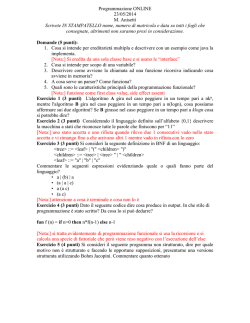
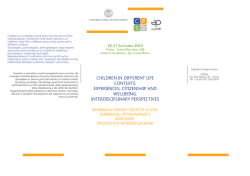
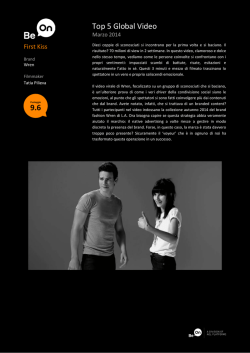
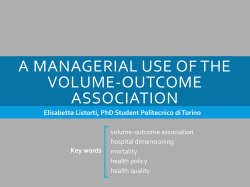
Bone Marrow Transplantation (2015) 50, 181–188 © 2015 Macmillan Publishers Limited All rights reserved 0268-3369/15 www.nature.com/bmt ORIGINAL ARTICLE Outcome of children with high-risk acute myeloid leukemia given autologous or allogeneic hematopoietic cell transplantation in the aieop AML-2002/01 study This article has been corrected since Advance Online Publication and an erratum is also printed in this issue. F Locatelli1,2, R Masetti3, R Rondelli3, M Zecca4, F Fagioli5, A Rovelli6, C Messina7, E Lanino8, A Bertaina1, C Favre9, G Giorgiani4, M Ripaldi10, O Ziino11, G Palumbo1, M Pillon7, A Pession3, S Rutella1,12 and A Prete3 on behalf of AIEOP BMT Working Group We analyzed the outcome of 243 children with high-risk (HR) AML in first CR1 enrolled in the AIEOP-2002/01 protocol, who were given either allogeneic (ALLO; n = 141) or autologous (AUTO; n = 102) hematopoietic SCT (HSCT), depending on the availability of a HLA-compatible sibling. Infants, patients with AML-M7, or complex karyotype or those with FLT3-ITD, were eligible to be transplanted also from alternative donors. All patients received a myeloablative regimen combining BU, Cyclophosphamide and Melphalan; AUTO-HSCT patients received BM cells in most cases, while in children given ALLO-HSCT stem cell source was BM in 96, peripheral blood in 19 and cord blood in 26. With a median follow-up of 57 months (range 12–130), the probability of disease-free survival (DFS) was 73% and 63% in patients given either ALLO- or AUTO-HSCT, respectively (P = NS). Although the cumulative incidence (CI) of relapse was lower in ALLO- than in AUTO-HSCT recipients (17% vs 28%, respectively; P = 0.043), the CI of TRM was 7% in both groups. Patients transplanted with unrelated donor cord blood had a remarkable 92.3% 8-year DFS probability. Altogether, these data confirm that HSCT is a suitable option for preventing leukemia recurrence in HR children with CR1 AML. Bone Marrow Transplantation (2015) 50, 181–188; doi:10.1038/bmt.2014.246; published online 10 November 2014 INTRODUCTION The outcome of children with AML has significantly improved over the past two decades.1–3 Besides better risk stratification, use of repeated course of intensive consolidation therapy and amelioration of supportive therapy, a remarkable contribution to this improvement has been given by the wide use of hematopoietic SCT (HSCT).4–7 In particular, for children achieving first CR1, allogeneic (ALLO) HSCT from an HLA-identical sibling has been shown to be the most effective post-remission therapy for preventing leukemia recurrence.5,7 Nowadays, large cooperative groups consider AML children with high-risk (HR) features, such as unfavorable cytogenetic/molecular characteristics or poor minimal residual disease clearance, eligible to be offered an allograft from an HLA-compatible sibling in CR1.2,8 In the past few years, several studies have documented that transplantation of unrelated CB cells in children with CR1 AML is associated with a favorable outcome, particularly in patients aged less than 1 year at time of diagnosis.9–11 The use of high-resolution molecular typing techniques for selecting an unrelated donor (UD) has also dramatically reduced the risk of immune-mediated complications and TRM, thus widening the indications for HSCT from an unrelated volunteer, which now are in part coincident with those for matched-related HSCT.12,13 Although largely used in the past,14,15 more recently the role of autologous (AUTO) HSCT has been questioned, especially in view of similar efficacy to repeated courses of intensive high-dose cytarabine (HD-AraC)-based consolidation chemotherapy for prevention of disease recurrence.5,16 We recently reported that risk-oriented treatment and broad use of HSCT in children with CR1 AML resulted in a long-term outcome, which compares favorably with that reported in other patient series.17 In this study, we thoroughly analyze the results of the 243 HR children enrolled in the AIEOP AML 2002/01 protocol, who were given either AUTO or ALLO HSCT for consolidating remission after achievement of CR1. PATIENTS AND METHODS Patients Included in this study were 243 HR children in CR1, aged 0–18 years, affected by de novo AML other than acute promyelocytic leukemia, who were treated according to the AIEOP AML 2002/01 protocol, which was approved by the Ethical Committee of each participating Institution (listed 1 Department of Pediatric Hematology-Oncology, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Bambino Gesù Children's Hospital, Roma, Italy; 2Department of Pediatric Science, University of Pavia, Pavia, Italy; 3Pediatric Oncology and Hematology Unit ‘Lalla Seragnoli’, Department of Pediatrics, University of Bologna Sant’Orsola-Malpighi Hospital, Bologna, Italy; 4Department of Pediatric Onco-Hematology, IRCCS, Policlinico San Matteo Foundation, Pavia, Italy; 5Pediatric Onco-Hematology, Stem Cell Transplantation and Cellular Therapy Division, Regina Margherita Children's Hospital, Torino, Italy; 6Department of Pediatric Hematology, San Gerardo Hospital, Monza, Italy; 7 Department of Pediatric Hematology and Oncology, University of Padova, Padova, Italy; 8Department of Pediatric Hematology Oncology, IRCCS G. Gaslini Institute, Genova, Italy; 9 Department of Pediatrics, University of Pisa, Pisa, Italy; 10BMT Unit, Department of Pediatric Hemato-Oncology, Santobono-Pausilipon Hospital, Napoli, Italy; 11Pediatric Hematology/Oncology, ARNAS Ospedale Civico di Palermo, Palermo, Italy and 12Department of Medical Sciences, Catholic University Medical School, Rome, Italy. Correspondence: Professor F Locatelli, Department of Pediatric Hematology and Oncology, IRCCS Ospedale Pediatrico Bambino Gesù, Piazza S. Onofrio, 4, Rome 00165, Italy. E-mail: franco.locatelli@opbg.net Received 15 July 2014; revised 6 September 2014; accepted 11 September 2014; published online 10 November 2014 Autologous and allogeneic HSCT in childhood AML F Locatelli et al 182 before references). Either parents or legal guardians provided written informed consent to patient treatment. Patients with a previous myelodysplastic phase, with Down's syndrome or who had received previous treatment with either cytotoxic agents or steroids in the 2 weeks preceding diagnosis were deemed not to be eligible for inclusion into the study. Details on demographics and clinical or biological characteristics of these HR patients are shown in Table 1, which also includes a separate analysis of children who received either AUTO- or ALLO-HSCT. Table 1. Donor selection In the AIEOP AML 2002/01 protocol, patients with isolated anomalies of CBF-β and in morphologic CR after the first induction course were allocated to the standard-risk (SR) group; the remaining children were assigned to the HR group and, thus, eligible to be treated with HSCT. All these HR children with an available HLA-compatible sibling were transplanted using this type of donor. Infants, patients with AML-M7, those with a complex karyotype or FLT3-internal tandem duplication (ITD) Patients and donor characteristics Whole population % AUTO-HSCT (%) ALLO-HSCT (%) P-value 107 136 44 56 43 (40) 57 (42) 64 (60) 79 (58) ns ns Age Median age at HSCT, years (range) o1 year 1–2 year 2–10 year 410 year 7.2 (0.6–17.5) 46 27 92 78 19 11 38 32 7 10 44 40 39 17 48 38 WBC count (x109/L) WBC at diagnosis, median (range) o10 10–99 4100 23.9 (0.9–475) 96 112 35 39 46 15 37 (39) 45 (40) 19 (54) 59 (61) 67 (60) 16 (46) 16 40 45 39 67 4 25 7 7 16 18 16 28 2 10 3 5 24 17 20 33 0 0 3 11 16 28 19 34 4 25 4 33 192 18 4 45 24 4 14 79 7 2 19 10 2 10 (30) 23 (70) 0 0 20 4 0 18 2 25 20 4 243 % 102 58 75 45 30 15 7 8 8 42 24 31 19 12 6 3 3 3 141 93 26 22 102 87 15 58 66 18 16 42 85 15 Patients Gender F M FAB M0 M1 M2 M4 M5 M6 M7 Unclassifiable/not known Subgroups CNS leukemia at diagnosis Available cytogenetic data Complex karyotype Monosomal karyotype 11q23 abnormalities FLT3-ITD-positive FLT3-TKD-positive Donor Type of donor AUTO MFD UD Fully matched Mismatched 1 antigen 1 allele 4 1 antigen/allele HAPLO Stem cell source Allogeneic BM Cord PBSC Autologous BM PBSC (15) (37) (48) (51) (31) (60) (38) (51) (49) (0) (0) (43) (0) (0) (44) (17) (0) (85) (63) (52) (49) (69) (40) (62) (49) (51) (100) (100) (57) (100) (100) (56) (83) (100) ns o0.001 ns ns ns ns ns ns 0.002 ns ns ns ns o0.001 o0.001 ns 0.001 ns o0.001 o0.001 ns o0.001 o0.001 Abbreviations: AUTO = autologous; CNS = central nervous system; F = female; HAPLO = HLA-haploidentical; HSCT = hematopoietic SCT; M = male; MFD = matched family donor; pts = patients; UD = unrelated donor. Bone Marrow Transplantation (2015) 181 – 188 © 2015 Macmillan Publishers Limited Autologous and allogeneic HSCT in childhood AML F Locatelli et al 183 or achieving CR1 only after the second course of induction therapy were considered eligible to be transplanted from an alternative donor, namely an UD, or an unrelated CB donor or an HLA-partially matched family donor. Eligible for AUTO-HSCT were those HR children without an HLA-identical sibling who did not qualify for receiving an allograft from an alternative donor. As far as children transplanted from either an HLA-identical sibling or using CB cells are concerned, in both donor and recipient, histocompatibility was determined by serology for HLA-A and HLA-B antigens and by DNA typing for the HLA-DRB1 locus. In all children transplanted from an UD, both class I and class II HLA alleles (that is, HLA-A, HLA-B, HLA-C, DRB1 and DQB1) of the donor/recipient pair were typed by high-resolution, 4-digit DNA technique. All UD ALLO-HSCT recipients were transplanted using a donor with complete identity or a single-locus mismatch. The transplant centers preferentially required BM as the stem cell source; however, the final choice was left to the UD. Of the 26 CB transplant recipients, 10 were transplanted from an HLA-identical donor, 11 from a 1-antigen disparate donor, and 5 using a unit with 2 HLA disparities. For patients candidate to receive an UD ALLO-HSCT, the search for locating a suitable unrelated volunteer or a CB unit started simultaneously. CB transplantation was performed whenever a donor with an HLA compatibility of at least 4/6 and a pre-thawing number of total nucleated cells/kg of recipient’s body weight of at least 3.5 × 107 was available. Pre-transplant treatment Before transplantation, all patients had been given two courses of induction chemotherapy, including idarubicin, cytarabine and etoposide (ICE, see Ravindranath et al.16 for details). After having achieved CR1, two consolidation courses including HD-Ara-C, combined with either etoposide in the first course (AVE) or mitoxantrone in the second course (HAM) were administered. BM harvesting and in vitro purging with mafosfamide for patients given AUTO-HSCT was recommended after the first consolidation course.14 Purging was performed for 78 AUTO-HSCT. Conditioning regimen and GVHD prophylaxis The conditioning regimen was homogenous in all the patients and it consisted of a combination of Busulfan (BU, 16 mg/Kg over 4 days), Cyclophosphamide (CY, 120 mg/Kg divided in two doses) and Melphalan (L-PAM, 140 mg/m2).18 Seventy-five percent of patients received oral BU, the remaining being treated with the i.v. formulation of the drug. In 221 out of the 243 patients (91%), BU dosage was adjusted based on the pharmacokinetic study performed in a centralized laboratory in Pavia following the first administration, in order to maintain a steady-state concentration comprised between 600 and 900 ng/mL. GVHD prophylaxis consisted of CsA alone for 95% of matched family donor recipients, and of a combination of CsA, short-term MTX and rabbit anti-thymocyte globulin (ATG, 2.5–3.75 mg/kg/day from day − 4 to day − 2) for 85% of UD recipients. Children transplanted with unrelated CB units received a GVHD prophylaxis based on the combination of CsA and steroids.11 Definitions Patients were considered in morphological CR if they had o5% blast cells in a BM smear, no extramedullary disease and normal neutrophil and platelet counts. All the patients had a lumbar puncture before HSCT to document cerebrospinal fluid CR. Neutrophil and platelet engraftment were defined as the first of the three consecutive days with a neutrophil count 40.5 × 109/L and an unsupported platelet count 420 × 109/L, respectively. Acute and chronic GVHD (aGVHD and cGVHD) were diagnosed and graded according to established criteria.19,20 Children surviving more than 14 days and 100 days post transplantation and with evidence of donor engraftment were evaluated for the occurrence of aGVHD and cGVHD, respectively. Relapse was defined on the basis of morphological evidence of leukemia in BM, or at other extramedullary sites. TRM was defined as all causes of non-leukemia death occurring after HSCT. OS was defined as the interval between HSCT and either death or date of last follow-up. Diseasefree survival (DFS) was defined as the interval between HSCT and either relapse, or death, or date of last follow-up, whichever occurred first. Statistical analysis Patient-, disease- and transplantation-related variables were expressed as median and ranges, or as percentages, as appropriate. The following © 2015 Macmillan Publishers Limited patient- or transplantation-related variables were analyzed for their potential impact on outcome: gender, age, WBC at diagnosis, FrenchAmerican-British subgroups, donor type, stem cell source, abnormalities involving MLL, FLT3-ITD, aGVHD and cGVHD occurrence. Patients were censored at the time of relapse, death or last follow-up. Probability of OS and DFS was estimated by the Kaplan-Meier product-limit method and expressed as percentage ± s.e. aGVHD and cGVHD occurrence, as well as TRM and relapse incidence (RI), were expressed as cumulative incidence (CI) curves ± s.e., in order to adjust the analysis for competing risks.21 Death from any cause and graft rejection were competing risks to estimate the CI of aGVHD and cGVHD. Death in remission was treated as a competing event to calculate the cumulative RI. Relapse was considered to be the competing event for calculating the CI of TRM. The significance of differences between the DFS curves was estimated by the log–rank test (Mantel–Cox), whereas in the univariate analyses, Gray’s test was used to assess differences between RI and TRM. All variables having a p-value o .05 in univariate analysis were included in a multivariate analysis on DFS performed using the Cox proportional regression model,22,23 while the proportional sub-distribution hazard regression model was used to perform multivariate analyses of CI of relapse and death in continuous CR. Computations were performed using SAS (Statistical Analysis System, Version 8.2, SAS Institute Inc., Cary, NC, USA). Analysis used 31 March 2013 as the reference date. RESULTS The median observation time for the surviving patients, considering the whole study population, was 57 months (range: 12–130). The median follow-up did not differ according to the type of transplantation received by the patient (data not shown). The patient flowchart is depicted in Figure 1. The median time from achievement of CR to transplantation was 139, 125 and 136 days for AUTO-HSCT, HLA-identical sibling ALLO-HSCT and UD ALLOHSCT, respectively (P = ns). The stem cell source employed did not significantly influence the median time elapsing from achievement of CR and transplantation (data not shown). Hematopoietic recovery Neutrophil engraftment was reached in 240 out of 243 children and the median time to neutrophil recovery was 13 days (range 9– 61) and 17 days (range 9–52), for AUTO- and ALLO-HSCT recipients, respectively (P = 0.11). Platelet recovery was reached in 235 children, the median time for obtaining an unsupported platelet count more than 20 × 109/L being 21 days (range 12–119) and 25 days (range 10–132), for AUTO- and ALLO-HSCT recipients, respectively (P = 0.12). Chimerism analysis during 100 days was available for 135 out of the 141 patients receiving an allograft. Of those patients reaching neutrophil recovery, 99% had full donor chimerism and 1% were mixed chimera. Acute and chronic GVHD Eighty-two out of the 141 patients given an allograft developed grade I–IV aGvHD, the median time of onset being 14 days (range 8–70); 53 and 19 of them had grade II–IV and grade III–IV acute GvHD, respectively. The CI of grade II–IV and grade III–IV acute GVHD was 38.1% (s.e. 4.1) and 13.7% (s.e. 2.9), respectively (Figure 2a). The CI of grade II–IV aGVHD in children transplanted from either an HLA-identical sibling or an adult UD or with UD CB cells was 35.1% (s.e. 6.3), 45.1% (s.e. 7.2) and 38.5% (s.e. 9.5), respectively (P = ns). Thirty-three patients developed cGVHD, the median time of onset being 165 days (range 100–426). In 22 of them, cGVHD was of limited severity, while the remaining 11 children experienced the extensive form of the disease. In 27 patients, cGVHD was preceded by aGVHD. The overall CI of cGVHD was 25.3% (s.e. 3.8), while that of extensive cGVHD was 8.6% (s.e. 2.5; Figure 2b). Bone Marrow Transplantation (2015) 181 – 188 Autologous and allogeneic HSCT in childhood AML F Locatelli et al 184 AML 2002/01 study: 421 patients in CR after induction 96 SR patients treated with chemotherapy only 325 HR patients 113 AUTO-HSCT candidates 77 with an available MFD donor 135 eligible to UD 52 patients lost due to: toxic death/relapse during consolidation or refusal of HSCT 11 patients lost due to: toxic death/relapse during consolidation or refusal of HSCT 19 patients lost due to: toxic death/relapse during consolidation or refusal of HSCT 8 patients without a MUD 102 AUTO Figure 1. 8 HAPLO 75 MUD 58 MFD Consolidated Standards for Reporting of Trials (CONSORT) diagram. 100 CI of chronic GvHD (%; SE) CI of grade II-IV acute GvHD (%; SE) 100 75 50 Grade II-IV = 38.1%(4.1) 25 Grade III-IV = 13.7%(2.9) 75 50 Chronic GvHD = 25.3% (3.8) 25 Extensive chronic GvHD = 8.6%(2.5) 0 0 0 2 4 6 8 10 12 14 16 0 Weeks from HSCT 1 3 2 Years from HSCT Figure 2. (a) Cumulative incidence (s.e.) of grade II–IV and of grade III–IV aGVHD in the whole population of children given allogenic HSCT (ALLO-HSCT). (b) Cumulative incidence ( ± s.e.) of overall and extensive cGVHD in the whole population of children given ALLO-HSCT. Transplantation-related mortality Sixteen patients died from transplantation-related causes, seven after AUTO- and nine after ALLO-HSCT. Five of the seven patients who died after AUTO-HSCT had the fatal event before 2006. The CI of TRM in AUTO- and AUTO-HSCT was 7.1% (s.e. 2.8) and 7.4% (s.e. 2.5), respectively (P = ns). Neither type of donor nor stem cell source employed influenced the risk of TRM in the 141 patients given an allograft. Table 2 enlists the causes of death in patients given either ALLO- or AUTO-HSCT. Only one of the four children who died because of sinusoidal obstruction syndrome had a steady-state BU concentration higher than the recommended range (data not shown). The CI of TRM of the 82 patients who experienced GVHD was 8.9% (s.e. 3.6), whereas that of patients who did not develop GVHD was 7.0% (s.e. 3.4; P = ns). Likewise, occurrence of cGVHD did not influence the risk of dying for transplantation-related complications (data not shown). Bone Marrow Transplantation (2015) 181 – 188 Table 2. Causes of death in patients given either allogeneic or autologous HSCT Causes of death Autologus HSCT Allogeneic HSCT 4 — — 1 2 — 3 4 1 — Sinusoidal obstruction syndrome aGVHD cGVHD Pulmonary aspergillosis Bacterial sepsis Abbreviation: HSCT = hematopoietic SCT. Leukemia relapse Fifty-one patients experienced leukemia relapse: 29 after AUTOand 22 after ALLO-HSCT; the CI of leukemia recurrence was 28.3% © 2015 Macmillan Publishers Limited Autologous and allogeneic HSCT in childhood AML F Locatelli et al 185 100 Table 3. % (SE) 75 P=0.043 50 AUTO 8-year C.I. of relapse (SE) = 28.3% (4.5) 25 ALLO 8-year C.I. of relapse (SE) =17.4% (3.3) 0 0 2 6 4 8 10 Years from HSCT Figure 3. Cumulative incidence ( ± s.e.) of leukemia relapse in children with CR1 AML given either an autologous or an allogeneic HSCT. 100 ALLO 8-year DFS (SE) = 73% (4.0) % (SE) 75 AUTO 8-year DFS (SE) = 63% (4.9) 50 25 0 0 2 4 6 8 10 Years from HSCT Figure 4. Eight-year probability of disease-free survival (DFS, ± s.e.) for children with CR1 AML given either an allogeneic or an autologous HSCT. 100 CORD 8-year DFS = 92.3 (5.2) BM 8-year DFS = 75.5 (4.6) % (SE) 75 PBSC 8-year DFS = 53.0 (12.6) 50 P = 0.0035 25 0 0 2 4 6 8 10 Probability of 8-year EFS by subgroups Variable Cases 8-Year EFS s.e. Gender F M 107 136 63.3 74.0 5.4 3.9 46 27 92 78 58.2 61.2 65.4 69.8 7.6 9.4 6.8 5.0 96 112 35 76.2 67.0 57.9 4.6 5.2 8.7 16 40 45 39 67 4 25 7 68.7 55.4 76.2 69.8 71.9 100 63.3 85.7 11.6 9.4 6.6 9.1 5.6 − 9.8 13.2 24 219 73.3 70.2 11.8 3.5 4 239 50 65.8 25 4.8 45 198 72.6 68.6 6.8 3.7 18 225 55.0 70.9 11.9 3.4 102 141 62.8 73.1 4.9 4.0 58 45 30 8 73.8 84.0 73.5 49.6 6.3 5.5 9.2 18.6 180 26 37 67.2 92.3 62.7 3.8 5.2 9.1 P-value 0.14 0.81 Age o 1 year 1–2 year 2–10 year 4 10 year WBC count (x109/L) o 10 10–99 4 100 0.12 FAB M0 M1 M2 M4 M5 M6 M7 Unclassifiable/not known Subgroups FLT3-ITD Yes No FLT3-TKD Yes No 11q23 abnormalities Yes No Complex karyotype Yes No 0.71 0.51 0.54 0.86 0.13 0.06 Type of transplant AUTO ALLO 0.12 Type of donor MFD MUD MMUD HAPLO 0.06 Stem cell source BM Cord blood PBSC Years from HSCT 0.0035 Figure 5. Eight-year probability of DFS ( ± s.e.) for children with CR1 AML given allogeneic HSCT according to the stem cell source used. Stem cell source only for ALLO BM Cord blood PBSC 95 26 20 75.5 92.3 53.0 4.6 5.2 12.6 (s.e. 4.5) and 17.4% (s.e. 3.3) after AUTO- and ALLO-HSCT, respectively (P = 0.043, Figure 3). The median time to leukemia recurrence was 6.3 months (range 1.1–49.5). Relapse involved BM only in 42 patients, while either combined or isolated extramedullary relapse occurred in 6 and 3 patients, respectively. In the subgroup of patients given an allograft, the stem cell source employed did not influence the risk of leukemia recurrence (data not shown). Notably, only 2 out of the 26 children given CB transplantation experienced leukemia relapse, this translating into a CI of recurrence of only 7.7% (s.e. 5.2). By contrast, the CI of relapse in children transplanted from an HLA-identical sibling or Stem cell source only for UD BM Cord blood PBSC 39 26 10 74.5 92.3 50.0 6.7 5.2 21.2 aGVHD Yes No 82 59 74.8 76.1 5.1 5.9 aGVHD, grade II-IV Yes No 53 88 78.3 73.3 6.4 4.9 © 2015 Macmillan Publishers Limited 0.18 0.79 0.42 Bone Marrow Transplantation (2015) 181 – 188 Autologous and allogeneic HSCT in childhood AML F Locatelli et al 186 Table. 3. (Continued ) Variable Cases 8-Year EFS s.e. aGVHD, grade III-IV Yes No 19 122 72.3 75.7 12.6 4.0 cGVHD Yes No 33 106 81.9 74.6 7.6 4.4 Extensive cGVHD Yes No 11 128 61.4 78.3 15.3 3.8 P-value 0.87 0.23 0.31 Abbreviations: ALLO = allogeneic; AUTO = autologous; CNS = central nervous system; F = female; HAPLO = HLA-haploidentical HSCT; HSCT = hematopoietic SCT; M = male; MFD = matched family donor; MMUD = mismatched unrelated donor; MUD = matched unrelated donor; pts = patients. an adult UD was 18.6% (s.e. 5.3) and 17.2% (s.e. 5.6), respectively (P = ns). While there was no difference in terms of leukemia recurrence for children who did or did not experience aGVHD (data not shown), only 2 out of the 33 patients who experienced cGVHD relapsed, as compared to 19 of the 106 patients who did not develop this complication, the CI of relapse in patients with or without cGVHD being 6.1% (s.e. 4.1) and 19.4% (s.e. 4.0), respectively (P = 0.09). Overall and event-free survival The 8-year probability of OS for the whole cohort of patients was 75.1% (s.e. 3.0); it was 75.5% (s.e. 4.4) and 74.7% (s.e. 4.0) for patients given either AUTO- or ALLO-HSCT, respectively (P = ns). The 8-year DFS, calculated from the date of HSCT, for the 102 patients given an AUTO-HSCT was 63% (s.e. 4.9); it was 73% (s.e. 4.0) for the 141 patients given an allograft (P = ns; Figure 4). The 8year DFS for AUTO-HSCT recipients who did or did not receive in vitro purging was comparable (data not shown). The 8-year probability of DFS for patients transplanted from an HLA-identical sibling was 73.8% (s.e. 6.3); it was 75.5% (s.e. 4.6), 53% (s.e. 12.6) and 92.3% (s.e. 5.2) for patients given either BM, or PBSC from an unrelated volunteer or CB cells, respectively (overall P = 0.0035; Figure 5). Table 3 reports details on the influence of the different variables analyzed on the probability of 8-year DFS. None of the variables analyzed resulted to be significantly associated with DFS in multivariate analysis. Notably, out of the 29 patients who experienced relapse after AUTO-HSCT 11 are alive and disease-free after having received an ALLO-HSCT in CR2; in 5 out of these 11 patients, the donor was an HLA-haploidentical relative. DISCUSSION We report the outcome of children with HR-AML in CR1, who were given either AUTO- or ALLO-HSCT in the AIEOP AML 2002/01 study. We have previously demonstrated that a broad use of HSCT in this HR population is able to lower the CI of relapse to an extent comparable to that of SR children,17 suggesting that transplantation can abolish the detrimental impact mainly imparted by specific molecular lesions and poor response to therapy. More than 75% of the patients in CR1 enrolled in this study became long-term survivors, leukemia recurrence being the most important cause of treatment failure. The strength of our results lies on the fact that: (i) children were prospectively allocated to the Bone Marrow Transplantation (2015) 181 – 188 HR group according to consistent criteria of stratification; (ii) all patients received the same chemotherapy treatment for inducing and consolidating remission before transplantation; and (iii) they were given a homogenous conditioning regimen. Our data argue that, despite being used in children with more adverse prognostic features (see also Tables 1 and 3), ALLO-HSCT is more effective than AUTO-HSCT in preventing leukemia recurrence, without this positive effect being obscured by an increased risk of TRM. Indeed, both in AUTO- and in ALLO-HSCT the CI of TRM was 7%, a value which compares favorably with previously reported data on ALLO-HSCT,4,5,7,10 while it was worse than expected in AUTO-HSCT. In this regard, it has to be emphasized that more than a half of the fatal events were due to sinusoidal obstruction syndrome, a complication known to occur with increased incidence in patients given BU as part of the conditioning regimen.24 However, there is no obvious explanation why sinusoidal obstruction syndrome occurred only in AUTOHSCT recipients, although more Centers perform this type of transplantation in comparison to those involved in the ALLO-HSCT procedure. The final outcome of our patients transplanted from an UD did not differ from that of patients given HSCT from an HLA-identical sibling and the 8-year DFS of 73% observed in our cohort of UD HSCT recipients compares favorably with results reported in previously published studies.10,25,26 The outcome of children transplanted from UDs acquires particular value in light of the fact that this type of allograft was employed in patients either with poor-prognosis molecular lesions, such as FLT3-ITD, or in infants, or in children with M7-AML or complex karyotype or in those patients not responding to the first course of induction therapy, these subgroups notoriously predicting a grim prognosis.2,8,17,27,28 We and others have previously provided evidence that the outcome of children with acute lymphoblastic leukemia given HSCT from an UD has improved over time,12,13,26 and the present results confirm that currently, thanks to the improvements in HLA typing obtained through the use of high-resolution molecular techniques and the optimization of GVHD prevention and treatment, post-transplantation outcome is not influenced by the type of donor used, either related or unrelated. The outcome of children transplanted with CB cells is particularly remarkable, as the probability of DFS in this subgroup of patients overcomes 90%. Our data confirm and strengthen the data reported by Michel et al.11 on children with AML receiving single-unit CB transplantation after a myeloablative preparation. These data were recently updated by Ruggeri and Colleagues9 for the subgroup of infants with AML, in whom the reported 4-year DFS was 82% for those patients who were transplanted in CR1. The favorable outcome of children transplanted with CB cells was both due to a particularly low risk of TRM and to a CI of recurrence of only 7.7%. Previously published studies have reported that FLT3-ITD is an adverse prognostic factor in childhood AML.27,28 In particular, Meshinchi et al.27 reported that children with FLT3-ITD had a 4year progression-free survival and a CI of leukemia recurrence of 31% and 65%, respectively. The probability of OS in children with FLT3-ITD given an allograft from a matched family donor increased to 64%, thanks to reduced risk of leukemia recurrence. The 74% probability of 8-year DFS in our cohort confirms and extends the data by Meshinchi et al., as well as those of other published studies,29,30 documenting that ALLO-HSCT can supersede the negative prognostic impact of FLT3-ITD in AML. The 72% probability of 8-year DFS observed in our patients with 11q23 abnormalities mimics that reported by the I-BFM group in a recently published paper (71% at 5 years),7 this finding confirming that the subgroup of children with CR1 AML and MLL rearrangement has a high probability of benefiting from HSCT. In particular, the 17 children with t(9;11) had a DFS probability of 82%, while © 2015 Macmillan Publishers Limited Autologous and allogeneic HSCT in childhood AML F Locatelli et al 187 the 28 children carrying MLL rearrangements with other partner genes had a DFS probability of 65% (P = ns). The choice of adopting a preparative regimen consisting of 3 alkylating agents was inspired by studies demonstrating the safety and efficacy of this therapy in both AML and juvenile myelomonocytic leukemia.18,31 Since we transplanted patients in CR1, the risk of TRM and of leukemia recurrence in our allograft recipients (7% and 17%, respectively) are in line with those (12% and 33%, respectively) reported by Beier et al.32 in children with AML in CR2, after the same conditioning regimen. Moreover, preparative regimens before the allograft which do not include TBI are particularly attractive for children, since radiation-induced late effects may be especially deleterious for very-young children.33–35 The merits of using HSCT, in particular the autograft procedure, as consolidation therapy for pediatric patients with CR1 AML have been contested vigorously in the past years in light of the progress achieved with chemotherapy, and the risks inherent to the procedure have been advocated in support of restricting the use of transplantation.2,4 Moreover, growing attention has been paid to the emergence of the potentially severe side effects, including also cGVHD, correlated to the transplant procedure. These considerations must certainly be put forward also in our cohort of patients, which, however, did not include any child with acute promyelocytic leukemia or core-binding factor anomalies. As we previously reported,17 37 HR patients (11% of the whole HR population included in the AIEOP-2002/01 protocol) received neither AUTO- nor ALLO-HSCT at the end of consolidation therapy. These patients had a significantly worse outcome in comparison with those given HSCT. In the successor protocol, the AIEOP group will not use AUTOHSCT and will restrict the indications to ALLO-HSCT to a population of patients (40–45% of the total number of children with AML other than acute promyelocytic leukemia instead of the 75–80% of patients who were given HSCT in the protocol AIEOP 2002/01) with biological and treatment-related characteristics predicting poor outcome if treated with chemotherapy only (see Pession et al.17 and Hasle36 for details). In conclusion, our data document that both AUTO- and ALLOHSCT, after a preparative regimen consisting of BU, CY and melphalan, offer a chance of cure for a large proportion of children with AML in CR1. Disease recurrence remains the major cause of treatment failure, and strategies to reduce the risk of relapse are warranted. In the future, the role of HSCT in the treatment of children and adolescents with AML in CR1 will need to be reassessed as the field evolves. In this regard, a more refined selection of children candidate to receive transplantation in CR1 based on genetic parameters, such as monosomy 7, complex karyotype, FLT3-ITD, so on1,2,36–39 and response to initial treatment through the use of flow cytometry for measuring minimal residual disease36,40 can contribute to further improve patient’s outcome and to spare long-term side effects associated with the transplant procedure. CONFLICT OF INTEREST The authors declare no conflict of interest. ACKNOWLEDGEMENTS This study was supported by research grants awarded by Associazione Italiana per la Ricerca sul Cancro (5 x 1000 Special Grant #9962 to FL), by PRIN (Progetti di Rilevante Interesse Nazionale) 2010 to FL and 2012 to SR, by Ospedale Bambino Gesù, Roma, (Progetto di Ricerca Corrente 2012–2013) to AB and FL, and FILAS (Adult Stem Cells) to SR. LIST OF PARTICIPATING CENTERS AND INVESTIGATORS Department of Pediatric Onco-Hematology, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Policlinico San Matteo © 2015 Macmillan Publishers Limited Foundation, Pavia. Franco Locatelli (till January 2010), Marco Zecca, Giovanna Giorgiani [38 HSCT].Department of Pediatric Hematology-Oncology, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Bambino Gesù Children's Hospital, Roma. Franco Locatelli (since January 2010), Alice Bertaina, Maurizio Caniglia, Giuseppe Palumbo, Sergio Rutella [30 HSCT]. Department of Pediatric Hematology and Oncology, University of Padova, Padova. Chiara Messina, Marta Pillon [29 HSCT]. Department of Pediatric Hematology, San Gerardo Hospital, Monza. Adriana Balduzzi, Attilio Rovelli [27 HSCT]. BMT Unit, Department of Pediatric Hemato-Oncology, Santobono-Pausilipon Hospital, Napoli. Mimmo Ripaldi [24 HSCT]. Department of Pediatric Hematology Oncology, IRCCS G. Gaslini Institute, Genova. Edoardo Lanino, Giorgio Dini [23 HSCT]. Pediatric Onco-Hematology, Stem Cell Transplantation and Cellular Therapy Division, Regina Margherita Children's Hospital, Torino. Franca Fagioli [15 HSCT]. Pediatric Oncology and Hematology Unit ‘Lalla Seragnoli’, Department of Pediatrics, University of Bologna Sant’OrsolaMalpighi Hospital, Bologna. Riccardo Masetti, Arcangelo Prete, Andrea Pession [12 HSCT]. Department of Pediatrics, University of Pisa, Pisa. Claudio Favre [9 HSCT]. Pediatric Hematology/Oncology, ARNAS Ospedale Civico di Palermo. Ottavio Ziino, Paolo D’Angelo [8 HSCT]. Pediatric Hematology/Oncology, University Hospital, Catania. Luca Lo Nigro [8 HSCT]. BMT Unit, Ospedale di Pescara. Paolo Di Bartolomeo [6 HSCT]. BMT Unit, Ospedale Pediatrico Burlo Garofalo, Trieste. Marco Rabusin [6 HSCT]. BMT Unit, Department of Pediatric Hematology/Oncology, Ospedale Pediatrico Meier, Florence. Desiree Caselli [5 HSCT]. BMT Unit, Pediatric Hematology/Oncology, Ospedale Silvestrini, Perugia. Franco Aversa [3 HSCT]. AUTHOR CONTRIBUTIONS FL designed the study, interpreted data, performed transplantation and wrote the article; RM designed the study, checked data and performed transplantation; RR analyzed data; MZ, FF, AR, CM and EL designed the study, performed transplantation and followed patients; AB, CF, GG, MR, GP, MP and OZ performed transplantation and followed patients; AP designed the study, performed transplantation and interpreted the data; SR interpreted the data and wrote the paper; ArPr contributed to study design, interpreted the data and performed transplantation. REFERENCES 1 Pui CH, Carroll WL, Meshinchi S, Arceci RJ. Biology, risk stratification, and therapy of pediatric acute leukemias: an update. J Clin Oncol 2011; 29: 551–565. 2 Creutzig U, van den Heuvel-Eibrink MM, Gibson B, Dworzak MN, Adachi S, de Bont E et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood 2012; 120: 3187–3205. 3 Kaspers GJ, Zwaan CM. Pediatric acute myeloid leukemia: towards high-quality cure of all patients. Haematologica 2007; 92: 1519–1532. 4 Niewerth D, Creutzig U, Bierings MB, Kaspers GJ. A review on allogeneic stem cell transplantation for newly diagnosed pediatric acute myeloid leukemia. Blood 2010; 116: 2205–2214. 5 Woods WG, Neudorf S, Gold S, Sanders J, Buckley JD, Barnard DR et al. A comparison of allogeneic bone marrow transplantation, autologous bone marrow transplantation, and aggressive chemotherapy in children with acute myeloid leukemia in remission. Blood 2001; 97: 56–62. 6 Amadori S, Testi AM, Arico M, Comelli A, Giuliano M, Madon E et al. Prospective comparative study of bone marrow transplantation and postremission chemotherapy for childhood acute myelogenous leukemia. The Associazione Italiana Ematologia ed Oncologia Pediatrica Cooperative Group. J Clin Oncol 1993; 11: 1046–1054. 7 Klusmann JH, Reinhardt D, Zimmermann M, Kremens B, Vormoor J, Dworzak M et al. The role of matched sibling donor allogeneic stem cell transplantation in pediatric high-risk acute myeloid leukemia: results from the AML-BFM 98 study. Haematologica 2012; 97: 21–29. 8 Horan JT, Alonzo TA, Lyman GH, Gerbing RB, Lange BJ, Ravindranath Y et al. Impact of disease risk on efficacy of matched related bone marrow Bone Marrow Transplantation (2015) 181 – 188 Autologous and allogeneic HSCT in childhood AML F Locatelli et al 188 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 transplantation for pediatric acute myeloid leukemia: the Children's Oncology Group. J Clin Oncol 2008; 26: 5797–5801. Ruggeri A, Volt F, Michel G, Diaz de Heredia C, Abecasis M, Zecca M et al. Unrelated cord blood transplantation for infant acute leukemia diagnosed within 1 year of age: outcomes and risk factor analysis on behalf of Eurocord and PDWP-EBMT. Blood 2013; 122: 160-. Eapen M, Rubinstein P, Zhang MJ, Stevens C, Kurtzberg J, Scaradavou A et al. Outcomes of transplantation of unrelated donor umbilical cord blood and bone marrow in children with acute leukaemia: a comparison study. Lancet 2007; 369: 1947–1954. Michel G, Rocha V, Chevret S, Arcese W, Chan KW, Filipovich A et al. Unrelated cord blood transplantation for childhood acute myeloid leukemia: a Eurocord Group analysis. Blood 2003; 102: 4290–4297. Locatelli F, Zecca M, Messina C, Rondelli R, Lanino E, Sacchi N et al. Improvement over time in outcome for children with acute lymphoblastic leukemia in second remission given hematopoietic stem cell transplantation from unrelated donors. Leukemia 2002; 16: 2228–2237. Dini G, Zecca M, Balduzzi A, Messina C, Masetti R, Fagioli F et al. No difference in outcome between children and adolescents transplanted for acute lymphoblastic leukemia in second remission. Blood 2011; 118: 6683–6690. Bonetti F, Zecca M, Pession A, Messina C, Montagna D, Lanino E et al. Total-body irradiation and melphalan is a safe and effective conditioning regimen for autologous bone marrow transplantation in children with acute myeloid leukemia in first remission. The Italian Association for Pediatric Hematology and OncologyBone Marrow Transplantation Group. J Clin Oncol 1999; 17: 3729–3735. Zittoun R A, Mandelli F, Willemze R, de Witte T, Labar B, Resegotti L et al. Autologous or allogeneic bone marrow transplantation compared with intensive chemotherapy in acute myelogenous leukemia. European Organization for Research and Treatment of Cancer (EORTC) and the Gruppo Italiano Malattie Ematologiche Maligne dell'Adulto (GIMEMA) Leukemia Cooperative Groups. N Engl J Med 1995; 332: 217–223. Ravindranath Y, Yeager AM, Chang MN, Steuber CP, Krischer J, Graham-Pole J et al. Autologous bone marrow transplantation versus intensive consolidation chemotherapy for acute myeloid leukemia in childhood. Pediatric Oncology Group. N Engl J Med 1996; 334: 1428–1434. Pession A, Masetti R, Rizzari C, Putti MC, Casale F, Fagioli F et al. Results of the AIEOP AML 2002/01 multicenter prospective trial for the treatment of children with acute myeloid leukemia. Blood 2013; 122: 170–178. Locatelli F, Pession A, Bonetti F, Maserati E, Prete L, Pedrazzoli P et al. Busulfan, cyclophosphamide and melphalan as conditioning regimen for bone marrow transplantation in children with myelodysplastic syndromes. Leukemia 1994; 8: 844–849. Glucksberg H, Storb R, Fefer A, Buckner CD, Neiman PE, Clift RA et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 1974; 18: 295–304. Storb R, Prentice RL, Sullivan KM, Shulman HM, Deeg HJ, Doney KC et al. Predictive factors in chronic graft-versus-host disease in patients with aplastic anemia treated by marrow transplantation from HLA-identical siblings. Ann intern Med 1983; 98: 461–466. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med 1999; 18: 695–706. Zhang X, Zhang MJ, Fine J. A proportional hazards regression model for the subdistribution with right-censored and left-truncated competing risks data. Stat Med 2011; 30: 1933–1951. Reeves GK, Cox DR, Darby SC, Whitley E. Some aspects of measurement error in explanatory variables for continuous and binary regression models. Stat Med 1998; 17: 2157–2177. Bone Marrow Transplantation (2015) 181 – 188 24 Dignan FL, Wynn RF, Hadzic N, Karani J, Quaglia A, Pagliuca A et al. BCSH/BSBMT guideline: diagnosis and management of veno-occlusive disease (sinusoidal obstruction syndrome) following haematopoietic stem cell transplantation. Brit J Haematol 2013; 163: 444–457. 25 Kelly MJ, Horan JT, Alonzo TA, Eapen M, Gerbing RB, He W et al. Comparable survival for pediatric acute myeloid leukemia with poor-risk cytogenetics following chemotherapy, matched related donor, or unrelated donor transplantation. Pediatri Blood Cancer 2014; 61: 269–275. 26 Eapen M, Rubinstein P, Zhang MJ, Camitta BM, Stevens C, Cairo MS et al. Comparable long-term survival after unrelated and HLA-matched sibling donor hematopoietic stem cell transplantations for acute leukemia in children younger than 18 months. J Clin Oncol 2006; 24: 145–151. 27 Meshinchi S, Arceci RJ, Sanders JE, Smith FO, Woods WB, Radich JP et al. Role of allogeneic stem cell transplantation in FLT3/ITD-positive AML. Blood 2006; 108: 400. 28 Staffas A, Kanduri M, Hovland R, Rosenquist R, Ommen HB, Abrahamsson J et al. Presence of FLT3-ITD and high BAALC expression are independent prognostic markers in childhood acute myeloid leukemia. Blood2011; 118: 5905–5913. 29 Levis M, Small D. FLT3: ITDoes matter in leukemia. Leukemia 2003; 17: 1738–1752. 30 DeZern A E, Sung A, Kim S, Smith B D, Karp J E, Gore S D et al. Role of allogeneic transplantation for FLT3/ITD acute myeloid leukemia: outcomes from 133 consecutive newly diagnosed patients from a single institution. Biol Blood Marrow Transplant 2011; 17: 1404–1409. 31 Locatelli F, Nollke P, Zecca M, Korthof E, Lanino E, Peters C et al. Hematopoietic stem cell transplantation (HSCT) in children with juvenile myelomonocytic leukemia (JMML): results of the EWOG-MDS/EBMT trial. Blood 2005; 105: 410–419. 32 Beier R, Albert MH, Bader P, Borkhardt A, Creutzig U, Eyrich M et al. Allo-SCT using BU, CY and melphalan for children with AML in second CR. Bone Marrow Transplant 2013; 48: 651–656. 33 Giorgiani G, Bozzola M, Locatelli F, Picco P, Zecca M, Cisternino M et al. Role of busulfan and total body irradiation on growth of prepubertal children receiving bone marrow transplantation and results of treatment with recombinant human growth hormone. Blood 1995; 86: 825–831. 34 Michel G, Gluckman E, Esperou-Bourdeau H, Reiffers J, Pico JL, Bordigoni P et al. Allogeneic bone marrow transplantation for children with acute myeloblastic leukemia in first complete remission: impact of conditioning regimen without total-body irradiation—a report from the Societe Francaise de Greffe de Moelle. J Clin Oncol 1994; 12: 1217–1222. 35 Parth P, Dunlap WP, Kennedy RS, Ordy JM, Lane NE. Motor and cognitive testing of bone marrow transplant patients after chemoradiotherapy. Percept Mot Skills 1989; 68: 1227–1241. 36 Hasle H. A critical review of which children with acute myeloid leukaemia need stem cell procedures. Brit J Haematol 2014; 166: 23–33. 37 Masetti R, Pigazzi M, Togni M, Astolfi A, Indio V, Manara E et al. CBFA2T3-GLIS2 fusion transcript is a novel common feature in pediatric, cytogenetically normal AML, not restricted to FAB M7 subtype. Blood 2013; 121: 3469–3472. 38 von Neuhoff C, Reinhardt D, Sander A, Zimmermann M, Bradtke J, Betts DR et al. Prognostic impact of specific chromosomal aberrations in a large group of pediatric patients with acute myeloid leukemia treated uniformly according to trial AML-BFM 98. J Clin Oncol 2010; 28: 2682–2689. 39 Balgobind BV, Van den Heuvel-Eibrink MM, De Menezes RX, Reinhardt D, Hollink IH, Arentsen-Peters ST et al. Evaluation of gene expression signatures predictive of cytogenetic and molecular subtypes of pediatric acute myeloid leukemia. Haematologica 2011; 96: 221–230. 40 Rubnitz JE, Inaba H, Dahl G, Ribeiro RC, Bowman WP, Taub J et al. Minimal residual disease-directed therapy for childhood acute myeloid leukaemia: results of the AML02 multicentre trial. Lancet Oncol 2010; 11: 543–552. © 2015 Macmillan Publishers Limited
© Copyright 2025 Paperzz