinson’s Disease Research, Education and Clinical Center (PADRECC), Philadelphia Veterans Affairs Medical Center, Philadelphia, Pennsylvania, USA
****
Mental Illness Research, Education and Clinical Center (MIRECC), Philadelphia Veterans Affairs Medical Center, Philadelphia, Pennsylvania,
USA
**
現在のところ,パーキンソン病(Parkinson’
s disease;
障害または行動の各項目で高かった〔受信者動作特性曲
PD)患者の衝動制御障害(impulse control disorder;
線下面積(receiver operating characteristic area
ICD)に関する包括的な評価法は存在しない。本研究の
under the curve; ROC AUC)
:賭博= 0.95,性行動=
目的は,PD 患者の ICD およびその他の強迫行動に関す
0.97,買い物= 0.87,摂食= 0.88,punding = 0.78,
る自己記入式スクリーニング用質問票をデザインし,そ
趣味への耽溺= 0.93,徘徊= 0.79〕
。事後解析の結果,
の精神測定特性を評価することである。Questionnaire
QUIP-S の ICD セクションでも同様の特性が認められた
for Impulsive-Compulsive Disorders in Parkinson’
s
(ROC AUC:賭博= 0.95,性行動= 0.96,買い物=
Disease(QUIP)は次の 3 つのセクションで構成される。
0.87,
摂食= 0.88)
。障害/行動を複合的に検討すると,
セクション 1 では 4 つの ICD(賭博,性行動,買い物,
何らかの障害を伴う患者を検出する QUIP と QUIP-S の
摂食)
,セクション 2 ではその他の強迫行動(punding,
感度はそれぞれ 96%および 94%であった。QUIP のス
趣味への耽溺,徘徊)
,セクション 3 では医薬品の強迫
コアは,PD 患者に生じる様々な ICD およびその他の強
的使用について評価する。本質問票の妥当性を検討
迫行動の自己評価式スクリーニング手段として妥当であ
す る た め,4 つ の 運 動 障 害 セ ン タ ー で 便 宜 的 標 本
り,簡易版も完全版と同様の高い効果をもつと考えられ
(convenience sample)の PD 患者 157 例に QUIP に
る。スクリーニング結果が陽性であれば,続いて包括的
回答してもらい,その後,研修を受け QUIP の結果を知
な臨床面接を行い,症状の範囲と重症度,臨床管理の必
らされていない評価担当者が診断面接を行った。次いで
要性を判定すべきである。
同質問票 の 簡 易版(shortened version of QUIP;
※
※
QUIP-S)
についても検討した。QUIP の弁別的妥当性は,
日本語版注釈:研究者の利便性を図るために無作為化を行わ
ず,アクセス可能な対象者から構成された標本。
Movement Disorders Vol. 24, No. 10, 2009, pp. 1461–1467
Key Word パーキンソン病,衝動制御障害,ドパミン調節異常症候群(dopamine dysregulation syndrome),
punding,病的賭博
30
5%), and 3.2% of the population having both pundSimilarly, as some patients were diagnosed with
and hobbyism.
more than one ICD or other compulsive behavior but
he median completion time for the QUIP was 5
did not endorse questions on the QUIP for each diagutes.
nosed disorder or behavior, we assessed the validity of
a positive response for any ICD or other compulsive
uestionnaire for Impulsive-Compulsive Disorders
Abstract
behavior (using the aforementioned cutoff points) to
in Parkinson’s Disease
identify
an
individual
with
any
‡1
ICD
or
other
compul1464
D. WEINTRAUB ET AL.
D Section
sive behavior (compulsive medication use excepted).
This2 analysis
had
AUC 5 0.85 (sensitivity 5 0.96,
he optimal cutoff point (i.e., point of maximum Table
QUIP ICD
セクションの障害別の妥当性検討
TABLE
2. Validation
ofPPV
the QUIP
ICD
section
specificity
5
0.73,
5 0.62,
and
NPVby5disorder
0.98).
mbined sensitivity and specificity) for each ICD
Cutoff pointsa
: (1) gambling: affirmative answers to ‡2 questions;
Shortened
Version of the QUIP
sexual behavior: ‡1 questions; (3) buying: Gambling
‡1 ques-(N 5 11)
Sex (N 5 14)
Buying (N 5 10)
Eating (N 5 7)
s; and (4) eating: ‡2 questions (Table 2). These
1
2
3
4 Item
5 Selection
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
off points provided at least 80% sensitivity and
91
91
82
64
46 evaluate
100
86a shortened
71
50 version
43
80of the
60 ICD
40 section,
30
30
86
86
57
43
29
To
cificity for each ICD. Sensitivity
Specificity
94
97
99
99 we
100started
89 with
93 the98introductory
98
99 question
89
97 for99each
99ICD100
83
89
94
98
99
PPV
53
71
90
88
100
47
55
77
70
86
33
55
67
75
100
19
26
31
50
67
her Compulsive Behaviors
NPV Sections 99
99
99
97 and
96added
100 questions
99
97 only
95 if they
95 increased
98
97 the
96 sensitiv95
95
99
99
98
97
97
AUC (95% CI)
0.95 (0.85–1.05) ity of the instrument.
0.97 (0.95–1.00)
0.87 (0.72–1.02)
0.88 (0.72–1.04)
As a result, the abbreviated
ICD
or other compulsive behaviors,
each introductory
section has two questions for each disorder (8 total
a aFive
stion by itself provided
optimal
sensitivity
and
questions
per ICD.
各 ICD
につき質問は
5 項目。
questions;
Table
Thearea
optimal
cutoff
PPV,
positive
predictive
value;
NPV,
negative
predictive
value;4).
AUC,
under the
curve. point for each
cificity (Table 3). The discriminant
validity of
the
PPV =陽性適中率,NPV
=陰性適中率,AUC
=曲線下面積
ICD
was
‡1
affirmative
answer
to
any
question, which
gle question for hobbyism was similar to that for
led
to
similar
AUCs,
sensitivities,
and
as
(11.5%),
and
3.2%
of
the
population
having
both
pundSimilarly, specificities
as some patients
were diagnosed with
ICD section (sensitivity 5 0.96, specificity 5
the
full
ICD
section.
ing
and
hobbyism.
more
than
one
ICD
or
other
compulsive behavior but
0), while the questions for punding and walkabout
QUIP-S,
created
onquestions
the results
median
completion time forThe
the complete
QUIP was
5
did not based
endorse
on the QUIP for each diagsimilarly high specificity The
but lower
sensitivity.
mentioned
earlier,
consists
of
two
questions
for
each
of
minutes.
nosed
disorder
or
behavior,
we assessed the validity of
Affirmative answers to the compulsive medication use
the
four
ICDs,
the
three
introductory
questions
for
a
positive
response
for
any
ICD or other compulsive
stions were uncommon, ranging
from 0 tofor6.4%.
The
Questionnaire
Impulsive-Compulsive
Disorders
other
compulsive
behaviors,
and
the
two
questions
for
behavior
(using
the
aforementioned
cutoff points) to
patient who met criteria for compulsiveinmedication
Parkinson’s Disease
identify
an
individual
with
any
‡1
ICD
or other compulendorsed both the introductory question and the
Table3.3 その他の強迫行動の妥当性検討
TABLE
Validation
of
other
compulsive
behaviors
ICD
Section
sive
behavior
(compulsive
medication
use excepted).
st commonly-endorsed of the other four questions.
This
analysis
had
AUC
5
0.85
(sensitivity
5 0.96,
The optimal cutoff point (i.e., point of maximum
Introductory questions
specificity
5
0.73,
PPV
5
0.62,
and
NPV
5
0.98).
combined sensitivity and specificity) for each Hobbyism
ICD
mbining Disorders/Behaviors
Punding
Walkabout
was:
(1)
gambling:
affirmative
answers
to
‡2
questions;
(N 5 23)
(N 5 16)
(N 5 5)
As some patients were diagnosed with more than one
Shortened
Version of the QUIP
(2)
sexual
behavior:
‡1
questions;
(3)
buying:
‡1
quesD but did not endorse questions on the QUIP for all
Sensitivity
96
63
60
tions;
(4) of
eating:
‡2 questions
(Table 2). These
Specificity
90
93
97
gnosed ICDs, we assessed
the and
validity
a positive
Item Selection
PPV
61
50
43
cutoff
points
provided
at
least
80%
sensitivity
and
ponse for any ICD (using the aforementioned cutoff
NPV
99
96
99
To
evaluate
a
shortened
version of the ICD section,
specificity
nts) to identify an individual
withfor
anyeach
‡1 ICD.
ICD (as
AUC (95% CI)
0.93
0.78
0.79
we
started
with
the
introductory
question for each ICD
(0.87–0.98)
(0.63–0.92)
(0.52–1.05)
osed to examining each individual ICD). This analyand added questions only if they increased the sensitivOther
Compulsive
Behaviors
Sections
had AUC 5 0.88 (sensitivity 5 0.97, specificity 5
PPV,
positive predictive value;
negative
predictiveAs
value;
PPV =陽性適中率,NPV
=陰性適中率,AUC
=曲線下面積
ityNPV,
of the
instrument.
a result, the abbreviated ICD
For0.99).
other compulsive behaviors,
each
introductory
AUC,
area under
the curve.
9, PPV 5 0.53, and NPV 5
section
has
two
questions
for each disorder (8 total
question by itself provided optimal sensitivity and
questions;
Table
4).
The
optimal
cutoff point for each
specificity (Table 3). The discriminant validity of the
ICD
was
‡1
affirmative
answer
to
any question, which
single question for hobbyism was similar to that for
ment Disorders, Vol. 24, No. 10, 2009
led
to
similar
AUCs,
sensitivities,
and specificities as
the ICD section (sensitivity 5 0.96, specificity 5
the
full
ICD
section.
0.90), while the questions for punding and walkabout
The complete QUIP-S, created based on the results
had similarly high specificity but lower sensitivity.
ICD
QUESTIONNAIRE
FOR
PARKINSON’S
DISEASE
1465
mentioned
earlier,
consists of two questions for each
of
Affirmative answers to the compulsive medication use
the
four
ICDs,
the
three
introductory
questions
for
questions were uncommon, ranging from 0 to 6.4%. The
other compulsive behaviors, and the two questions for
Table
4 QUIP-S
ICD セクションの障害別の妥当性検討
sole patient who met criteria for
compulsive
medication
TABLE 4. Validation of QUIP-S ICD section by disorder
use endorsed both the introductory question and the
most commonly-endorsed of the other four questions.
Gamblingb
(N 5 11)
a
Cutoff
points
TABLE
3. Validation of other compulsive behaviors
Sexc (N 5 14)
Introductory questions e
Buyingd (N 5 10)
Eating (N 5 7)
Combining Disorders/Behaviors
Hobbyism
Punding
Walkabout
2
2
1 (N 5 23)
2 (N 5 16) 1
(N 5 5) 2
As some patients were1 diagnosed with
more than1 one
Sensitivity
91
73
100
64
80
40
86
ICD but did not endorse questions on the QUIP for all
Sensitivity
96
63
60 43
Specificity
95
99
90
96
91
99
85
Specificity
90
93
97 96
diagnosed ICDs, we assessed
the validity
of a positive
PPV
59
89
48
60
38
80
21
PPV
61
50
43 40
response for any ICD (using
the aforementioned
cutoff
NPV
99
98
100
96
99
96
99
NPV
99
96
99 98
AUC
(95%
0.95 (0.84–1.05)
0.87 0.93
(0.72–1.02)
0.88 (0.72–1.04)
points)
toCI)
identify an individual
with any ‡1 ICD0.96
(as(0.93–0.99)
AUC (95% CI)
0.78
0.79
(0.87–0.98)
(0.63–0.92)
(0.52–1.05)
opposed
to examining
each individual ICD). This analya a
per ICD.
各Two
ICDquestions
につき質問は
2 項目。
b
sis
had
AUC
5 4.
0.88 (sensitivity 5 0.97, specificity 5
Questions
#14。
and
b
PPV, positive predictive value; NPV, negative predictive value;
質問
1 および
c
Questions
#1 0.53,
and 2. and NPV 5 0.99).
AUC, area under the curve.
0.79,
PPV
5
c d
質問 1 および 2。
Questions #1 and 5.
e
Questions
#15。
and 3.
質問
1 および
PPV,
positive3。
predictive value; NPV, negative predictive value; AUC, area under the curve.
e
質問
1 および
PPV =陽性適中率,NPV
=陰性適中率,AUC
=曲線下面積
Movement
Disorders, Vol. 24, No.
10, 2009
d
compulsive medication use endorsed by the sole
patient who met diagnostic criteria (for a total of
13 questions). A single positive response to any disorder’s/behavior’s question is a positive screen for that
disorder or behavior.
Combining Disorders/Behaviors
As we did for the QUIP, we assessed the validity of
sexual behavior, and buying, has been used in PD.4,17
However, the MIDI does not cover compulsive eating
or other compulsive behaviors, and thresholding of
scores to identify cases has varied across studies.
Different rating scales (e.g., the South Oaks Gambling Screen25), questionnaires (Punding Questionnaire20), and diagnostic criteria (DSM-IV diagnostic
criteria for pathological gambling, McElroy criteria
26
31
代謝比率で評価したパーキンソン病患者の大脳皮質の代謝
低下は主に認知機能低下を反映する:
[18F]FDG-PET
Cortical Hypometabolism Assessed by a Metabolic Ratio in Parkinson’s Disease Primarily Reflects
Cognitive Deterioration—[18F]FDG-PET
*
Inga Liepelt, PhD, Matthias Reimold, MD, Walter Maetzler, MD, Jana Godau, MD, Gerald Reischl, PhD, Alexandra Gaenslen, MD, Heinz
Herbst, MD, and Daniela Berg, MD
*
Hertie Institute for Clinical Brain Research, Department of Neurodegenerative Diseases, University of Tuebingen, Tuebingen, Germany
認 知 機 能 が 低 下し た パ ー キ ン ソン 病(Parkinson’
的な FDG 取り込 み の平 均値)を計 算し,認 知機 能
Disease;PD)患者では,
[ F]フルオロデオキシグル
(Minimental State Examination; MMSE)
,運動能力
コース陽電子放射断層撮影(fluorodeoxyglucose-
(Unified Parkinson’
s Disease Rating Scale; UPDRS
positron emission tomography; FDG-PET)により大
Part Ⅲ )
,行動(Neuropsychiatric Inventory)の各評
脳皮質の局所的な代謝低下が認められる。本研究の目
価スコアと比較した。ステップワイズ線形回帰分析の結
的は,PD 患者の総体的な代謝低下程度を単一指標で把
果,MI との有意な関連が認められたのは MMSE スコア
握できる強力な手法を開発することと,代謝低下と最も
。 DSM- Ⅳ の基準に照ら
のみであった( p < 0.001)
高い相関を示す臨床的特徴を明らかにすることである。
して診断した認知症に対する MI の推計学的な感度およ
PD] 患者 22 例(10 例は認知症を伴う)と対照被験者
び特異度は高く,それぞれ 91%および 100%であった。
7 例に FDG-PET を施行した。患者ごとに代謝指数
今回のデータを総合すると,PD 患者における大脳の代
18
(metabolic index; MI)
(典型的な病変部における相対
謝低下は主に認知障害と関連することが示された。
Movement Disorders Vol. 24, No. 10, 2009, pp. 1504–1511
Key Word パーキンソン病,PET,認知症
CORTICAL HYPOMETABOLISM IN PARKINSON’S DISEASE
Spearman-rank correlation coefficients (q)および MI*)
show that this index is able to differentiate b
Table 2 PD TABLE
患者(222.例)の臨床的特徴および代謝指数(MI
between the clinical characteristics and the metabolic indices
PDND and PDD patients with very high accurac
間の Spearman 順位相関係数(ρ)
(MI and MI*) for patients with Parkinson’s disease (n 5 22)
Brain regions typically showing decrease
MI
Age (years)
Disease duration
(years)
Levodopa (mg/day)
Unified Parkinson’s
Disease Rating
Scale Motor score
Minimental State
Examination
score
Neuropsychiatric
Inventory-total
score
Neuropsychiartric
Inventory-dysphoria
score
Neuropsychiatric
Inventory-hallucination
score
32
MI*
q
Level of
significance
q
Level of
significance
20.19
20.15
P 5 0.41
P 5 0.52
20.16
20.21
P 5 0.49
P 5 0.36
20.07
20.41
P 5 0.75
P 5 0.06
20.006
20.42
P 5 0.98
P 5 0.06
0.75
P < 0.001
0.75 P < 0.001
20.30
P 5 0.17
20.38
P 5 0.08
0.19
P 5 0.40
0.13
P 5 0.57
20.64 P 5 0.001 20.60
P 5 0.003
Post Hoc Analysis: Diagnostic Accuracy
of [18F]FDG-PET for PDD
ROC analysis revealed an area under the curve
(AUC) of 0.95 (95% confidence interval [CI]:
0.85–1.00) for differentiation of PDD (n 5 10) and PD
uptake in PD appear in the nominator of thi
while the remaining gray matter appears
denominator. Therefore, absolute quantificat
FDG uptake including blood sampling is not ne
However, this definition leaves some room to
what actually qualifies a region ‘‘typically s
decreased FDG uptake.’’ If a conservative st
threshold is applied to identify differences in
uptake between PDND patients and controls
regions will appear in the denominator althou
do show disease related hypometabolism (
error). The effect might be that the calculated ra
marily reflects hypometabolism in selected are
(i.e. those with the highest effect size), rather t
overall extent of metabolic deterioration whi
also include disease-related hypermetabolism, e
to compensatory increase in neuronal activ
avoid this problem and to equally account for
hyper- and hypometabolism, we calculated the
tive index MI* with a threshold of t > 0, whic
most liberal threshold possible but associated
increased possibility of a type I error. Both indi
culated in this article correlated closely, so t
aforementioned effects did not compromise our
The MI correlated more closely with the MM
measurement of dementia severity than with th
Abstract
28
26
20
8
28
26
用したマスク処理画像(mask)
。これらのマスク処理画像は,認知症を伴わない
PD 患者と対照被験者とのボクセル毎の群間比較で作成した(黄色:ボクセル毎で
22
p < 0.05,オレンジ色:t > 0)
。
22
30
A
Figure 1 代謝指数(MI,黄色)と代替代謝指数(MI*,オレンジ色)の計算に使
24
24
rho = 0.77
18
0.85
0.9
0.95
1
1.05
1.1
A
B
1.15
1.2
20
rho = 0.77
18
0.85
1.25
rho = -0.66
8
0.9
0.95
1
1.05
1.1
B
1.15
1.2
1.25
rho = -0.66
28
NPI - Hallucination
Minimental
State Examination
NPI - Hallucination
30
A
Minimental State Examination
Minimental State Examination
30
6
26
4
24
222
20
rho = 0.77
0
18
0.85
0.85
0.9
0.9
B
0.95
0.95
11
1.05
1.05
1.1
1.1
1.15
1.15
Metabolic Index (MI)
1.2
1.2
6
4
2
0
1.25
1.25
0.85
0.9
0.95
1
1.05
1.1
1.15
1.2
1.25
Metabolic Index (MI)
rho
= -0.66
Figure 2 代謝指数(MI)と Minimental State
Examination(MMSE)スコア(上図)および
Neuropsychiatric Inventory(NPI)の幻
覚関連項目スコア(下図)との Spearman 順位相関解析。黒点は認知症を伴う PD 患者,白点は認知症のない PD 患者,白十字は対
照被験者を示す。
6
NPI - Hallucination
8
4
33
2
0
パーキンソン病における衝動行動と強迫行動
Impulsive and Compulsive Behaviors in Parkinson’s Disease
*
Andrew H. Evans, FRACP, Antonio P. Strafella, MD, Daniel Weintraub, MD, and Mark Stacy, MD
*
Department of Neurology, Royal Melbourne Hospital, and Department of Medicine, University of Melbourne, Parkville, Australia
抗パーキンソン病療法は,複雑で抑制の利かない一連
dysregulation syndrome; DDS)もこれに含まれる。よ
の精神運動障害など,様々な非運動症状の主要原因とな
くみられる ICD には,病的賭博,性欲過剰,強迫摂食,
りうる。これらの非運動症状はいずれも,反復的で,報
強迫買い物症などがある。本総説では,これらの障害の
酬や動機に基づく性質を有する。これらの行動は異常な
現象学,疫学,ならびに同定・評価方法に焦点を合わせ
または過剰なドパミン受容体刺激に関連し,衝動制御障
て検討する。ドパミン作動薬に関連する強迫行動の管理
害(impulse control disorder; ICD)
,反復常同行動
については,現時点におけるこれらの障害の神経生物学
(punding)
,ド パ ミン 調 節 異 常 症 候 群(dopamine
的基質に関する理解を踏まえて考察する。
Movement Disorders Vol. 24, No. 11, 2009, pp. 1561–1570
Key Word パーキンソン病,衝動制御障害(impulse control disorder; ICD),ドパミン調節異常症候群(dopamine
dysregulation syndrome; DDS),反復常同行動(punding),中脳辺縁系,報酬,腹側線条体
34
Abstract
Figure 1 腹側被蓋野(ventral tegmental area; VTA)から生じ,側
坐核(nucleus accumbens; NA)と前頭前皮質(prefrontal cortex;
PFC)に投射する中脳辺縁系ドパミン作動系。扁桃体(amygdala; A)
と海馬(hippocampus; HC)は NA に投射を送る。
[カラーの図は
www.interscience.wiley.com のオンライン版で閲覧可能]
。
IMPULSIVE AND COMPULSIVE BEHAVIORS IN PD
1565
Table 1 DDS,ICD,反復常同行動(punding)の発現との関連が報告されている薬剤,疾患,個人因子
TABLE 1. Medication, disease, and individual factors reported to be relevant to the emergence of DDS, ICDs, and punding
ICDs
Medication factors
Dopamine agonist use
Longer agonist therapy
Agonist dose
Total medication dose
Disease factors
Early PD onset
Disease duration
Cognitive dysfunction
Individual factors
Impulsivity
Male gender
Marital status
Prior substance use
Depression
Medication-induced mania
Family history
DDS
PG
HS
Punding
No
Yes
Probable
Probable
Probable
Yes
Yes
Probable
Probable
Probable
Yes
Yes
9.5 years74
Possible
Yes
7.8 years34
Yes
9.6 years
Yes
Longer
Yes
No
Yes
Yes
Yes
Yes
Possible
Yes
Yes
Yes
Yes
Yes
No
Yes
No
Yes
Modifies phenomenology
Yes
Yes
Yes
abusers have consistently reported long-lasting reductions in the level of striatal dopamine D2 receptors.
Chronic drug consumption appears to reduce striatal
dopamine activity and also leads to a dose-related disruption of metabolism in the frontal regions particularly the orbitofrontal and anterior cingulate cortex86—
brain regions implicated in motivation, drive and inhibitory control respectively. Cocaine abusers also display
decreased dopamine cell activity, as evidenced by
reduced dopamine release in response to a pharmaco-
Assoc. with poorer disease related QoL
sufficient to drive compulsive dopaminergic drug use
in PD patients.
Aberrant Learning and Impaired
Behavioral Inhibition
The Iowa Gambling task emphasizes the learning of
reward and punishment associations in order to guide
ongoing decision-making. The task is sensitive to dysfunction of the ventromedial cortex in which individu-
35
パーキンソン病と多系統萎縮症における胃筋電図所見の違い
Gastric Myoelectrical Differences between Parkinson’s Disease and Multiple System Atrophy
*
Yumi Sakakibara, MD, Masato Asahina, MD, PhD, Atsuya Suzuki, MD, PhD, and Takamichi Hattori, MD, PhD
*
Department of Neurology, Graduate School of Medicine, Chiba University, Chiba, Japan
600
胃筋電図(electrogastrogram; EGG)を,パーキンソ
frequency range; NFR%)
,高周波数帯域(ratio of
ン病(Parkinson’
s disease; PD)患者 17 例,多系統
high frequency range; HFR%)の割合を求めた。PD
萎縮症(multiple system atrophy; MSA)患者 17 例,
患者では不規則徐波,HFR%高値,ICDF 高値を認めた
健常対照被験者 8 例で 24 時間にわたって記録し,両
µV
0
のに対し,MSA
患者では規則的徐波と ICDF 低値を認
疾患の EGG 所見の違いを検討した。スペクトル解析の
めた。対照群では食後に
DF と NFR%が上昇したが,
-200
ため,全記録から 8 つの EGG セグメント(食前 3,食
両患者群では DF と NFR%の食後の上昇程度は対照群
後 3,睡眠時 2)を選択し,優位周波数(dominant
A
よりも有意に小さかった。PD
患者では,胃ペースメー
frequency; DF)
,DF の 不 安 定 性 係 数(instability
カー障害を示す
0
1 EGG2上の律動不整がみられた。MSA
3
4
5
coefficient of dominant frequency; ICDF)
,総パワー
患者では徐波リズムの変動性が少ない(ICDF 低値の)
値に占める低周波数帯域(ratio of low frequency
400
規則的徐波が認められたが,これは胃自律神経機能に起
range; LFR%)
,標準周波数帯域(ratio of normal
200
因する可能性がある。
400
200
-400
-600
600
µV
0
Movement Disorders Vol. 24, No. 11, 2009, pp. 1579–1586
-200
-400
Key Word 胃筋電活動,胃筋電図,パーキンソン病,多系統萎縮症,自律神経系
B
-600
0
µV
600
600
400
400
200
200
µV
0
-200
2
3
4
5
1
2
3
4
5
0
-200
-400
-600
1
-400
A
0
1
2
3
4
5
C
-600
0
600
400
200
µV
0
-200
-400
B
-600
0
600
400
36
200
µV
0
-200
1
2
3
4
5
Figure 1 (A)健常対照被験者,
(B)多系統萎縮症(MSA)
患者,
(C)パーキンソン病(PD)患者において空腹時に記
録した胃筋電図(未加工)
。
Abstract
A
B
4.0
*
14
2.0
9
cpm
%
0
Control MSA
Figure 2 対照被験者,多系統萎縮症(MSA)患者,パー
キンソン病(PD)患者における(A)優位周波数,
(B)
優位周波数の不安定性係数,
(C)低周波数帯域の割合
(LFR%)
,
(D)標準周波数帯域の割合(NFR%)
,
(E)
高周波数帯域の割合(HFR%)
。8 つのセグメントの平
均値。*p < 0.05,**p < 0.01。
*
**
4
PD
Control MSA
C
PD
D
E
*
40
65
20
%
45
%
0
25
40
20
%
Control
Control MSA PD
MSA
PD
Control
3.4
3.2
3.0
2.8
2.6
Á
Á
Á
15
10
5
*
0
t
s
e-
*p<0.05
le
ep
ea
br
r
r
h
h
p
st
ne
ne lee
nc
nc
fa
ak e-lu t-lu -din -din y-s
e
t
r
rl
pr pos pre os
-b
ea
p
st
kf
epr
po
as
PD
50
40
30
20
80
70
60
50
40
t
compared with the controls.
p<0.05, Á p<0.01 between the MSA and PD groups.
Figure 3 対照被験者,多系統萎縮症(MSA)患者,パー
キンソン病(PD)患者における(A)優位周波数(DF)
,
(B)優位周波数の不安定性係数(ICDF)
,
(C)低周波数
帯 域 の 割 合(LFR %)
,
(D)標 準 周 波 数 帯 域 の 割 合
(NFR%)
,
(E)高周波数帯域の割合(HFR%)の 24 時
間変化。* 対照群との比較で p < 0.05。MSA 群と PD 群
との比較で† p < 0.05,‡ p < 0.01。
E
High-frequency range
(%)
ICDF (%)
Á*
20
Normal-frequency range
(%)
D
25
la
MSA
10
2.4
B
Control
C
3.6
Low-frequency range
(%)
Dominant frequency
(cycle/min)
A
0
MSA PD
40
30
20
10
0
t
t
h
h
er ner
ep
ep
as
as
nc inn
nc
le
n
kf
sle akf
lu t-lu
d
di ly-s
ea ree
t
r
r
s
e
r
p
la e-b
-b
pr pos
po
ea
st
pr
po
te
37
早期パーキンソン病における抑うつ症状の経過
The Course of Depressive Symptoms in Early Parkinson’s Disease
*
Bernard Ravina, MD, MSCE, Jordan Elm, MA, Richard Camicioli, MD, Peter G. Como, PhD, Laura Marsh, MD, Joseph Jankovic, MD, and
Daniel Weintraub, MD
*
Department of Neurology, University of Rochester School of Medicine and Dentistry, Rochester, New York, USA
パーキンソン病(Parkinson’
s disease; PD)患者にみ
と判定され,GDS-15 スコアの中央値は軽度の抑うつ
られる抑うつ症状の経過についてはほとんど知られてい
を示す 6 であった。患者の 47%は,6 ヵ月以内に臨床
ない。本研究では,未治療の早期 PD 患者 413 名を
的に有意な抑うつ症状が寛解した。軽度の抑うつ症状
12 ~ 18 ヵ月間経過観察した 2 つの臨床試験のデータ
がある患者は,それまで抑うつ症状がなかった患者に比
を用いて,
臨床的に有意な抑うつ症状の経過を検討した。
べると,中等度~重度の抑うつ症状(GDS-15 スコア
抑うつ症状は,
15項目の老年期うつ病評価尺度
(15-item
≧ 10)を発現する傾向があった(相対リスク= 6.16)
。
geriatric depression scale; GDS-15)を用いて評価し
抑うつ症状の重症度が高いほど,年齢が高いほど,そし
た。GDS-15 スコアが 5 以上の場合,臨床的に有意な
て PD 罹病期間が長いほど,症状消失の可能性は低下す
抑うつ症状ありと判定される。本研究では,抑うつ症状
ると予測された(ハザード比 0.83 ~ 0.92)
。軽度の抑
が消失するまでの時間と,患者の人口統計学的変数,
うつ症状は様々な経過をたどり,時間の経過とともに寛
PD 重症度,薬剤使用との関連性を,時間依存性 Cox モ
解することもあれば,さらに持続的かつ重度の症状が発
デルを用いて検討した。患者 413 名中 114 名
(27.6%)
現する場合もある。重症度の高い抑うつ症状は,遷延
が試験期間中のスクリーニングによって抑うつ症状あり
性の経過をたどることの前触れかもしれない。
Movement Disorders Vol. 24, No. 9, 2009, pp. 1306–1311
Key Word パーキンソン病,抑うつ,臨床経過,予後
1.0
0.9
Proportion Remaining Depressed
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0
3
6
9
12
15
18
21
Time from First Observed GDS>=5 (mo)
Figure 1 ベースライン時の抑うつ症例および経過観察中の新規
発症例における寛解までの期間に関する Kaplan-Meier プロット
38
Abstract
Baseline and Incident Cases
N=114
77
61
28
Percent of subjects
(at each time point)
100%
90%
80%
70%
Mod/severe
GDS >9
Mild
GDS 5-9
60%
50%
40%
30%
20%
Not Depressed
GDS <5
10%
0%
0
6
12
18
Time (months) after screening positive
Figure 2 ベースライン時の抑うつ症例および経過観察中の新規
発症例における GDS-15 スコアの経時的変化
DEPRESSIVE SYMPTOMS IN EARLY PD
Table
2 抑うつが寛解(GDS-15
に回復)するまで
TABLE
2. Cox Regression model<
of5time
to depression
remission (returnCox
to GDS
, 5)
の時間に関する
回帰分析
study in early PD, 27% of the cohort screened p
for depression using the Beck Depression Inven
Only
15.9% of those who were depressed at b
95% Hazard
ratio
remained depressed at the final visit. Subjec
Hazard
confidence
P
remain depressed had higher baseline BDI
Variable
ratio
limits
value
Another study examining a range of PD s
Age, yr
0.91
0.86
0.96
0.001
showed that after 1 year, 63% of subjects with
Gender (reference is
1.11
0.55
2.26
0.77
depression were likely to be in remission, bu
Female)
Duration of PD
0.92
0.86
0.98
0.01
11% of subjects who initially had major dep
Diagnosis, mo
were in remission.13 Consistent with prior stud
Baseline GDS
0.83
0.70
0.98
0.03
found that the majority of cases of depression i
Baseline UPDRS total
1.02
0.97
1.06
0.52
Baseline Hoehn and Yahr
2.47
1.07
5.73
0.03
PD were in remission by 6 to 9 months, b
Baseline RBANS total
1.03
1.01
1.06
0.01
greater depression severity was associated with
score (reverse coded)
a
chance of remission.
1.3
0.51
3.22
0.60
Symptomatic therapy use
0.13
0.37
0.04
0.0002
Started antidepressantsa
We found a more than sixfold increase in
more
severe depressive symptoms among tho
本モデルでは試験,治療群,表中のすべての変数について補正
Model adjusts for study, treatment group, and all variables shown
had
minor
symptoms. Similarly, findings in a c
※
in table. RBANS was reverse coded so that higher
score is worse.
した。アーバンス(RBANS)神経心理テスト
は,スコアが高いほ
For all other scales a higher score is worse.
nity
setting
and general medical patients sugge
ど状態が不良となるように数値を逆転させた。他の尺度はいずれも
a
Time varying covariates. Overall model R2 5 0.4.
minor
or
sub-threshold
depression may predict
スコアが高いほど状態が不良であることを示す。
14
Chronic illness has als
quent
major
depression.
a
2
時間依存性共変量。モデル全体では R = 0.4。
associated with an increased risk for conversio
sub-threshold depression to major depression.15
model including both baseline and incident cases of
many of the community-based studies have h
depression, only initiation of antidepressants remained
low-up periods of one year, some have followe
a statistically significant predictor and were associated
jects for more than 10 years. Studies with long
with a reduced likelihood of remission (data not
low-up will help to clarify the evolution of dep
※
shown).Repeatable Battery for the Assessment of Neuropsychological Status の略称。高次脳機能を評価する
symptoms during the course of PD and help
日本語版注釈:米国の Randolph が開発した
treatment decisions. Our findings clearly indicat
心理検査。12 種類のテストにより,
「即時記憶」
「短期記憶」
「視空間・構成」
「言語」
「注意(集中)力」の 5 項目が評価できる。
ever, that careful monitoring of depressive sym
DISCUSSION
in PD is warranted.
This study assessed the course of clinically signifiWe modeled remission of depressive sympt
cant depressive symptoms in early PD subjects foltwo ways to maximize the 39
value of our dat
lowed for 12 to 18 months. We used data from two
model including only baseline cases allowed
clinical trials that were designed to evaluate progresinclude important covariates that were not meas
sion of PD, controlling for treatment assignment and
all visits, such as cognition (RBANS) and HY
other covariates. Most subjects who screened positive
The model using both baseline and incident cas
パーキンソン病におけるレボドパ空腸内注入:非運動症状
および QOL への効果に関する予備的多施設共同試験
Intrajejunal Levodopa Infusion in Parkinson’s Disease: A Pilot Multicenter Study of Effects on
Nonmotor Symptoms and Quality of Life
*
Holger Honig, MD, Angelo Antonini, MD, Pablo Martinez-Martin, MD, Ian Forgacs, FRCP, Guy C. Faye, FRCP, Thomas Fox, MD, Karen Fox,
MD, Francesca Mancini, MD, Margherita Canesi, MD, Per Odin, MD, PhD, and K. Ray Chaudhuri, MD, FRCP, DSc
*
Department of Neurology, Central Hospital, Bremerhaven, Germany
進行期パーキンソン病(Parkinson’
s disease; PD)患
睡眠 / 疲労,注意 / 記憶,消化器系,泌尿器系,その他
者では,内服治療からレボドパ(L—ドパ)/ カルビドパ・
(疼痛および流涎を含む)
〕と,NMSS の総合スコア
ゲル剤の持続注入に切り替えると,運動合併症が減少
(NMSST)で統計学的に有意な有益効果が認められ,運
する。しかし,非 運 動症 状(nonmotor symptom;
動症状〔
“best on”状態における UPDRS Part Ⅲ (運動
NMS)に対する効果は不明である。今回のプロスペク
(合併症)
〕とジスキネジア /motor
能力)および Part Ⅳ ティブな非盲検観察研究では,Nonmotor Symptoms
fluctuation の改善も並行して認められた。さらに,
Scale(NMSS)および Unified Parkinson’
s Disease
Parkinson’
s Disease Sleep Scale(PDDS)と PDQ-8
Rating Scale〔UPDRS Part Ⅲ (運動能力)および Part
(QOL)でも有意な改善が認められた。PDQ-8 スコア
(合併症)
〕 に よ る 標 準 的 評 価 と,Parkinson’
s
Ⅳ の改善は NMSST の変化ときわめて有意に相関したの
Disease Questionnaire(PDQ-8)による生活の質
に対し,UPDRS の変化との相関は中程度の強さであっ
(quality of life; QOL)の評価に基づき,PD の NMS に
た。本研究により,L—ドパによる持続性ドパミン刺激は,
対する L—ドパ / カルビドパ・ゲル剤空腸内注入の効果
motor fluctuation とジスキネジアの軽減に加え,PD 患
について報告する。進行期 PD 患者 22 例(平均年齢
者の NMS ならびに健康関連 QOL に対し,有益な効果
58.6 歳,罹病期間 15.3 年)を 6 ヵ月間追跡調査した。
を発揮することが初めて実証された。
NMSS を構成する 9 つの領域のうち 6 つ〔心血管系,
Movement Disorders Vol. 24, No. 10, 2009, pp. 1468–1474
LEVODOPA INFUSION AND NONMOTOR PD SYMPTOMS
1471
Key Word パーキンソン病,非運動症状,QOL,十二指腸,注入
Table 1 使用評価尺度のスコアと変化程度
TABLE 1. Scores of the
applied measures and magnitude of the change
Baseline score
UPDRS 3-Motor
UPDRS 4-Complications
UPDRS-Dyskinesia scorea
PD Sleep Scaleb
PDQ-8
NMSS-Total score
Cardiovascular
Sleep/Fatigue
Mood/Cognition
Perception/Hallucinations
Attention/Memory
Gastrointestinal
Urinary
Sexual
Miscellaneous
19.1
10.5
5.6
86.0
44.2
89.9
2.9
18.1
15.3
2.9
7.3
10.0
11.4
7.9
14.1
(14.0)
(2.9)
(2.3)
(13.2)
(18.4)
(56.5)
(3.6)
(15.8)
(15.3)
(5.2)
(8.1)
(9.3)
(10.7)
(8.2)
(8.0)
Follow-up score
11.6
4.5
1.9
114.5
20.7
39.4
0.5
6.8
7.8
1.3
4.0
3.8
4.8
3.9
6.4
(7.2)
(2.2)
(1.5)
(16.2)
(12.0)
(33.9)
(1.3)
(7.7)
(11.2)
(3.4)
(5.6)
(5.4)
(6.1)
(5.7)
(6.1)
P*
Mean D in score
Relative change (%)
0.002
0.0000
0.0001
0.002
0.0003
0.0001
0.0004
0.0001
0.02 NS
0.1 NS
0.002
0.0003
0.002
0.03 NS
0.0004
27.54
25.91
23.7
28.51
223.4
250.55
22.41
211.32
27.50
21.54
23.27
26.23
26.64
23.91
27.73
239
256
267
33
253
256
281
263
249
254
245
262
258
250
255
* *Wilcoxon test: Mean (SD). Bonferroni correction: 0.003; NS, no significant; D, difference baseline-follow-up; UPDRS, Unified Parkinson’s
Wilcoxon 検定:平均(SD)
。Bonferroni 補正:0.003。NS =有意性なし,Δ=ベースライン時と追跡調査時の差,UPDRS = Unified
disease rating scale.
Parkinson’
s Disease Rating Scale
a
UPDRS-Dyskinesia, items 32 to 35 of the UPDRS; PD Sleep Scale, Parkinson’s Disease Sleep Scale; PDQ-8, Parkinson’s disease questiona
UPDRS(ジスキネジア)
,UPDRS
の項目
32 ~ 35。PD Sleep Scale = Parkinson’
s Disease Sleep Scale,PDQ-8 = Parkinson’
s Disease
naire-8
items; NMSS, nonmotor
symptoms
scale.
b
(nPDSS 5 15).
Increase in=
PDNonmotor
sleep scale
score means
Questionnaire-8
項目,NMSS
Symptoms
Scaleimprovement. In all other used scales increased score means worsening.
(nPDSS = 15)
。PD Sleep Scale スコアの増加は改善を意味する。使用した他のすべての尺度では,スコアの増加は悪化を意味する。
b
40
gastrointestinal, urinary, and miscellaneous) and
NMSST. The remaining three categories (mood/cognition, perception/hallucinations, sexual function) showed
a trend for improvement.
The change in NMSST score showed a moderate
strongly associated with improvement in NMSST
scores (rS 5 0.61; P 5 0.003) and moderately with
changes in UPDRS-3 motor (rS 5 0.42; P 5 0.05) and
UPDRS-4 complications (rS 5 0.47; P 5 0.03). The
strongest correlations between changes in NMSS
© Copyright 2025 Paperzz