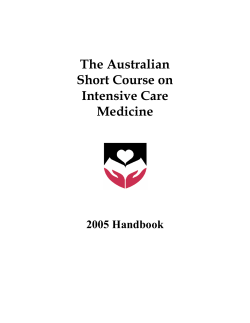
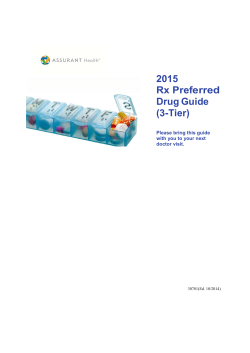
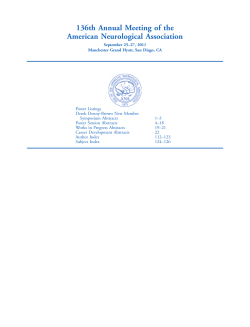
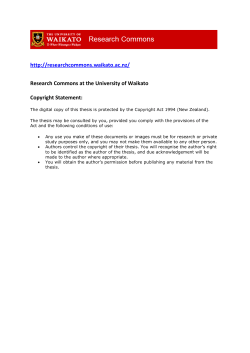
Volume 357 — August 9, 2007 — Number 6,pp.525-628 Article Summaries Immigrants and Health Care — At the Intersection of Two Broken Systems S. Okie Becoming a Physician: Terra Firma — A Journey from Migrant Farm Labor to Neurosurgery A. QuiГ±ones-Hinojosa Pay for Performance, Version 2.0? T. H. Lee Prophylaxis versus Episodic Treatment to Prevent Joint Disease in Boys with Severe Hemophilia M. J. Manco-Johnson and Others A Single Cycle of Rituximab for the Treatment of Severe Pemphigus P. Joly and Others Complement C3 Variant and the Risk of Age-Related Macular Degeneration J. R.W. Yates and Others NXY-059 for the Treatment of Acute Ischemic Stroke A. Shuaib and Others Acute Ischemic Stroke H. B. van der Worp and J. van Gijn Current Concepts: Drug-Induced Immune Thrombocytopenia R. H. Aster and D. W. Bougie Intravesical Foreign Body N. Mondaini and R. Bartoletti Asymptomatic Bladder Stones Y. Daneshbod Case 24-2007 — A 20-Year-Old Pregnant Woman with Altered Mental Status A. J. Cole, J. W. Henson, M. H.A. Roehrl, and M. P. Frosch Safer Drugs for the American People G. D. Curfman, S. Morrissey, and J. M. Drazen Prophylactic Treatment for Prevention of Joint Disease in Hemophilia — Cost versus Benefit G. Roosendaal and F. Lafeber Rituximab and Pemphigus — A Therapeutic Advance L. A. Diaz The Tension between Needing to Improve Care and Knowing How to Do It A. D. Auerbach, C. S. Landefeld, and K. G. Shojania Adjunctive Antidepressant Treatment for Bipolar Depression Glucose Regulation in Young Adults with Very Low Birth Weight Use of Physicians' Services for Medicare Beneficiaries Video on Orotracheal Intubation Case 14-2007: A Man with Pain and Swelling of Both Eyes and the Right Ear Pregnancy in a Patient with Congenital Erythropoietic Porphyria Preventing Medication Errors Medication Errors Medical Management of Vulnerable and Underserved Patients: Principles, Practice, and Populations New and Evolving Infections of the 21st Century Vaccine: The Controversial Story of Medicine's Greatest Lifesaver The n e w e ng l a n d j o u r na l of m e dic i n e images in clinical medicine Asymptomatic Bladder Stones A  healthy 26-year-old driver had routine laboratory tests performed to renew his driver’s license. Hematuria (3+) was incidentally noted. He reported having had no urinary tract symptoms. Abdominal radiography of the kidneys, ureters, and bladder showed large bladder stones (Panel A, with a Foley catheter tube visible). During cystotomy, two large stones, measuring 8 cm and 3 cm in diameter, were removed (Panel B). These stones were found to contain both calcium phosphate and uric acid and were infected with Proteus mirabilis. No structural bladder-outlet obstruction or other anatomical abnormalities were identified. The patient recovered quickly from the surgery and was discharged 2 days after the procedure. The infection was treated with 500 mg of ciprofloxacin twice daily. Whereas a small stone (only millimeters in size) often causes significant pain as it travels through a narrow ureter, bladder calculi may become large and yet not cause symptoms. A Copyright В© 2007 Massachusetts Medical Society. Yahya Daneshbod, M.D. Dr. Daneshbod Pathology Laboratory Shiraz 71347, Iran daneshbk@yahoo.com B ICM n engl j med 357;6  www.nejm.org  august 9, 2007 RETAKE 1st AUTHOR Daneshbod REG F FIGURE CASE TITLE EMail Enon 2nd 3rd a&b Line 4-C Revised SIZE e The NEW ENGLA ND JOURNAL of MEDICINE Perspective august 9, 2007 Immigrants and Health Care — At the Intersection of Two Broken Systems Susan Okie, M.D. A t a primary care clinic in Montgomery County, Maryland, where I volunteer, the patients are uninsured immigrants from Latin America or West Africa. Many are day laborers, house cleaners, or construction workers; most do not speak English. Several months ago, I saw a middle-aged Hispanic baker with profound weakness, fatigue, limb swelling, and severe muscle pain, who had to be hospitalized for myxedema. Fortunately, a local charity agreed to pay most of her hospital costs, and she’s now receiving thyroid hormone–replacement therapy — but with regular care, her hypothyroidism could have been diagnosed earlier and hospitalization averted. Another day, I tried to persuade a reticent West African man who had been tortured in prison that psychological counseling might help his chronic pain. However, mental health services for uninsured immigrants are sparse, and the man was reluctant to venture to a distant part of Washington, D.C., to a program for torture survivors. A third patient, a man in his 40s, came in with a nearly empty bottle of eyedrops, which he had brought from Ghana to take for glaucoma. The disease had already blinded him in one eye, and the vision in his other eye had been fluctuating. He needed a complete eye exam and visual-field testing, but arranging timely referrals to specialists is often difficult for caregivers treating the uninsured. I wrote him a prescription, and we managed to set up an appointment at a hospital-based ophthalmology clinic that ac- cepts a limited number of uninsured patients. For recent immigrants — especially the estimated 12 million who are here illegally — seeking health care often involves daunting encounters with a fragmented, bewildering, and hostile system. The reason most immigrants come here is to work and earn money; on average, they are younger and healthier than native-born Americans, and they tend to avoid going to the doctor. Many work for employers who don’t offer health insurance, and they can’t afford insurance premiums or medical care. They face language and cultural barriers, and many illegal immigrants fear that visiting a hospital or clinic may draw the attention of immigration officials. Although anti-immigrant sentiment is fueled by the belief that immigrants can obtain federal benefits, 1996 welfare-reform legislation greatly restricted im- n engl j med 357;6  www.nejm.org  august 9, 2007 525 PERSPE C T I V E Immigrants and Health Care — At the Intersection of Two Broken Systems migrants’ access to programs such as Medicaid, shifting most health care responsibility to state and local governments. The law requires that immigrants wait 5 years after obtaining lawful permanent residency (a “green card”) to apply for federal benefits. In response, some states and localities — for instance, Illinois, New York, the District of Columbia, and certain California counties — have used their own funds to expand health insurance coverage even for undocumented immigrant children and pregnant women with low incomes. Other states, however, such as Arizona, Colorado, Georgia, and Virginia, have passed laws making it even more difficult for noncitizens to gain access to health services. Whether or not they have health insurance, immigrants overall have much lower per capita health care expenditures than native-born Americans,1 and recent analyses indicate that they contribute more to the economy in taxes than they receive in public benefits. In a study from the RAND Corporation, researchers estimated that undocumented adult immigrants, who make up about 3.2% of the population, account for only about 1.5% of U.S. medical costs.2 Many immigrants do not seek medical treatment unless they are injured or acutely ill; at our clinic, patients with type 2 diabetes often have florid symptoms and even incipient renal damage by the time their disease is diagnosed. One study found that annual per capita expenses for health care were 86% lower for uninsured immigrant children than for uninsured U.S.-born children — but emergency department expenditures were more than 526 three times as high.1 Although U.S. hospitals must provide emergency care without first asking about income, insurance, or citizenship, early diagnosis and treatment in a primary care setting are both medically preferable and a better use of resources. “If people keep postponing medical care because they’re so concerned about being sent back over the border,” noted Elizabeth Benson Forer, executive director of the Venice Family Clinic, a venerable free clinic in Los Angeles that serves many immigrants, “then you can end up with some pretty horrendous health situations.” Immigrants live, work, and attend school in communities throughout the country; laws and bureaucratic barriers that reduce their use of key preventive health services, such as immunizations and screenings for infectious disease, make for bad public health policy, and denying immigrants primary care ultimately increases health care costs for everyone. For example, labor and delivery costs for undocumented immigrant women are covered under the federal and state emergency Medicaid program, but most states do not cover prenatal care, and there is no coverage for family planning. Some of my patients say they would like to use oral contraceptives or an intrauterine device or undergo a tubal ligation, but they can’t afford it. And immigrants, like native-born Americans, are vulnerable to chronic diseases; as my colleague, nurse practitioner Lois Wessel, notes, “Even the 25-year-old day laborers are eventually going to become 45-year-olds, probably still undocumented, with hypertension and diabetes.  .  .  .  Life in America is going to make them become not so healthy.” Recently, a bipartisan group of U.S. senators, with White House support, introduced an immigration bill that offered the best chance in years of achieving substantial reform of a dysfunctional system. However, the bill met with opposition from both conservatives and liberals and was killed in the Senate this past June, quashing all hope of immigration reform during the current administration. State legislatures this year are considering a record number of anti-immigrant measures, and the Senate bill’s demise heightens their chances of passage. “You will see the states and cities scrambling to pass their own laws and regulations, and you’re going to get a completely contradictory set of policies,” Senator John McCain (R-AZ) predicted in a Washington Post article on July 8. In many areas of the country, one consequence is likely to be reduced access to health care for immigrants. Noncitizens make up about 20% of the 46 million uninsured people in the United States. Hospitals generally do not collect information on patient immigration status, and there are no reliable national figures on hospital costs for undocumented immigrants. Nevertheless, the soaring cost of uncompensated care (see graph A) has made the problem of providing care for uninsured immigrants a hot political issue, particularly in border states and those (such as the southeastern states) whose immigrant populations have grown rapidly in recent years. Some uninsured immigrants needing emergency treatment (including pregnant women, children, adults n engl j med 357;6  www.nejm.org  august 9, 2007 Immigrants and Health Care — At the Intersection of Two Broken Systems Cost of Uncompensated Hospital Care (billions of $) 30 25 20 15 10 5 0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2002 2003 2004 2005 Year B 13 12 11 10 9 8 7 6 5 4 3 2 1 0 1996 1997 1998 1999 2000 2001 Year C 50 47 48 47 46 45 44 43 42 41 40 39 6 5 20 05 –2 00 00 4 –2 20 04 00 3 –2 03 20 –2 00 02 20 –2 00 2 1 00 20 01 0 00 20 00 –2 9 99 99 –2 19 8 19 98 –1 99 7 –1 99 19 97 –1 96 19 95 –1 99 6 0 19 with dependent children, and elderly, blind, or disabled patients with incomes below Medicaid thresholds) qualify for emergency Medicaid coverage. In many other cases, hospitals receive no payment for their care, although in 2003 Congress appropriated $250 million per year for 4 years (starting in 2005) to partially compensate hospitals for treating undocumented immigrants. A recent study found that although emergency Medicaid spending for immigrants in North Carolina grew by 28% between 2001 and 2004, it still represented less than 1% of the state’s Medicaid budget.3 More than 80% of that spending was for childbirth and complications of pregnancy, and major injuries accounted for nearly one third of the rest. In California, emergency Medicaid spending for uninsured immigrants for fiscal year 2007 exceeded $941 million, according to Kim BelshГ©, secretary of the California Health and Human Services Agency. “Clearly, there are medical needs faced by this population,” said BelshГ©, “and the emergency room is not the most cost-effective A Estimated No. of Unauthorized Immigrants Living in the U.S. (millions) Cost of Uncompensated Care (Panel A), Number of Unauthorized Immigrants (Panel B), and Number of Uninsured People (Panel C) in the United States. The annual cost to U.S. hospitals of uncompensated care (charity care plus bad debt) has been rising, although the fraction of total hospital expenses represented by such care has remained relatively constant at about 5 to 6% since 1980. The number of unauthorized immigrants present in the United States has also been increasing, although the estimates are uncertain. Treatment of unauthorized immigrants contributes to uncompensated care costs, but the main reason such costs are increasing is the rise in the number of people who lack health insurance. Immigrants represent only about 20% of the uninsured. Data on uncompensated care are from the American Hospital Association; data on unauthorized immigrants are from the Pew Hispanic Center; data on the uninsured are from the U.S. Census Bureau. No. of People Not Covered by Health Insurance (millions) PERSPECTIVE Year place for [addressing] them.” In addition, undocumented immiAUTHOR: Okie ICM grants may account for as much REG F FIGURE 1 of 1 as $750 million annually of the CASE cost of uncompensated care in California hospitals — about 10% of theRETAKE annual1st total — since 2nd they represent about 3rd 10% of the Revised Line 4-C SIZE ARTIST: ts H/T H/T Enon Combo n engl j med 357;6  www.nejm.org  august 9, 2007 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. EMail JOB: 35706 ISSUE: 08-09-07 527 PERSPE C T I V E Immigrants and Health Care — At the Intersection of Two Broken Systems state’s emergency department patients, according to Jan Emerson, vice president of external affairs for the California Hospital Association. “Almost half of the hospitals in California are currently operating in the red,” she said. “It would not be fair to place the blame solely on undocumented immigrants, but certainly, they are a contributing factor.” The chief sources of outpatient care for uninsured immigrants are public clinics and community health centers. Such clinics are often sparse in suburban and rural areas that have recently faced an influx of immigrants. Even in cities with strong community-clinic networks and a long history of serving immigrants, access to care is uneven. For example, at the Venice Family Clinic, a bilingual nurse educator runs health and exercise classes in Spanish and English for patients with diabetes, pregnant women receive free state-subsidized prenatal care, and there are regularly scheduled clinic sessions for victims of torture and human trafficking. Yet arranging specialty referrals is a constant challenge — it usually entails sending patients to outpatient clinics at county hospitals, where some have to wait as long as a year for an appointment. In the Washington, D.C., area uninsured women, including undocumented immigrants, can get free annual mammograms and Pap smears through subsidized cancer-screening programs, but follow-up treatment for abnormal findings other than cancer is usually not included, and many clients have no source of primary care, as noted by nurse practitioner Wessel, who works monthly at one such pro528 gram. “Patients come in year after year” for Pap smears — “but they’ve never had their blood pressure checked,” she said. “We don’t check it, because all we’re financed to do is cervical- and breast-cancer screening.” In states seeking to expand insurance coverage, the question of including undocumented immigrants is a thorny one. About 1 million of California’s 4.8 million uninsured residents are undocumented adults, and about 136,000 are undocumented children.4 As part of a proposal for comprehensive health care reform, Governor Arnold Schwarzenegger is seeking to provide health insurance coverage (through Medicaid and the State Children’s Health Insurance Program, or SCHIP) to all children with family incomes at or below 300% of the federal poverty level, regardless of immigration status. Although there is considerable public support for insuring undocumented immigrant children, Republican state legislators “do not believe that state general fund revenues should be invested in people who are here illegally,” said health secretary BelshГ© — “and that extends to children.” The federal Medicaid program has always been restricted to U.S. citizens and legal residents, but recent federal and state laws designed to strengthen enforcement of eligibility rules have created new barriers, even for infants and children who are citizens, and have had a chilling effect on other programs providing health services for immigrants. The 2005 Deficit Reduction Act requires all persons applying for or renewing Medicaid coverage to provide proof of identity and U.S. citi- zenship. Since that law went into effect, at least eight states have reported dramatic declines in Medicaid enrollment, and some Medicaid-eligible infants and children have gone without immunizations and needed medical care because of delays in coverage.5 In Georgia, which last year passed a law requiring immigrants to show proof of legal residency in many situations, “we’ve started seeing a lot of kids not going to the doctor,” said Flavia Mercado, a pediatrician who runs the International Medical Center at Atlanta’s Grady Memorial Hospital. “A lot of my clients are leaving and going to other states, and a couple are even going back to their country. Everyone is very fearful.” She said that Atlanta organizations are scaling back health services for Hispanics and have stopped sponsoring Hispanic health fairs, fearing that they will be raided by police or immigration officials. Meanwhile, faced with rising health care costs and increasing numbers of uninsured persons, the state’s Medicaid program has sharply reduced benefits: it recently stopped paying for prenatal care for high-risk women and for nonemergency hemodialysis. Although immigrants make up a minority of the uninsured, Mercado said media reports regularly blame illegal immigrants for the worsening problems of the state’s health care system. Anger over high medical costs and reduced access to care no doubt contributes to anti-immigrant sentiment; the remedy, however, is not immigrant bashing, but health care reform. “As an American citizen, I understand that you want to n engl j med 357;6  www.nejm.org  august 9, 2007 PERSPECTIVE Immigrants and Health Care — At the Intersection of Two Broken Systems make sure the resources are there for the right people,” Mercado said. “Yet how can you deny someone health access? If we don’t treat and prevent illness  .  .  .  our whole community is going to suffer.” Dr. Okie is a contributing editor of the Journal. 1. Mohanty SA, Woolhandler S, Himmelstein DU, Pati S, Carrasquillo O, Bor DH. Health care expenditures of immigrants in the United States: a nationally representative analysis. Am J Public Health 2005;95:1431-8. 2. Goldman DP, Smith JP, Sood N. Immigrants and the cost of medical care. Health Aff (Millwood) 2006;25:1700-11. 3. DuBard CA, Massing MW. Trends in emergency Medicaid expenditures for recent and undocumented immigrants. JAMA 2007;297: 1085-92. [Erratum, JAMA 2007;297:1774.] 4. Brown ER, Pourat N, Wallace SP. Undocumented residents make up small share of California’s uninsured population. Los Angeles: UCLA Center for Health Policy Research, March 2007. 5. Pear R. Lacking papers, citizens are cut from Medicaid. New York Times. March 12, 2007:A1. Copyright В© 2007 Massachusetts Medical Society. BECOMING A PHYSICIAN Terra Firma — A Journey from Migrant Farm Labor to Neurosurgery Alfredo QuiГ±ones-Hinojosa, M.D. “ You will spend the rest of your life working in the fields,” my cousin told me when I arrived in the United States in the mid-1980s. This fate indeed appeared likely: a 19year-old illegal migrant farm worker, I had no English language skills and no dependable means of support. I had grown up in a small Mexican farming community, where I began working at my father’s gas station at the age of 5. Our family was poor, and we were subject to the diseases of poverty: my earliest memory is of my infant sister’s death from diarrhea when I was 3 years old. But my parents worked long hours and had always made enough money to feed us, until an economic crisis hit our country in the 1970s. Then they could no longer support the family, and although I trained to be a teacher, I could not put enough food on the table either. Desperate for a livable in- come, I packed my few belongings and, with $65 in my pocket, crossed the U.S. border illegally. The first time I hopped the fence into California, I was caught eating anything I could get, with hands bloodied from pulling weeds — the very same hands that today perform brain surgery. My days as a farm worker and sent back to Mexico, but I tried again and succeeded. I am not condoning illegal immigration; honestly, at the time, the law was far from the front of my mind. I was merely responding to the dream of a better life, the hope of escaping poverty so that one day I could return home triumphant. Reality, however, posed a stark contrast to the dream. I spent long days in the fields picking fruits and vegetables, sleeping under leaky camper shells, taught me a great deal about economics, politics, and society. I learned that being illegal and poor in a foreign country could be more painful than any poverty I had previously experienced. I learned that our society sometimes treats us differently depending on the places we have been and the education we have obtained. When my cousin told me I would never escape that life of poverty, I became determined to prove him wrong. I took night n engl j med 357;6  www.nejm.org  august 9, 2007 529 PERSPE C T I V E Terra Firma — A Journey from Migrant Farm Labor to Neurosurgery jobs as a janitor and subsequently as a welder that allowed me to attend a community college where I could learn English. In 1989, while I was working for a railroad company as a welder and high-pressure valve specialist, I had an accident that caused me to reevaluate my life once again. I fell into a tank car that was used to carry liquefied petroleum gas. My father was working at the same company. Hearing a coworker’s cry for help, he tried to get into the tank; fortunately, someone stopped him. It was my brother-in-law, Ramon, who climbed in and saved my life. He was taken out of the tank unconscious but regained consciousness quickly. By the time I was rescued, my heart rate had slowed almost to zero, but I was resuscitated in time. When I awoke, I saw a person dressed all in white and was flooded with a sense of security, confidence, and protection, knowing that a doc- 530 tor was taking care of me. Although it was clear to me that our poverty and inability to speak English usually translated into suboptimal health care for my community, the moment I saw this physician at my bedside, I felt I had reached terra firma, that I had a guardian. After community college, I was accepted at the University of California, Berkeley, where a combination of excellent mentorship, scholarships, and my own passion for math and science led me to research in the neurosciences. One of my mentors there convinced me, despite my skepticism, that I could go anywhere I wanted for medical school. Thanks to such support and encouragement, I eventually went to Harvard Medical School. As I pursued my own education, I became increasingly aware of the need and responsibility we have to educate our country’s poor. It is no secret that minority communities have the highest dropout rates and the lowest educational achievement levels in the country. The pathway to higher education and professional training programs is not “primed” for minority students. In 1994, when I started medical school, members of minority groups made up about 18% of the U.S. population but accounted for only 3.7% of the faculty in U.S. medical schools. I was very fortunate to find outstanding minority role models, but though their quality was high, their numbers were low. Given my background, perhaps it is not surprising that I did not discover the field of neurosurgery until I was a medical student. I vividly remember when, in my third year of medical school, I first witnessed neurosurgeons peeling back the dura and exposing a real, live, throbbing human brain. I recall feeling absolute awe and humility — and an immediate and deep recognition of the intimacy between a patient and a doctor. That year, one of my professors strongly encouraged me to go into primary care, arguing that it was the best way for me to serve my Hispanic immigrant community. Although I had initially intended to return to Mexico triumphant, I had since fallen in love with this country, and I soon found myself immersed in and committed to the betterment of U.S. society. With my sights set on neurosurgery after medical school, I followed my heart and instincts and have tried to contribute to my community and the larger society in my own way. I see a career in academic medicine as an opportunity not only to improve our understanding and treatment of human diseases but also to provide leadership within medicine and support to future scientists, medical students, and physician scientists from minority and nonminority groups alike. n engl j med 357;6  www.nejm.org  august 9, 2007 PERSPECTIVE Terra Firma — A Journey from Migrant Farm Labor to Neurosurgery My grandmother was the medicine woman in the small town in rural Mexico where I grew up. As I have gotten older, I have come to recognize the crucial role she played not only in instilling in me the value of healing but also in determining the fate and future of others. She was my first role model, and throughout my life I have depended on the help of my mentors in pursuing my dreams. Like many other illegal immigrants, I arrived in the United States able only to contemplate those dreams — I was not at that point on solid ground. From the fields of the San Joaquin Valley in California to the field of neurosurgery, it has been quite a journey. Today, as a neurosurgeon and researcher, I am taking part in the larger journey of medicine, both caring for patients and conducting clinical and translational research on brain cancer that I hope will lead to innovative ways of fighting devastating disease. And as a citizen of the United States, I am also participating in the great journey of this country. For immigrants like me, this voyage still means the pursuit of a better life — and the opportunity to give back to society. An interview with Dr. QuiГ±ones-Hinojosa can be heard at www.nejm.org. Dr. QuiГ±ones-Hinojosa is an assistant professor of neurosurgery and oncology and director of the brain-tumor stem-cell laboratory at Johns Hopkins School of Medicine, Baltimore, and director of the braintumor program at the Johns Hopkins Bayview campus. Copyright В© 2007 Massachusetts Medical Society. Pay for Performance, Version 2.0? Thomas H. Lee, M.D. “ Old wine in a new bottle.” “A financial gamble.” “An early glimpse of the next generation of pay for performance.” All these appraisals have been applied to Geisinger Health System’s new approach to elective coronary-artery bypass grafting (CABG), which has been described with words rarely invoked in health care, such as “promise” and “guarantee.” Geisinger, an integrated health care delivery system in northeastern Pennsylvania, promises that 40 key processes will be completed for every patient who undergoes elective CABG — even though several of the “benchmarks” are to be reached before or after hospitalization. And although Geisinger cannot guarantee good clinical outcomes, it charges a standard flat rate that covers care for related complications during the 90 days after surgery. As a member of Geisinger’s board of directors, I have watched this program evolve over the past year, and I see truth in all three of the above assessments. Many of the core components of the program are familiar, but this sort of application of those components represents a foray into the unknown. Since a front-page article in the New York Times on May 17, 2007, drew national attention to the Geisinger program, other hospitals have been watching closely and wondering whether they, too, should go down this road. Those who examine it closely will quickly discover that the program is less about cardiac surgery than about the search for an alternative to traditional fee-for-service care. The basic concept is far from radical. The seven cardiac surgeons in the Geisinger delivery system agreed on 40 processes that should be completed during the care of every patient undergoing elective CABG. Most of the “Proven Care Benchmarks” come directly from guidelines established by the American College of Cardiology and the American Heart Association (ACC–AHA) (see box). These steps (such as the administration of preoperative antibiotics at a specified time) are prominent in the critical pathways in use for cardiac surgery at many other hospitals. The list does not force the surgeons to practice “cookbook medicine.” For example, they do not necessarily have to use epiaortic echocardiography to screen for atheromata before manipulating the aorta. But the protocol requires that they consider this test and document the reason if they decide not to use it. Closer inspection reveals some other items on the list that would be new to most critical pathways for CABG. The first benchmark that must be documented is a statement of the indication for CABG according to the ACC–AHA guidelines.1 These guidelines de- n engl j med 357;6  www.nejm.org  august 9, 2007 531 PERSPE C T I V E Pay for Performance, Version 2.0? Selected Key Processes in the Geisinger “Proven Care” Elective CABG Program.* Preadmission documentation American College of Cardiology–American Heart Association indication for surgery Explanation of treatment options to patient Indication of whether patient is a current user of clopidogrel or warfarin Screening for stroke risk Screening for use of epiaortic echocardiography Operative documentation Patient receives correct dose of beta-blocker Patient receives preoperative antibiotics (within 60 minutes of incision; with vancomycin within 120 minutes) Left internal thoracic artery is used for grafting of the left anterior descending artery Postoperative documentation Antibiotics are administered (postoperatively, for 24 to 48 hours) Beta-blocker is administered (within 24 hours after surgery) Tobacco screening and counseling are provided Discharge documentation Referral to cardiac rehabilitation is provided Discharge medications (aspirin, beta-blockers, statin) are prescribed Postdischarge documentation Patient is taking medications correctly Patient has or has not resumed smoking Patient is enrolled in cardiac rehabilitation *CABG denotes coronary-artery bypass grafting. scribe 22 class I indications, for which there is strong evidence in support of the appropriateness of CABG. At the other end of the spectrum are 9 class III indications, for which the evidence actually argues against performing surgery. In between are 11 class IIa indications, for which the evidence generally favors the use of CABG, and 3 class IIb indications, for which there is less support. The surgeons can proceed directly to surgery if the patient has a class I or IIa indication. However, if the strongest indication for surgery is class IIb, the case must be reviewed by a colleague. For patients with class III indications only, surgery is not an option. 532 Another preadmission benchmark is documentation that the surgeon has reviewed the treatment options and their risks and benefits with the patient and that the patient prefers the surgical approach. Completion of this step, along with the appropriateness assessment, provides assurance that the patient both desires and needs the operation. A third innovation is the requirement of postdischarge follow-up to ensure that patients are taking their medications correctly, participating in a rehabilitation program, and (one hopes) refraining from smoking. In between these preadmission and postdischarge steps, the Geising- er program looks very much like other CABG critical pathways. Of course, one key difference is that Geisinger guarantees that all 40 benchmarks will be achieved for every elective CABG. Delivering on that guarantee turned out to be easier said than done. After the Geisinger surgeons agreed on the benchmarks in the spring of 2006, they looked at a series of cases and found that slightly more than half of patients were going through every one of the processes. The surgical teams began creating systems to ensure that all 40 processes would be completed, without disrupting the flow of care. Within a few months, 100% of patients were hitting 100% of the benchmarks. Today, if any of the preoperative benchmarks are overlooked, surgery is delayed until the unfinished task has been completed. Thus far, the Geisinger program sounds like a no-nonsense critical pathway with some extra bells and whistles — but now we get to the risky part. For patients who have surgery as part of this program, Geisinger will not charge for related care within 90 days. For example, there are no additional charges for treatment of sternal wound infections or heart failure due to a perioperative infarction, as long as patients receive their care at a Geisinger facility. On the other hand, the usual charges would apply to care for preexisting heart failure or unrelated problems, such as diverticulitis or a hip fracture. To calculate the case rate for CABG, Geisinger examined its historical costs for related care during the first 90 days after surgery — and then set itself a target of reducing those costs by n engl j med 357;6  www.nejm.org  august 9, 2007 PERSPECTIVE Pay for Performance, Version 2.0? half. Geisinger has some encouraging early data suggesting that its complication rates may have decreased since the program was introduced. But the numbers are small, and no one knows for sure whether this approach will really reduce complication rates or lower postdischarge costs by anything approaching 50%. This uncertainty explains why most chief financial officers get nervous when they hear about Geisinger’s program. They point out that Geisinger is a unique organization. It has its own insurance company, and its physicians are salaried employees of the Geisinger Health System. It has a spectacular management information system that records and guides most aspects of both inpatient and outpatient care. And it has a tradition of innovation and collaboration that makes it easier to get physicians to participate in a program like this one. On the basis of my interactions with Geisinger’s physicians, I would say they are pretty much like the doctors I know everywhere — willing to agree to things that will improve patient care but in no particular hurry to compromise their profession- al autonomy. I also know that Geisinger’s financial leaders (and its board) do not like uncertainty any more than those of other organizations. But the fact is that elective CABG is not a common procedure in the era of statins, betablockers, aspirin therapy, and angioplasty. If the revenue from CABG performed at the case rate is too low to cover costs, Geisinger will be able to adjust its prices upward without causing too much damage. So the gamble, though real, is not huge. And the experience gained by learning how clinicians need to collaborate to succeed within this framework seems worth the risk. The real question for Geisinger and for the rest of the health care system is whether this caserate approach might emerge as a new form of pay for performance. Many current models of pay for performance (involving, for example, quality-of-care measures for patients with diabetes) focus on populations of patients whose care is managed by primary care physicians. For most specialists and hospitals, existing incentive systems put only a modest amount of revenue at stake, and as would be expected, resulting changes in care have been modest as well. But the drumbeat is growing stronger for health care financing models that go beyond rewarding volume alone. Case rates and critical pathways are not foreign concepts at many hospitals — they just have not been married so explicitly before. Geisinger is actively working to extend this approach to other surgical procedures, and diseases treated on an outpatient basis, such as diabetes and hypertension, could be next. A reasonable guess is that models that work for organized delivery systems such as Geisinger will spread over time to the rest of U.S. health care. So this experiment bears watching. Dr. Lee is network president at Partners Healthcare System, Boston, and an associate editor of the Journal. He is a member of the Geisinger board of directors. 1. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Washington, DC: American College of Cardiology, 2004. (Accessed July 19, 2007, at http://www.acc.org/ qualityandscience/clinical/guidelines/cabg/ index.pdf.) Copyright В© 2007 Massachusetts Medical Society. n engl j med 357;6  www.nejm.org  august 9, 2007 533 Clinical Practice Acute Ischemic Stroke A 62-year-old man has sudden weakness of the left arm and leg and slurred speech. Except for untreated hypertension, his medical history is unremarkable. He is original article a current smoker with a smoking history of 45 packProphylaxis versus Episodic Treatment to Prevent years. On arrival at the emergency department 1 hour Joint Disease in Boys with Severe Hemophilia 15 minutes after the onset of symptoms, he reports no This randomized trial involving young boys with severe headache or vomiting. His blood pressure is 180/100 hemophilia showed that prophylaxis with regular infu- mm Hg; his pulse is 76 beats per minute and is regular. sions of recombinant factor VIII was associated with How should this patient be evaluated and treated in clinically and statistically significant reductions in joint the short term? damage, as compared with episodic infusions at the See P. 572; CME, P. 629 time of a clinically evident hemarthrosis. Because of the high cost of recombinant factor VIII, its widespread Current Concepts use for prophylaxis may be impractical. Drug-Induced Immune Thrombocytopenia See P. 535; Editorial, P. 603; CME, P. 630 Drug-induced thrombocytopenia should be suspected in any patient with acute thrombocytopenia of unknown Original Article cause. Although the incidence is low, more than 100 Rituximab for the Treatment of Severe Pemphigus drugs have been implicated in thrombocytopenia, inIn this study of 21 patients with severe pemphigus cluding quinine, sulfonamides, abciximab, carbamazewhose disease was refractory to or dependent on sys- pine, and vancomycin, as well as herbal remedies and temic corticosteroids or who had contraindications to several nonprescription drugs. This review summarizes corticosteroids, 18 patients (86%) had a complete re- the current understanding of pathogenesis and provides mission after a single cycle of rituximab treatment. Two a guide for diagnosis and management of this potenpatients had serious infections, one of which resulted in tially dangerous disorder. death. The efficacy of rituximab for pemphigus must be See p. 580; CME, P. 631 weighed against the risk of severe adverse events. CASE RECORDS OF THE MASSACHUSETTS GENERAL HOSPITAL See P. 545; Editorial, P. 605 A Pregnant Woman with Altered Mental Status Original Article A 20-year-old pregnant woman was admitted at 26 weeks’ gestation because of dizziness, confusion, and difficulty walking. Six weeks earlier, she was confused and had A variant on complement factor 3 is associated with odd head movements. Four days before admission, age-related macular degeneration, with a population she had dizziness and weakness; she began to fall to attributable risk of 22%. This finding underlines the her left and vomited. On admission, examination of the importance of complement activation in the pathogen- cerebrospinal fluid showed a lymphocytic pleocytosis esis of the disease. with mildly elevated protein and normal glucose levels. See P. 553 During the next 18 days, her condition worsened. Complement C3 and Age-Related Macular Degeneration Original Article See P. 589 NXY-059 for Acute Ischemic Stroke Sounding Board Two phase 3 clinical trials (SAINT I and SAINT II) evaluated the free-radical–trapping agent NXY-059 for the treatment of acute ischemic stroke. The SAINT I trial, reported last year, suggested that NXY-059 might be effective. The authors now report the results of the SAINT II trial, which clearly shows that NXY-059 is not effective for ischemic stroke. The discrepancy in the findings of the two trials is best explained by chance false positive findings in the SAINT I trial. See P. 562 534 Needing to Improve Care versus Knowing How to Do It The authors argue that interventions to improve health care quality should be held to the same standards that we apply to medical treatments. They believe qualityimprovement initiatives should not be widely disseminated unless studies have demonstrated that they are safe and effective. See P. 608 n engl j med 357;6  www.nejm.org  august 9, 2007 new england journal of medicine The established in 1812 august 9, 2007 vol. 357  no. 6 Prophylaxis versus Episodic Treatment to Prevent Joint Disease in Boys with Severe Hemophilia Marilyn J. Manco-Johnson, M.D., Thomas C. Abshire, M.D., Amy D. Shapiro, M.D., Brenda Riske, M.S., M.B.A., M.P.A., Michele R. Hacker, Sc.D., Ray Kilcoyne, M.D., J. David Ingram, M.D., Michael L. Manco-Johnson, M.D., Sharon Funk, B.Sc., P.T., Linda Jacobson, B.S., Leonard A. Valentino, M.D., W. Keith Hoots, M.D., George R. Buchanan, M.D., Donna DiMichele, M.D., Michael Recht, M.D., Ph.D., Deborah Brown, M.D., Cindy Leissinger, M.D., Shirley Bleak, M.S.N., Alan Cohen, M.D., Prasad Mathew, M.D., Alison Matsunaga, M.D., Desiree Medeiros, M.D., Diane Nugent, M.D., Gregory A. Thomas, M.D., Alexis A. Thompson, M.D., Kevin McRedmond, M.D., J. Michael Soucie, Ph.D., Harlan Austin, Ph.D., and Bruce L. Evatt, M.D. A bs t r ac t background Effective ways to prevent arthropathy in severe hemophilia are unknown. Methods We randomly assigned young boys with severe hemophilia A to regular infusions of recombinant factor VIII (prophylaxis) or to an enhanced episodic infusion schedule of at least three doses totaling a minimum of 80 IU of factor VIII per kilogram of body weight at the time of a joint hemorrhage. The primary outcome was the incidence of bone or cartilage damage as detected in index joints (ankles, knees, and elbows) by radiography or magnetic resonance imaging (MRI). Authors’ affiliations are listed in the Appendix. Address reprint requests to Dr. M.J. Manco-Johnson, Mountain States Regional Hemophilia and Thrombosis Center, MS F-416, PO Box 6507, Aurora, CO 80045, or at marilyn.manco-johnson@ uchsc.edu. N Engl J Med 2007;357:535-44. Copyright В© 2007 Massachusetts Medical Society. Results Sixty-five boys younger than 30 months of age were randomly assigned to prophylaxis (32 boys) or enhanced episodic therapy (33 boys). When the boys reached 6 years of age, 93% of those in the prophylaxis group and 55% of those in the episodic-therapy group were considered to have normal index-joint structure on MRI (P = 0.006). The relative risk of MRI-detected joint damage with episodic therapy as compared with prophylaxis was 6.1 (95% confidence interval, 1.5 to 24.4). The mean annual numbers of joint and total hemorrhages were higher at study exit in the episodic-therapy group than in the prophylaxis group (P<0.001 for both comparisons). High titers of inhibitors of factor VIII developed in two boys who received prophylaxis; three boys in the episodic-therapy group had a life-threatening hemorrhage. Hospitalizations and infections associated with central-catheter placement did not differ significantВ ly between the two groups. Conclusions Prophylaxis with recombinant factor VIII can prevent joint damage and decrease the frequency of joint and other hemorrhages in young boys with severe hemophilia A. (ClinicalTrials.gov number, NCT00207597.) n engl j med 357;6  www.nejm.org  august 9, 2007 535 The n e w e ng l a n d j o u r na l B efore the development of cryoprecipitate, a plasma fraction that contains concentrated factor VIII, boys with severe hemophilia A had a diminished life expectancy.1-3 These children are at risk for many types of hemorrhages, but the predominant source of chronic coexisting disease is crippling, painful arthritis due to hemarthrosis.4 Small trials were conducted in the 1960s to determine whether routine administration of factor VIII concentrate was effective as prophylaxis against hemophilic arthropathy.5‑8 Clinically effective prophylactic schedules were developed empirically, without the benefit of data from controlled trials,9 and many clinicians began to recommend prophylaxis with factor VIII.10 In the 1980s, when it was discovered that plasma-derived factor VIII concentrates were contaminated by human immunodeficiency and hepatitis viruses, the use of prophylaxis was severely curtailed.4 In 1992, approval of the first recombinant factor VIII molecule for replacement therapy in the United States allowed for safe prophylaxis in patients with hemophilia.11 Petrini and colleagues reported the prevention of hemophilic arthropathy when prophylaxis was initiated before patients reached 2 years of age.12 Aledort and others reportВ ed that prophylaxis slowed the progression of established joint damage.13 Nevertheless, questions remained as to when prophylaxis should begin, what dose of recombinant factor VIII should be administered, and how long prophylaxis should be provided. An important question that could be answered by a clinical trial was whether prophylaxis prevents joint hemorrhage and damage.14 The aim of our randomized trial was to determine whether prophylactic factor VIII infusions, given every other day, are more effective in preventing joint damage than an intensive replacement regimen given at the time of a hemarthrosis. The study focused on the index joints — ankles, knees, and elbows — because these joints are the most susceptible to hemophilic arthropathy. This trial was conducted in the context of a national hemophilia comprehensive care system.15 Me thods Study Design We conducted a multicenter, randomized, openlabel trial, with written informed consent obtained from the parents or guardians of all patients. Enrollment began in August 1996, and the last sub536 of m e dic i n e ject to be enrolled completed the study in April 2005. The power calculation was based on pilot data indicating that normal joint structure would be maintained in 70% of children receiving prophylaxis and 20% of those receiving enhanced episodic therapy. Estimated proportions of loss of participants were 10% for the assessment of early joint damage, 7% for the development of high-titer factor VIII antibodies, 7% for the assessment of lifethreatening hemorrhage, and 10% for follow-up. Thus, 64 participants were needed to detect a significant difference between the two treatments with a two-sided test (0.05 alpha level and 95% power). Randomization was performed centrally and stratified by site in permuted blocks of 2, 4, or 6. The radiologists who reviewed joint images, the physiotherapists who performed joint examinations, and the laboratory technologists who performed assays were unaware of the patients’ treatment assignments and status with respect to a history of bleeding. Eligibility and Exclusion Criteria Eligibility criteria were an age of less than 30 months, a factor VIII activity level of 2 U per deciliter or less, a history of two or fewer hemorrhages into each index joint, normal baseline joint imaging, undetectable levels of factor VIII inhibitor, a normal platelet count, and normal joint motion. Treatment Children in the prophylaxis group received infusions of 25 IU of factor VIII (Kogenate or Kogenate FS, Bayer HealthCare) per kilogram of body weight every other day to prevent bleeding. The dose and the frequency of administration were based on pharmacokinetic studies and clinical experience.9,16 Hemarthroses were defined as acute episodes of joint pain with decreased joint motion. When hemarthroses occurred during prophylaxis, patients were treated with 40 IU per kilogram, and the assigned prophylaxis schedule was resumed the next day. Children assigned to receive enhanced episodic therapy were treated only at the time of clinically recognized joint hemorrhage. The rationale for this treatment was to decrease inflammation and prevent joint damage by preventing rebleeding after a joint hemorrhage. Children in this group received 40 IU of factor VIII per kilogram at the time of joint hemorrhage and 20 IU at 24 hours and 72 hours after the first dose. Parents were n engl j med 357;6  www.nejm.org  august 9, 2007 Preventing Joint Disease in Hemophilia encouraged to continue infusions of 20 IU of factor VIII per kilogram every other day until joint pain and impairment of mobility had completely resolved, for a maximum of 4 weeks. All other therapies, including surgery, and all bleeding events other than hemarthroses, including nasal, muscle, parenchymal, gastrointestinal, and intracranial hemorrhages, were managed according to local standards of practice. In both groups, the protocol allowed for two dose escalations of 5 IU of factor VIII per kilogram in the case of an inadequate response. The protocol did not require the use of central-venous-access devices, and all decisions regarding placement of the devices were made according to local standards. Outcome Measures laxis group only), and serologic tests for hepatitis B and C, human immunodeficiency virus, and parvovirus. Titers of factor VIII inhibitors were determined with the use of the Bethesda assay.19 Factor VIII trough levels were not used to alter dosing. Clinical Assessment of Joints Clinical examination of joints, with assessment of swelling, strength, range of motion, pain, and gait, was performed semiannually, as previously described, and videotaped for central review at study entry, midpoint, and completion.20,21 Protocol Failure before Study Completion The protocol allowed for early termination of participation if the assigned treatment was deemed inadequate for the child as evidenced by the development of factor VIII inhibitors, life-threatening hemorrhage, or bone or cartilage damage on joint imaging. If an inhibitory titer exceeded 25 BU in duplicate testing of the sample or if it exceeded 10 BU for more than 3 months, the child was withdrawn from the study. These thresholds were chosen to avoid the withdrawal of a child with a transient factor VIII inhibitor (Lusher JM: personal communication).22 Life-threatening hemorrhages were treated in accordance with local standards. After the resolution of the first such event, the assigned treatment was resumed. In the event of recurrence, the child was removed from the study, but data were retained for inclusion in intention-to-treat analyses. Participants with clinically suspected early joint failure were eligible for an early joint evaluation. The joint (or joints) in question were evaluated by means of MRI, radiography, or both if the child had had 8 hemorrhages into an index joint within 12 consecutive months or 20 hemorrhages into an index joint since study enrollment or if the highest score obtainable on any one item of the joint physical examination had been recorded at least 2 weeks after hemarthrosis. If the imaging evaluation showed bone or cartilage damage, the child was removed from the study. The primary outcome was preservation of indexjoint structure, as determined by means of magnetic resonance imaging (MRI) and plain-film radiography at the completion of the study, when participants were 6 years old. Secondary outcomes were number of joint and other bleeding events, number of infusions, and total units of factor VIII administered. MRI and plain-film radiography were performed as described previously.17,18 Joint failure was defined as an MRI or radiograph score that indicated a subchondral cyst, surface erosion, or joint-space narrowing. MRIs and radiographs were read independently by two radiologists; discrepant readings were adjudicated by a third radiologist. Reports of infusions of factor VIII and emergency-room and clinic visits were collected monthly. At quarterly visits, data were collected on hospitalizations, port placements, port removals, and infections. Each child was examined quarterly and weighed for calculation of the dose of factor VIII. Race and ethnic group were reported by the parent or guardian of each child. Compliance was monitored by a review of infusion logs. However, no child was removed from the study for any level of noncompliance. Death, recurrent life-threatening hemorrhage, an inhibitory titer of 10 or more Bethesda units (BU), and hospitalization were classified as serious adverse Statistical Analysis events. We used Fisher’s exact test to compare the two Laboratory Assays groups with respect to the primary outcome — Blood was collected quarterly for the detection and the proportion of children in whom normal joint measurement of factor VIII inhibitors, measure- structure was maintained, as determined by MRI ment of factor VIII trough levels (in the prophy- or radiography. The relative risk of joint damage n engl j med 357;6  www.nejm.org  august 9, 2007 537 The n e w e ng l a n d j o u r na l of m e dic i n e 119 Patients were screened 54 Were not eligible or did not give consent 65 Underwent randomization 33 Were assigned to enhanced episodic therapy 32 Were assigned to prophylaxis 3 Were removed from protocol because of lifethreatening hemorrhage 6 Were removed from protocol because of joint damage 1 Was withdrawn 1 Was lost to follow-up 2 Were removed from protocol because of hightiter inhibitor 1 Was removed from protocol because of joint damage 2 Were withdrawn 27 Completed protocol 22 Completed protocol Figure 1. Randomization and Follow-up of Study Participants. Although just 27 boys in the prophylaxis group and 22 boys in the episodic-therapy group remained on the protocol unВtil the age of 6 years, primary outcome data wereManco-Johnson available for boys who were removed from the protocol before RETAKE 1st AUTHOR: ICM 2nd the age of 6 years. REG F FIGURE: 1 of 3 3rd CASE EMail Line 4-C Revised SIZE ARTIST: ts H/T H/Tinterim 33p9 and 95% confidence intervals were included joint imaging studies in children Enon calculated for Combo the episodic-therapy group as compared with the who were withdrawn from the study because of AUTHOR, PLEASE NOTE: prophylaxis group. Differences inFigure secondary joint damage has been outredrawn early and type has been reset. and joint imaging studies perPlease check carefully. comes were evaluated with the t-test or the Mann– formed in the remaining children at the age of Whitney U test, as appropriate. The Spearman cor- 6 years. For the secondary analyses, data were inJOB: 35706 ISSUE: 08-09-07 relation coefficient was calculated for data that cluded until withdrawal from the study, loss to were not normally distributed. Two-sided P values follow-up, early protocol failure, or completion of of less than 0.05 were considered to indicate sta- the study at the age of 6 years. tistical significance. The proportion of data collected was calculated Two interim analyses were planned and con- by dividing the number of data forms received by ducted by an independent data and safety moni- the number of forms expected. Compliance was toring board after one third and two thirds of determined by calculating the proportion of preparticipants had undergone evaluation of the out- scribed infusions that were actually administered. come measures. Data used for interim analyses included MRI and radiographic findings, the numR e sult s ber of joint hemorrhages, the occurrence of lifethreatening hemorrhages, and the total number Sixty-five children were enrolled in the study beof hemorrhages and hospitalizations. All partici- tween August 1996 and March 2000; 32 children pants randomly assigned to a treatment group were randomly assigned to prophylaxis and 33 to were included in the intention-to-treat analysis of enhanced episodic treatment (Fig 1). The two the primary outcome. Data used for this analysis groups showed no differences in baseline demo- 538 n engl j med 357;6  www.nejm.org  august 9, 2007 Preventing Joint Disease in Hemophilia graphic characteristics (Table 1). The median factor VIII activity level for all the children was 0.6 U per deciliter, with a range of 0.3 to 2.0; 31 of the 65 participants (48%) had one or more hemarthroses into index joints before enrollment. The mean period of participation in the study was 49 months (interquartile range, 48 to 58). Primary outcome data from both MRI and radiographic studies were obtained for 50 of 65 participants (77%); partial data (with either MRI or radiography) were obtained for 11 participants (17%); and there were no data available for 4 participants (6%). Mean compliance was 96% (interquartile range, 96 to 100) in the prophylaxis group and 98% (interquartile range, 98 to 100) in the episodic therapy group. Among all participants, an average of 94% of data forms were received. Outcome results are shown in Table 2. According to the findings on MRI, the proportion of participants in whom all six index joints were normal at 6 years of age was 25 of 27 (93%) in the prophylaxis group and 16 of 29 (55%) in the enhanced episodic-therapy group (P = 0.002). As compared with the prophylaxis group, the episodictherapy group had a relative risk of damage to one or more joints, as shown by MRI, of 6.1 (95% confidence [CI], 1.5 to 24.4). The corresponding relative risk for the prophylaxis group, as compared with the episodic-therapy group, was 0.17, indicating an 83% reduction in the risk of joint damage as determined by MRI. With the use of radiography to assess joint damage, the relative risk was 5.2 (95% CI, 0.65 to 41.5) with episodic therВ apy as compared with prophylaxis. Radiographic and MRI readings were concordant in 97% of index joints. A total of 18 abnormal joints (13 ankles, 3 elbows, and 2 knees) were detected in 15 children — 2 in the prophylaxis group and 13 in the episodic-therapy group. Six of the abnormalities were detected by both MRI and radiography, seven by MRI alone, and one by radiography alone. Only one type of imaging was available for the four remaining abnormal joints. For each joint, the MRI score was compared with the total number of hemarthroses. As shown in Figure 2, some joints had abnormal MRI scores but no hemarthrosis, and some had normal MRI scores despite many hemarthroses. Bone and cartilage damage detected on MRI was not correlated with hemarthroses (P = 0.63), and overall the correlation of hemarthroses with MRI scores was Table 1. Baseline Demographic and Clinical Characteristics of All Randomized Participants. Enhanced Episodic Therapy (N = 33) P Value Characteristic Prophylaxis (N = 32) Mean age (yr) 1.6 1.6 24 (75) 25 (76) Race or ethnic group — no. (%)* White 0.78 0.33 Black 0 3 (9) Hispanic 4 (13) 4 (12) Asian or Pacific Islander 1 (3) 1 (3) American Indian or Alaskan native 1 (3) 0 Other 2 (6) 0 Educational level of parent or guardian — no. (%) 0.06 ≤12 yr 20 (63) 13 (39) >12 yr 12 (37) 20 (61) First index-joint hemorrhage before enrollment — no. (%) 0.17 Yes 18 (56) 13 (39) No 14 (44) 20 (61) No. of previous index-joint hemorrhages 0.17 Mean 1.0 0.6 Range 0–5 0–3 Mean 6.2 6.8 Range   0–35   0–32 No. of previous total hemorrhages 0.74 *Race and ethnic group were reported by the parent or guardian of each child. weak (r = 0.14, P = 0.02). Joint physical-examination scores showed a weak correlation with MRI scores (r = 0.26, P<0.001). Table 2 shows secondary outcomes. Table 3 shows serious adverse events. Average monthly factor VIII use and hemorrhages, as well as joint physical examination scores, stratified by year of age, are shown in Figure 3. No statistically significant differences between the two treatment groups were found with respect to joint scores on physical examination (Fig. 3A). A central-venous-access device was placed in 54 children (83%). In 12 of these boys (22%), at least one infection associated with the device developed. The median number of hospitalizations per year was similar for both study groups. Most hemophilia-related hospitalizations were for place- n engl j med 357;6  www.nejm.org  august 9, 2007 539 The n e w e ng l a n d j o u r na l of m e dic i n e Table 2. Outcome Data.* Variable Prophylaxis (N = 32) Enhanced Episodic Therapy (N = 33) P Value 27 29 0.73 2 (7) 13 (45) 0.002 25 (93) 16 (55) MRI findings No. of participants with primary outcome data Joint damage — no. (%) No joint damage — no. (%) Radiographic findings No. of participants with primary outcome data 28 27 0.73 1 (4)   5 (19) 0.10 27 (96) 22 (81) Mean   1,497   1,490 Total 47,895 49,179 Mean 653В±246 187В±100 Total 20,896 6,176 Mean 352,793В±150,454 113,237В±65,494 Total 11,289,372 3,736,807 0.63В±1.35 4.89В±3.57 0.20 4.35 3.27В±6.24 17.69В±9.25 1.15 17.13 Joint damage — no. (%) No joint damage — no. (%) No. of days in study 0.95 Reported no. of factor VIII infusions <0.001 Reported no. of factor VIII units infused <0.001 Joint hemorrhages (no./participant/yr) Mean Median <0.001 Total hemorrhages (no./participant/yr) Mean Median <0.001 *Plus–minus values are means В±SD. The data on MRI and radiographic findings include interim-analysis data for children who were removed from the study because of early joint failure. ment and removal of central-venous-access de- and was based on a history of joint hemorrhage vices. rather than age. In the prophylaxis group, radiologic evidence of preserved joint architecture was found in 93% of participants at 6 years of age. Dis cus sion In this group, 18 of 32 (56%) of the children had We found that prophylaxis with recombinant fac- one or two hemarthroses into one or more index tor VIII was effective in preventing hemarthroses joints before prophylaxis, and 17 (53%) had one and structural joint damage (as detected by MRI) to five hemorrhages into one or more index joints in young boys with hemoВphilia A.23 Reported sug- during prophylaxis. Prophylaxis was efficacious gestions for the best time to begin prophylaxis in decreasing bleeding and joint damage after range from before the first joint hemorrhage9 to up to five hemarthroses. before 1 to 2 years of age to before the occurrence More than half of the joint abnormalities that of five hemarthroses.24 In our trial, prophylaxis were detected by MRI were not apparent in radiowas initiated between the ages of 6 and 30 months graphic studies, whereas only one joint abnormal- 540 n engl j med 357;6  www.nejm.org  august 9, 2007 Preventing Joint Disease in Hemophilia 10 9 8 7 6 MRI Score ity that was detected by radiography was not detectВ ed by MRI, indicating that MRI is more sensitive than radiography. We believe that MRI is the preВ ferable imaging technique for young boys with hemophilia. Surprisingly, the number of clinically evident hemarthroses correlated weakly with the outcome as determined by MRI. In addition, joint abnormalities were not apparent on physical examination in the very young children in our study. It is possible that the joint score we used was insufficiently sensitive for the detection of early arthropathy, even though our physical-examination scoring system is more sensitive for the detection of mild abnormalities of gait, joint swelling, muscle strength, and atrophy than is that of the World Federation of Hemophilia.9,12,13,20 Thus, the absence of overt hemarthroses and abnormalities of joints on physical examination can lead to the erroneous assumption that episodic therapy in young children with hemophilia is effective. We propose that chronic microhemorrhage into the joints or subchondral bone in young boys with hemophilia causes deterioration of joints without clinical evidence of hemarthroses and that prophylaxis prevents this subclinical process. The enhanced episodic therapy used in this trial was experimental because it involved higher doses and more infusions of factor VIII than are provided in standard care. Enhanced episodic therapy was used because the outcome of standard care is poor.13 Clearly, however, the results of enhanced episodic therapy were inferior to those of alternate-day prophylaxis. Children who received enhanced episodic therapy had extra-articular bleeding in addition to hemarthroses; 10% had recurrent, life-threatening hemorrhage, including intracranial and gastrointestinal hemorrhage. Two children in the prophylaxis group were found to have high titers of factor VIII inhibitors. This finding was not unexpected, since inhibitors develop in 30% of children with severe hemophilia, usually within the first 50 exposures to factor VIII, and most of the children in our study had fewer than 50 factor VIII exposures at the time of enrollment. Use of recombinant factor VIII has been estimated to account for more than 90% of the cost of hemophilia care.25,26 By the age of 6 years, the children in the prophylaxis group in our study 5 4 3 2 1 0 0 5 10 15 20 25 No. of Clinically Evident Index-Joint Hemorrhages Figure 2. MRI Score for Index Joint According to AUTHOR: Manco-Johnson the ICM Number of Hemorrhages in That JointRETAKE for Both 1st 2nd Treatment Groups.2 of 3 REG F FIGURE: 3rd TheCASE MRI score is the average of the two concordant Revised Line a normal 4-C joint and readings; EMail a score of 0 indicates SIZEa ARTIST: ts H/T to H/T score of 7 to 10 indicates damage joint bone16p6 or carEnon Combo tilage. The size of each circle corresponds to the numPLEASE of NOTE: ber of cases. TheAUTHOR, largest number index joints had Figure has been redrawn and type has been reset. no hemorrhage andPlease an MRI score of 0. The shaded area check carefully. of the graph shows the 14 joints with bone or cartilage damage on MRI. The larger bubbles represent JOB: 35706 ISSUE: more 08-09-07 than one joint. Some joints with no hemorrhages had high MRI scores, whereas some joints with more than 10 hemorrhages did not show bone or cartilage damage on MRI. Table 3. Serious Adverse Events.* Event Prophylaxis (N = 32) Enhanced Episodic Therapy (N = 33) P Value Detection of high-titer inhibitor (no. of participants) 2 0 0.24 Life-threatening hemorrhage (no. of participants) 0 3 0.24 Hemophilia-related hospitalization (no./participant/yr) Mean Median 1.70В±8.03 0.47В±0.85 0.25 0.24 0.90 CVAD (no. of participants) 29 25 0.19 ≥1 CVAD-related infection (no. of participants) 6 6 0.95 *Plus–minus values are means В±SD. CVAD denotes central-venous-access device. n engl j med 357;6  www.nejm.org  august 9, 2007 541 n e w e ng l a n d j o u r na l The m e dic i n e of A =1 1 Episodic therapy N 18 16 14 =2 2 7 =2 =2 =2 N N N 3 =3 N 4 N =2 7 N =2 9 9 =2 N =2 5 =2 5 N 6 6 8 N N =2 10 2 5 12 N Average Joint Physical-Examination Score Prophylaxis 2 0 1 2 3 4 5 6 Age (yr) B Average No. of Hemorrhages per Mo Prophylaxis: Joint hemorrhages Prophylaxis: Other hemorrhages Episodic therapy: Joint hemorrhages Episodic therapy: Other hemorrhages 1.8 N=25 1.6 1.4 1.2 N=31 N=31 N=33 N=24 1.0 0.8 0.6 N=23 0.4 N=31 0.0 1 2 N=26 N=29 N=29 0.2 3 4 5 Age (yr) C 6 N N =2 =2 9 9 =2 N N N 500 =2 3 =3 1 600 Episodic therapy 6 400 N N N =3 =3 N =2 4 200 1 3 =3 1 =2 300 N Average Monthly Factor VIII Use (IU/kg) Prophylaxis 100 0 1 2 3 4 5 Age (yr) were receiving 6000 IU of factor VIII per kilogram Prophylaxis has not been widely used in the per year, as compared with approximately 2500 IU care of patients with hemophilia. In 1995, when per kilogram in the enhanced ICM episodic group. At the currentRETAKE study was 1st conceived, only 33% of U.S. AUTHOR: Manco-Johnson 2nd FIGURE: 3 of 3 a price of $1 per unit of recombinant factor VIII, children with hemophilia received prophylaxis.27 REG F 3rd the cost of prophylaxis for a child The Centers Revised for Disease Control and Prevention CASE weighing 50 kg Line 4-C could reach $300,000 per year.EMail ARTIST: ts reported that SIZE 51.5% of children with severe H/T H/T 33p6 Combo n engl j med 357;6  www.nejm.org  august 9, 2007 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. Enon 542 JOB: 35706 ISSUE: 08-09-07 Preventing Joint Disease in Hemophilia Figure 3 (facing page). Joint Scores on Physical Examination, Frequency of Bleeding Events, and Factor VIII Use According to Age and Study Group. Panel A shows the mean joint score on physical examination. The scale sums the scores of all six index joints. Mean joint scores for the two study groups were not significantly different at any age. In Panel B, mean joint and other hemorrhages increased progressively throughout the study in children receiving enhanced episodic therapy, whereas the mean numbers of joint and other hemorrhages remained at a low level in children receiving prophylaxis. As shown in Panel C, factor VIII use per kilogram rose progressively throughout the study period in the episode-therapy group; overall, however, there was greater use in the prophylaxis group than in the episodictherapy group (P<0.001 for each year of age). T bars indicate standard errors. N denotes the number of participants at risk in each age group. hemophilia who were younger than 6 years of age received prophylaxis during 2004.28 We previously reported that the time required for infusions, unwillingness on the part of the child, limitations in venous access, and difficulty in balancing prophylaxis with other family needs were major barriers to the implementation of prophylaxis.29 Even in the present group of highly motivated, intensively supported families, the infusion schedule was inadequate for 2 of the 32 participants in the prophylaxis group. This study demonstrates the efficacy of prophylaxis with recombinant factor VIII in reducing the incidence of joint hemorrhages, life-threatening hemorrhages, and other hemorrhages and in lowering the risk of joint damage among young boys with severe factor VIII deficiency. However, the high cost of recombinant factor VIII is a barrier to widespread acceptance of prophylaxis. Supported by grants from the Centers for Disease Control and Prevention (U27/CCU812106) and the National Institutes of Health (R00069). Bayer HealthCare donated the factor VIII used in the study but had no role in study design, data accrual, data analysis, or manuscript preparation. The Hemophilia and Thrombosis Research Society recruited sites for participation. Dr. Manco-Johnson reports receiving consulting fees from Baxter BioScience, Bayer HealthCare, CSL Behring, and Wyeth, speaking fees from Baxter BioScience, Bayer HealthCare, CSL Behring, and Novo Nordisk, licensure study support from Baxter BioScience, Bayer HealthCare, CSL Behring, Wyeth, and Novo Nordisk, and grant support from Bayer HealthCare; Dr. Abshire, consulting fees from Bayer HealthCare, CSL Behring, and Novo Nordisk and licensure study support from Baxter BioScience, Bayer HealthCare, CSL Behring, Octagen, and Wyeth; Dr. Shapiro, consulting fees from Baxter BioScience, Bayer HealthCare, Inspiration Biopharmaceuticals, Pro Metic, Syntonix Pharmaceuticals, and Wyeth, speaking fees from Baxter BioScience, Novo Nordisk, and Wyeth, licensure study support from Baxter BioScience, Bayer HealthCare, CSL Behring, Novo Nordisk, Octagen, and Wyeth, and grant support from Novo Nordisk; Ms. Riske, consulting and lecture fees from Bayer HealthCare; Dr. Valentino, consulting fees from Baxter BioScience, CSL Behring, and Wyeth, speaking fees from Baxter HealthCare, Novo Nordisk, and Wyeth, licensure study support from Baxter HealthCare, Novo Nordisk, and Wyeth, and grant support from Baxter BioScience; Dr. Hoots, consulting fees from Baxter BioScience, Bayer HealthCare, CSL Behring, Novo Nordisk, and Wyeth, speaking fees from Baxter Bioscience, Bayer HealthCare, Novo Nordisk, and Wyeth, licensure study support from Avigen, Baxter BioВ Science, Bayer HealthCare, CSL Behring, Grifols, Novo Nordisk, Octagen, Rho, and Wyeth, and grant support from Wyeth; Dr. DiMichele, consulting fees from Bayer HealthCare, speaking fees from Baxter BioScience, Bayer HealthCare, and Novo Nordisk, licensure study support from Baxter BioScience, CSL Behring, and Wyeth, and grant support from Baxter BioScience, Bayer HealthCare, CSL Behring, Grifols Biologics, and Wyeth; Dr. Recht, consulting fees from Baxter BioScience and licensure study support from Baxter BioScience and Wyeth; Dr. Leissinger, consulting fees from Baxter BioScience and CSL Behring, speaking fees from Sanofi-Aventis and Grifols, and licensure study support from Baxter BioScience, Bayer HealthCare, and Wyeth; Dr. Mathew, consulting fees from Bayer HealthCare and CSL Behring, speaking fees from Baxter BioScience, Bayer HealthCare, CSL Behring, Novo Nordisk, and Wyeth, and licensure study support from Baxter BioScience, Bayer HealthCare, Novo Nordisk, and Wyeth; Dr. Nugent, consulting fees from Bayer HealthCare and Novo Nordisk and licensure study support from Bayer HealthCare and CSL Behring; Dr. Thompson, consulting and speaking fees from Novartis and grant support from Baxter BioScience and Novartis; and Dr. Brown, licensure study support from Grifols, Baxter HealthCare, Novo Nordisk, Octagen, and Wyeth and grant support from CSL Behring. No other potential conflict of interest relevant to this article was reported. We thank the Data and Safety Monitoring Board members — Dr. Louis Aledort (chair), Dr. David Tubergen, Dr. Gary Cutter, Dr. Mark Yarborough, Mary Jo Cleveland, and Susan Havens — for their valuable contributions throughout the study; the study nurses, especially Sheryl Giambartolomei, for their diligence in data collection; Dr. Neil Goldenberg for his thoughtful comments and support in the conduct and analysis of the study; Dr. Eduard Gorina, Dr. Peter Larsen, Dr. Richard Lutes, and Chris Cheney of Bayer HealthCare; and the parents and participants who made this study possible. This article is dedicated to Dr. Ray Kilcoyne, pioneer in magnetic resonance joint imaging in hemophilia, who died shortly after completion of the Joint Outcome Study. appendix The authors are affiliated with the following institutions: the University of Colorado and Health Sciences Center (M.J.M.-J., B.R., R.K., M.L.M.-J., S.F., L.J.,) and Children’s Hospital (M.J.M.-J., J.D.I.), Denver; Emory University, Atlanta (T.C.A.); Indiana Hemophilia and Thrombosis Center, Indianapolis (A.D.S.); Beth Israel Deaconess Medical Center, Harvard Medical School, Boston (M.R.H.); Rush Children’s Hospital, Chicago (L.A.V.); University of Texas, Houston (W.K.H., D.B.); University of Texas Southwestern Medical Center and Children’s Medical Center at Dallas (G.R.B.); Weill Medical College of Cornell University, New York (D.D.); Phoenix Children’s Hospital, Phoenix, AZ (M.R.); Tulane University, New Orleans (C.L.); Primary Children’s Hospital, Salt Lake City (S.B.); University of Pennsylvania School of Medicine, Children’s Hospital of Philadelphia (A.C.); University of New Mexico, Albuquerque (P.M.); Oakland Children’s Hospital, Oakland, CA (A.M.); University of Hawaii, Honolulu (D.M.); Children’s Hospital of Orange County, CA (D.N.); Oregon Health and Science University, Portland (G.A.T.); Children’s Memorial Hospital and Northwestern University, Chicago (A.A.T.); Palmetto Health Richland, Columbia, SC (K.M.); and Centers for Disease Control and Prevention, Atlanta (J.M.S., H.A., B.L.E.). n engl j med 357;6  www.nejm.org  august 9, 2007 543 Preventing Joint Disease in Hemophilia References 1. Mejia-Carvajal C, Czapek EE, Valenti- no LA. Life expectancy in hemophilia outcome. J Thromb Haemost 2006;4:507-9. 2. Chorba TL, Holman RC, Strine TW, Clarke MJ, Evatt BL. Changes in longevity and causes of death among persons with hemophilia A. Am J Hematol 1994;45: 112-21. 3. Ikkala E, Heilske T, MyllylГ¤ G, Nevanlinna HR, PitkГ¤nen P, Rasi V. Changes in the life expectancy of patients with severe haemophilia A in Finland in 1930-79. Br J Haematol 1982;52:7-12. 4. Manco-Johnson MJ, Riske B, Kasper CK. Advances in care of children with hemoВphilia. Semin Thromb Hemost 2003; 29:585-94. 5. Ahlberg A. Haemophilia in Sweden. VII. Incidence, treatment and prophylaxis of arthropathy and other musculo-skeletal manifestations of haemophlia A and B. Acta Orthop Scand Suppl 1965;77:3-132. 6. Robinson PM, Tittley P, Smiley RK. Prophylactic therapy in classical hemophilia: a preliminary report. Can Med Assoc J 1967;97:559-61. 7. Shanbrom E, Thelin GM. Experimental prophylaxis of severe hemophilia with a factor VIII concentrate. JAMA 1969;208: 1853-6. 8. Van Creveld S. Prophylaxis of joint hemorrhages in hemophilia. Acta Haematol 1969;41:206-14. 9. Nilsson IM, Berntorp E, LГ¶fqvist T, Pettersson H. Twenty-five years’ experience of prophylactic treatment in severe haemophiВ lia A and B. J Intern Med 1992;232:25-32. 10. Medical and Scientific Advisory Council (MASAC) recommendations concerning prophylaxis. Medical bulletin #193. New York: National Hemophilia Foundation, March 11, 1994. 11. Recombinate: licensed on December 10, 1992. FDA bulletin P92-39. Rockville, MD: Food and Drug Administration, 1992. (Accessed July 13, 2007, at http://www.fda. gov/bbs/topics/NEWS/NEW00312.html.) 12. Petrini P, Lindvall N, Egberg N, Blomback M. Prophylaxis with factor concentrates in preventing hemophilic arthropathy. Am J Pediatr Hematol Oncol 1991; 13:280-7. 13. Aledort LM, Haschmeyer RH, Pettersson H. A longitudinal study of orthopaedic outcomes for severe factor-VIII-deficient haemophiliacs. J Intern Med 1994;236: 391-9. 14. Stobart K, Iorio A, Wu JK. Clotting factor concentrates given to prevent bleeding and bleeding-related complications in people with hemophilia A or B. Cochrane Database Syst Rev 2006;2:CD003429. 15. Baker JR, Crudder SO, Riske B, Bias V, Forsberg A. A model for a regional system of care to promote the health and wellbeing of people with rare chronic genetic disorders. Am J Public Health 2005;95: 1910-6. 16. Hirschman RJ, Itscoitz SB, Shulman NR. Prophylactic treatment of factor VIII deficiency. Blood 1970;35:189-94. 17. Nuss R, Kilcoyne RF, Geraghty S, et al. MRI findings in haemophilic joints treated with radiosynoviorthesis with development of an MRI scale of joint damage. Haemophilia 2000;6:162-9. 18. Pettersson H, Ahlberg A, Nilsson IM. A radiologic classification of hemophilic arthropathy. Clin Orthop Relat Res 1980; 149:153-9. 19. Kasper CK, Aledort L, Aronson D, et al. Proceedings: a more uniform measurement of factor VIII inhibitors. Thromb Diath Haemorr 1975;34:612. 20. Manco-Johnson MJ, Nuss R, Funk S, Murphy J. Joint evaluation instruments for children and adults with haemophilia. Haemophilia 2000;6:649-57. 21. Hacker MR, Funk SM, Manco-Johnson MJ. The Colorado Haemophilia Pedi- atric Joint Physical Examination Scale: normal values and interrater reliability. Haemophilia 2007;13:71-8. 22. Lusher JM. Natural history of inhibitor development in children with severe hemophilia A treated with factor VIII products. In: Lee CA, Berntorp EE, Hoots WK, eds. Textbook of hemophilia. Oxford, EnВ gland: Blackwell, 2005:34-8. 23. Soucie JM, Cianfrini C, Janco RL, et al. Joint range-of-motion limitations among young males with hemophilia: prevalence and risk factors. Blood 2004;103:2467-73. 24. Kreuz W, Escuriola-Ettinghausen C, Funk M, Schmidt H, Kornnhuber B. When should prophylactic treatment in patients with haemophilia A and B start? — the German experience. Haemophilia 1998;4: 413-7. 25. Smith PS, Teutsch SM, Shaffer PA, Rolka H, Evatt B. Episodic versus prophylactic infusions for hemophilia A: a costeffectiveness analysis. J Pediatr 1996;129: 424-31. 26. Globe DR, Curtis RG, Koerper MA. Utilization of care in haemophilia: a resource-based method for cost analysis from the Haemophilia Utilization Group Study (HUGS). Haemophilia 2004;10:Suppl 1: 63-70. 27. Blanchette VS, McCready M, Achonu C, et al. A survey of factor prophylaxis in boys with haemophilia followed in North American haemophilia treatment centers. Haemophilia 2003;9:Suppl 1:19-26. 28. Report on the Universal Data Collection Program. Atlanta: Centers for Disease Control and Prevention, 2005;7(1):28. (Accessed July 18, 2007, at http://www.cdc. gov/ncbddd/hbd/documents/UDC7(1).pdf.) 29. Hacker MR, Geraghty S, Manco-Johnson M. Barriers to compliance with prophylaxis therapy in haemophilia. Haemophilia 2001;7:392-6. Copyright В© 2007 Massachusetts Medical Society. receive immediate notification when a journal article is released early To be notified when an article is released early on the Web and to receive the table of contents of the Journal by e-mail every Wednesday evening, sign up through our Web site at www.nejm.org 544 n engl j med 357;6  www.nejm.org  august 9, 2007 The n e w e ng l a n d j o u r na l of m e dic i n e original article A Single Cycle of Rituximab for the Treatment of Severe Pemphigus Pascal Joly, M.D., Ph.D., Hugo Mouquet, Ph.D., Jean-Claude Roujeau, M.D., Michel D’Incan, M.D., Ph.D., DaniГЁle Gilbert, Ph.D., Serge Jacquot, M.D., Ph.D., Marie-Lise Gougeon, Ph.D., Christophe Bedane, M.D., Ph.D., Ralf Muller, Ph.D., Brigitte Dreno, M.D., Ph.D., Marie-Sylvie Doutre, M.D., Ph.D., Emmanuel Delaporte, M.D., Ph.D., Christine Pauwels, M.D., Nathalie Franck, M.D., FrГ©dГ©ric Caux, M.D., Ph.D., Catherine Picard, M.D., Ph.D., Emmanuelle Tancrede-Bohin, M.D., Philippe Bernard, M.D., Ph.D., FranГ§ois Tron, M.D., Ph.D., Michael Hertl, M.D., Ph.D., and Philippe Musette, M.D., Ph.D. A bs t r ac t Background The combination of multiple cycles of rituximab and intravenous immune globulins has been reported to be effective in patients with severe pemphigus. The aim of this study was to assess the efficacy of a single cycle of rituximab in severe types of pemphigus. Methods We studied 21 patients with pemphigus whose disease had not responded to an 8-week course of 1.5 mg of prednisone per kilogram of body weight per day (corticosteroidrefractory disease), who had had at least two relapses despite doses of prednisone higher than 20 mg per day (corticosteroid-dependent disease), or who had severe contraindications to corticosteroids. The patients were treated with four weekly infusions of 375 mg of rituximab per square meter of body-surface area. The primary end point was complete remission 3 months after the end of rituximab treatment; complete remission was defined as epithelialization of all skin and mucosal lesions. Results Eighteen of 21 patients (86%; 95% confidence interval, 64 to 97%) had a complete remission at 3 months. The disease relapsed in nine patients after a mean of 18.9В±7.9 months. After a median follow-up of 34 months, 18 patients (86%) were free of disease, including 8 who were not receiving corticosteroids; the mean prednisone dose decreased from 94.0В±10.2 to 12.0В±7.5 mg per day (P = 0.04) in patients with corticosteroid-refractory disease and from 29.1В±12.4 to 10.9В±16.5 mg per day (P = 0.007) in patients with corticosteroid-dependent disease. Pyelonephritis developed in one patient 12 months after rituximab treatment, and one patient died of septicemia 18 months after rituximab treatment. These patients had a profound decrease in the number of circulating B lymphocytes but normal serum levels of IgG. From Rouen University Hospital, Rouen (P.J., P.M.); INSERM UnitГ© 519, Rouen UniВversity Hospital, Rouen (P.J., H.M., D.G., S.J., F.T., P.M.); Henri Mondor University Hospital, CrГ©teil (J.-C.R.); ClermontFerrand University Hospital, ClermontFerrand (M.D.); Pasteur Institute, Paris (M.-L.G.); Limoges University Hospital, Limoges (C.B.); Nantes University Hospital, Nantes (B.D.); Bordeaux University Hospital, Bordeaux (M.-S.D.); Lille University Hospital, Lille (E.D.); Poissy–Saint Germain-en-Laye Intercommunal Hospital, Saint Germain-en-Laye (C. Pauwels); Paris V University, Paris (N.F.); Paris XIII University Hospital, Bobigny (F.C.); Bichat University Hospital, Paris (C. Picard); Paris X University Hospital, Paris (E.T.-B.); and Reims University Hospital, Reims (P.B.) — all in France; and the Faculty of Medicine, Philipp University, Marburg, Germany (R.M., M.H.). Address reprint requests to Dr. Joly at the Clinique ВDermatologique, HГґpital Charles Nicolle, 1 rue de Germont, 76031 Rouen CEDEX, France, or at Pascal.Joly@chu-rouen.fr. N Engl J Med 2007;357:545-52. Copyright В© 2007 Massachusetts Medical Society. Conclusions A single cycle of rituximab is an effective treatment for pemphigus. Because of its potentially severe side effects, its use should be limited to the most severe types of the disease. (ClinicalTrials.gov number, NCT00213512.) n engl j med 357;6  www.nejm.org  august 9, 2007 545 The n e w e ng l a n d j o u r na l P emphigus is a life-threatening autoimmune blistering disease affecting the skin and mucosa. It is mediated by pathogenic autoantibodies directed against desmoglein 1 and desmoglein 3, adhesion molecules of the epidermis that are responsible for the cohesion between keratinocytes in skin and mucosa, respectively.1-3 Patients with severe pemphigus require long-term treatment with corticosteroids and other immunosuppressive drugs, which can lead to serious adverse events.4,5 Rituximab, a monoclonal antibody directed against the CD20 antigen of B lymphocytes, has been demonstrated to be effective in various autoimmune diseases6-12 and in occasional cases of life-threatening pemphigus.13-22 Recently, the combination of multiple cycles of rituximab and intravenous immune globulin, another potentially active agent in pemphigus, was reported to be effective in a single-center study of 11 patients with pemphigus.23 We report a multicenter series of 21 patients with severe pemphigus treated by a simple regimen of one cycle of rituximab. Immunologic evaluations explored the mechanism of the shortterm and long-term effects of rituximab on these patients. Me thods 546 of m e dic i n e Treatment The patients were treated with one cycle of four weekly infusions of rituximab at a dose of 375 mg per square meter of body-surface area on days 1, 8, 15, and 22. Corticosteroids were maintained at the initial dose until the disease was controlled, and the corticosteroid dose was then reduced by 10% twice a month. Patients with contraindications to corticosteroids were treated with rituximab alone. Complete remission was defined as the epithelialization of all skin and mucosal lesions, partial remission as the epithelialization of more than 50% of lesions but not of all lesions, and relapse as the occurrence of new cutaneous or mucosal erosions. End Points The patients were evaluated clinically and biologically every month during the first year of followup and every other month during the second year. The primary end point was the rate of complete remission 3 months after the last infusion of rituximab. The secondary end points were the rate of complete remission during the study period, the time from the start of rituximab treatment to complete remission, the number of relapses and the length of time to each relapse, and adverse effects of treatment. Patients Immunologic evaluation Thirteen centers in France participated in this prospective, open trial. The study was approved by the ethics committee of Seine-Maritime, and written informed consent was obtained from each patient. Consecutive patients with severe mucosal erosions, superficial blisters, or both suggestive of pemphigus vulgaris or pemphigus foliaceus; a histologic picture of intraepidermal acantholysis; and deposition of IgG, complement component 3 (C3), or both on the keratinocyte membrane detected by direct immunofluorescence24 were included if additional criteria were met. These were the absence of response to an 8-week course of treatment with 1.5 mg of prednisone per kilogram of body weight per day (corticosteroid-refractory cases); the occurrence of at least two cutaneous or mucosal relapses during the period when corticosteroid doses were being decreased, despite prednisone doses higher than 20 mg per day (corticosteroiddependent cases); and contraindication to corticosteroids because of severe associated medical conditions. Blood samples were collected at each evaluation. Titers of antibodies against desmoglein 1 and desmoglein 3 were measured by a desmoglein enzyme-linked immunosorbent assay (ELISA) test (MESACUP Desmoglein Test, MBL Medical and Biological Laboratories) with 1:100 diluted serum. For determination of IgG subclass, mouse antihuman IgG1, IgG2, IgG3, and IgG4 antibodies (Sigma) and peroxidase-conjugated goat antimouse IgG (Rockland) were used. IgG reactivity of pemphigus vulgaris serum against the NH2 terminal domains of desmoglein 3 was characterized with the use of ELISA with baculovirus-derived recombinant proteins of desmoglein 3.25 The phenotype of peripheral-blood mononuclear cells was determined by three-color flow cytometry with the use of murine monoclonal antibodies against CD3, CD4, CD5, CD19, CD20, CD21, CD22, CD23, CD24, CD27, CD38, CD56, and CD86 (Coulter). The IgG, IgA, and IgM repertoire of peripheral-blood B lymphocytes was determined with the use of the immunoscope technique, a method that evaluates the diversity of the n engl j med 357;6  www.nejm.org  august 9, 2007 Rituximab for the Treatment of Severe Pemphigus B-lymphocyte repertoire and monitors its evolution. First, a polymerase chain reaction amplified the heavy-chain variable (HV) region of the IgG, IgA, and IgM molecules. In a second step, the lengths of the complementary determining region 3 (CDR3) were analyzed on an automatic sequencer.26 The serum levels of antibodies against pneumococcal capsule polysaccharide and tetanus toxin were determined on days 0, 90, and 180.27 Statistical Analysis Two-sided P values less than 0.05 were considered to indicate statistical significance. Continuous variables are expressed as means В±SD. Mean doses of prednisone were compared with the use of the nonparametric Wilcoxon test. Roche, France (the maker of rituximab) had no role in the design of the study, in data accrual or analysis, or in manuscript preparation. R e sult s Characteristics of the Patients Twenty-one patients (14 men and 7 women; 14 with pemphigus vulgaris and 7 with pemphigus foliaceus) were enrolled between January 2003 and December 2004 and followed through March 2007. Their mean (В±SD) age was 53.7В±15.6 years. The baseline clinical characteristics of the patients are shown in Table 1. The mean proportion of the body-surface area involved was 27%. All the patients had severe oral involvement and weight loss Table 1. Baseline Characteristics of Patients with Pemphigus Treated with Rituximab.* Characteristic Sex (M/F) Age (yr) CorticosteroidRefractory Disease (N = 5)†CorticosteroidDependent Disease (N = 11) Contraindication to Corticosteroids (N = 5) 2/3 7/4 5/0 56.2В±18.9 47.5В±13.1 64.6В±19.7 4 7 Type of pemphigus (no. of patients) Pemphigus vulgaris Pemphigus foliaceus 3 1 4 Duration of mucosal lesions (mo) 21.8В±30.5 81.0В±82.7 12.5В±7.8 2 Duration of cutaneous lesions (mo) 54.6В±62.3 71.0В±75.0 8.0В±6.9 Diabetes mellitus 1 3 2 Hypertension 0 3 2 Hyperlipidemia 0 3 2 Other‡ 1 6 6 Associated medical conditions (no. of patients) Previous treatment failure (no. of patients) Intravenous immune globulin 2 1 Azathioprine 4 3 Methotrexate 2 3 Mycophenolate mofetil 0 4 Cyclosporine Mean body-surface area involved (%) Prednisone dose at time of rituximab infusion (mg/day) 0 1 30 31 17 94.0В±10.2 29.1В±12.4 0 *Plus–minus values are means В±SD. †Corticosteroid-refractory pemphigus did not respond to an 8-week course of treatment with 1.5 mg of prednisone per kilogram of body weight per day. ‡Other medical conditions included asthma in one patient with corticosteroid-refractory pemphigus; rheumatoid arthritis (one patient), myopathy (one), bone fracture (one), pyelonephritis (one), and depression (two) among patients with corticosteroid-dependent disease; and blindness, bacterial meningitis, bone tuberculosis, gram-negative pneumonia, osteonecrosis of the hip, and cardiac insufficiency, each in one patient, among those with contraindications to corticosteroids. n engl j med 357;6  www.nejm.org  august 9, 2007 547 n e w e ng l a n d j o u r na l The of m e dic i n e Table 2. Complete Remission 3 Months after Rituximab Treatment in Patients with Severe Pemphigus.* Pemphigus Vulgaris (N = 14) Group Pemphigus Foliaceus (N = 7) Total (N = 21) no. with remission/total no. Corticosteroid-refractory disease 4/4 0/1 4/5 Corticosteroid-dependent disease 6/7 4/4 10/11 Contraindication to corticosteroids 2/3 2/2 4/5 12/14 6/7 18/21 Total *Complete remission was defined as epithelialization of all skin and mucosal lesions. of up to 10 kg. In addition, seven patients had severe involvement of one or more other mucosae, including the genital, anal, conjunctival, or pharyngeal mucosae or a combination of these. All patients with corticosteroid-refractory disease and all patients with corticosteroid-dependent disease had been treated previously with various immunosuppressive drugs, intravenous immune globulins, or both without success. The duration of all systemic therapy before study entry ranged from 4 to 168 months (mean, 70.2). Severe associated medical conditions or side effects of corticosteroids were present at baseline in 14 patients (67%). Five patients were treated with rituximab alone because they had contraindications to corticosteroid use. Corticosteroids were contraindicated in two patients because of severe diabetes mellitus, arterial hypertension, or both; in two patients because of a history of severe infection, osteonecrosis of the hip, or both; and in one patient because of old age (84 years) and poor general condition (Table 1). Response to rituximab treatment Eighteen of 21 patients (86%; 95% confidence interval, 64 to 94) had a complete remission at 3 months, including 12 of 14 patients with pemphigus vulgaris and 6 of 7 with pemphigus foliaceus (Table 2). Two patients with pemphigus vulgaris had a delayed complete remission on days 180 and 360 (Fig. 1). One patient with pemphigus foliaceus with lesions that initially involved the entire body surface was only slightly improved after rituximab, and treatment of this patient was considered to have failed. All the other patients (95%) had a complete remission at some time during the study period. The median delays to partial and complete remission are shown in Table 3. Of the 20 patients who had a complete remission, 9 (6 with pemphigus vulgaris and 3 with 548 pemphigus foliaceus) had a relapse after a mean period of 18.9В±7.9 months. Three patients with corticosteroid-dependent disease had a total of six relapses. Of the nine patients who had a relapse, three were treated with topical corticosteroids only, four with a moderately increased dose of oral corticosteroids, and two with a second course of rituximab. The second course of rituximab was chosen because one of the two patients was 84 years old and was thought to be at high risk for complications from corticosteroids, and the other had a severe relapse. Both patients had a complete remission again. After a median follow-up time of 34 months (range, 26 to 45), 18 patients (86%) were free of disease, including 8 patients (38%) who received no more corticosteroids. The mean dose of prednisone for patients with corticosteroid-refractory disease decreased from 94.0В±10.2 mg per day at baseline to 12.0В±7.5 mg per day at the end of the study (P = 0.04) (Fig. 1). The mean dose of prednisone for patients with corticosteroid-dependent disease decreased from 29.1В±12.4 mg per day at baseline to 10.9В±16.5 mg Figure 1 (facing page). Changes in Clinical Lesions, Antidesmoglein Antibodies, and Doses of Prednisone in Patients with Pemphigus Treated with Rituximab. Panel A shows cutaneous lesions (blue) and mucosal lesions (orange) in patients with pemphigus vulgaris; Panel B shows cutaneous lesions (blue) and no mucosal lesions in patients with pemphigus foliaceus. Arrows point to the number of days after rituximab treatment at which a relapse occurred; patients were treated on day 0. Panel C shows serum levels of anti–desmoglein 1 antibodies (blue) and anti–desmoglein 3 antibodies (orange) in patients with pemphigus vulgaris. Panel D shows serum levels of anti–desmoglein 1 antibodies (blue) and no anti–desmoglein 3 antibodies in patients with pemphigus foliaceus. Panels E and F show doses of prednisone in patients with pemphigus vulgaris and in those with pemphigus foliaceus, respectively. n engl j med 357;6  www.nejm.org  august 9, 2007 0 0 60 0 20 40 60 80 100 120 0 0 100 200 300 400 Days 120 180 240 300 360 420 480 540 600 660 720 Days Days 549 EMail CASE REG F ICM ARTIST: sw FIGURE: 1 of 1 AUTHOR: Joly 120 240 360 480 600 720 840 960 1080 1200 1320 1440 E Pemphigus vulgaris 0 50 100 150 200 250 300 Partial Remission Baseline Complete Remission 120 240 360 480 600 720 840 960 1080 1200 1320 1440 C Pemphigus vulgaris 0 20 40 60 80 Mucosal Lesions Anti–Desmoglein 3 Antibody Titer (U/ml) 100 Skin Lesions 0 Line H/T 0 60 4-C H/T SIZE 36p6 Revised RETAKE 0 1st 2nd 3rd 0 20 40 60 80 100 120 Days 120 180 240 300 360 420 480 540 600 660 720 Days Days 120 240 360 480 600 720 840 960 1080 1200 1320 1440 F Pemphigus foliaceus 0 50 100 150 200 250 300 Partial Remission Baseline Mucosal Lesions Complete Remission 120 240 360 480 600 720 840 960 1080 1200 1320 1440 D Pemphigus foliaceus 0 20 40 60 80 100 Skin Lesions B Pemphigus foliaceus Body-Surface Area Involved (%) Anti–Desmoglein 1 Antibody Titer (U/ml) Body-Surface Area Involved (%) Anti–Desmoglein 1 Antibody Titer (U/ml) Prednisone Dose (mg/day) n engl j med 357;6  www.nejm.org  august 9, 2007 Prednisone Dose (mg/day) A Pemphigus vulgaris Rituximab for the Treatment of Severe Pemphigus The n e w e ng l a n d j o u r na l Table 3. Median Time to Partial and Complete Remission in Patients with Pemphigus Treated with Rituximab. Pemphigus Vulgaris (N = 14) Type of Remission Pemphigus Foliaceus (N = 7) median no. of days to remission (interquartile range) Partial remission Cutaneous lesions 15 (15–30) 30 (30–56) Mucosal lesions 60 (30–60) — Cutaneous lesions 30 (30–60) 60 (60–90) Mucosal lesions 90 (60–90) — Complete remission per day at the end of the study (P = 0.007). Nine patients reported minor and transient side effects during rituximab infusion: headache in three patients, asthenia in three, fever in one, chills in one, and nausea in one. In addition, two severe side effects were observed: one patient had pyeloВ nephritis 12 months after rituximab treatment, and one patient died from septicemia 18 months after rituximab treatment. The patient who died also had rheumatoid arthritis and was concomitantly treated with the anti–tumor necrosis factor agent etanercept. Immunologic evaluations Peripheral-blood B- and T-lymphocyte subpopulations and T-lymphocyte cytokine production were analyzed longitudinally. The B-cell count decreased dramatically from a median of 275 cells per cubic millimeter (range, 29 to 752) to 0 cells per cubic millimeter (range, 0 to 1) at day 21 and remained undetectable until day 180 in all but two patients. Reappearance of B cells began between day 180 and day 270. Ninety percent of them expressed a CD19+CD27в€’ phenotype suggestive of naive B lymphocytes. Twenty-nine percent had a CD19+ CD38highCD24high transitional phenotype suggestive of the migration of B cells from the bone marrow to the periphery. No major changes in T cells or natural killer cells or in T-cell cytokine production were detected after rituximab treatment. Using the immunoscope method, we followed the evolution of the repertoire of IgG, IgA, and IgM in blood B lymphocytes in two patients. Before treatment, immunoscope profiles showed some peak expansions in the immunoglobulin HV550 of m e dic i n e region genes (IgVH3a, IgVH3b, and IgVH4), the most represented ones, reflecting in vivo antigen-driven responses. Six months later, reappearing blood B cells showed a typical gaussian distribution of the CDR3 lengths for these IgVH families, similar to that found in the naive B cells of cord blood, suggesting the reconstitution of a diverse B-cell repertoire (data not shown). Antidesmoglein autoantibody response was then analyzed. A dramatic decrease of IgG and IgG4 anti–desmoglein 1 and anti–desmoglein 3 antibodies was observed in 15 of the 18 patients who had a complete remission 3 months after rituximab treatment, whereas persistent high titers were detected in the 2 patients who had a delayed complete remission and in the 1 patient in whom treatment failed. Persistent high titers or rises in anti–desmoglein 1 and anti–desmoglein 3 antibody levels were detected in patients with relapsing disease and, surprisingly, in five patients with pemphigus vulgaris in whom a complete remission was maintained (Fig. 1). To disentangle this discrepancy, we retested serum from these patients on recombinant proteins of five extracellular (EC) domains of desmoglein 3 (EC1 to EC5). Antibodies reacting with epitopes of the EC1 to EC2 domains, which are considered the main pathogenic antibodies,28,29 decreased dramatically after rituximab treatment and remained undetectable until day 540, a result that was in accordance with the absence of mucosal lesions in these patients.30,31 Finally, to assess the influence of rituximab on antimicrobial response, we first determined the serum level of IgG and IgM antibodies. No significant change in mean IgG levels was observed after rituximab treatment (P = 0.79). On the contrary, mean IgM levels decreased from 1.5В±1.1 g per liter at baseline to 1.1В±0.9 g per liter on day 180 and 1.0В±0.7 g per liter on day 360 (P = 0.003). We then determined that the levels of antibodies against pneumococcal capsule polysaccharide and the levels of antibodies against tetanus toxin were not significantly altered between baseline, day 21, and day 90. The two patients who had severe infections, one at 12 months after rituximab treatment and one at 18 months, had normal serum IgG levels (21 g per liter and 13.5 g per liter, respectively), despite low numbers of circulating B lymphocytes (5 per cubic millimeter and 9 per cubic millimeter, respectively) at the times of their infections. n engl j med 357;6  www.nejm.org  august 9, 2007 Rituximab for the Treatment of Severe Pemphigus Dis cus sion Our study demonstrated the efficacy of rituximab for severe pemphigus; 86% of patients were in complete remission 3 months after receiving four weekly infusions of rituximab. After a 34-month followup period, 18 patients were free of disease, and 8 of these patients were not receiving any systemic therapy. Overall, treatment with rituximab both resulted in major clinical improvement and permitted a large decrease in the doses of corticosteroids. Our results were similar to those recently reported by Ahmed et al.,23 who obtained a complete remission in 9 of 11 patients (82%). Our patients were treated with one cycle of four weekly infusions of rituximab, and the patients in the study by Ahmed et al. were treated with two induction cycles of rituximab, followed by consolidation therapy and six infusions of intravenous immune globulins, another potentially active agent in pemphigus.23,32,33 Therefore, we believe multiple cycles of rituximab may not be necessary. Accordingly, we suggest restricting the use of additional cycles of rituximab to the few relapses that cannot be adequately controlled with conventional treatments. Two severe side effects were observed in our study: pyelonephritis developed in one patient 12 months after rituximab treatment, and one patient died from septicemia 18 months after rituximab treatment. It is important to emphasize that rituximab treatment is associated with a risk of death from severe side effects, such as pneumocystis infection, toxic epidermal necrolysis, and progressive multifocal leukoencephalopathy.34,35 The risk of serious infection led Ahmed et al. to propose combining intravenous immune globulins with rituximab during the first 6 months of treatment with rituximab.23 We do not think that 6 months of treatment with immune globulins would have prevented the two serious infections observed in our study, which occurred at 12 and 18 months in patients who had no defect in IgG serum levels or in preformed antibacterial antibodies. It is not known whether the addition of intravenous imReferences 1. Stanley JR. Pemphigus and pemphigoid as paradigms of organ-specific, autoantibody-mediated diseases. J Clin Invest 1989;83:1443-8. 2. Stanley JR. Cell adhesion molecules as targets of autoantibodies in pemphigus and pemphigoid, bullous diseases due to mune globulins to rituximab reduces the risk of serious infections.36,37 Immunologic investigations demonstrated that one cycle of rituximab induced a prolonged depletion of peripheral-blood B lymphocytes, followed by the reappearance of B cells with a naive phenotype similar to that found in cord blood from neonates. Rituximab induced a modification of the repertoire of B cells, with the disappearance of the initially expanded populations and the reconstitution of a diverse B-cell repertoire that might account for its long-lasting effect. The clinical response to rituximab in patients with pemphigus foliaceus was closely related to the evolution of anti–desmoglein 1 antibodies, which dramatically decreased in patients who had a complete remission, whereas we were surprised to observe persistently high levels of anti–desmoglein 3 antibodies in a few patients in whom pemphigus vulgaris was in complete remission. The dissociation between anti–desmoglein 1 and anti– desmoglein 3 antibody responses, as well as the absence of major modification of serum levels of antibodies against pneumococcal and tetanustoxin antigens, suggested some specificity of rituximab for the autoreactive B-cell response.38,39 One hypothesis is that rituximab would differentially affect the turnover of short-life and long-life plasma cells that produce antibodies directed against desmoglein 1 and desmoglein 3.40 Overall, our study suggests that rituximab is a very effective treatment for severe pemphigus. Larger series with a longer follow-up are needed to assess the long-term risks of this treatment. Supported by the French Society of Dermatology, Paris, and by Roche, France. Presented in part at the December 2006 Congress of the French Society of Dermatology and at the September 2006 Congress of the European Society of Dermatological Research (ESDR), both in Paris. No potential conflict of interest relevant to this article was reported. We thank Marie-France Hellot for her help with the statistical analysis, Vincent Ferranti for monitoring the study, Ken Wood for assistance in editing an earlier version of the manuscript, and Nathalie Jourdain for excellent secretarial assistance. defective epidermal cell adhesion. Adv Immunol 1993;53:291-325. 3. Amagai M, Klaus-Kovtun V, Stanley JR. Autoantibodies against a novel epithelial cadherin in pemphigus vulgaris, a disease of cell adhesion. Cell 1991;67: 869-77. 4. Bystryn JC, Steinman NM. The adju- vant therapy of pemphigus: an update. Arch Dermatol 1996;132:203-12. 5. McDonald CJ. Cytotoxic agents for use in dermatology. J Am Acad Dermatol 1985;12:753-75. 6. Kazkaz H, Isenberg D. Anti B cell ther- n engl j med 357;6  www.nejm.org  august 9, 2007 551 Rituximab for the Treatment of Severe Pemphigus apy (rituximab) in the treatment of autoimmune diseases. Curr Opin Pharmacol 2004; 4:398-402. 7. Stasi R, Stipa E, Forte V, Meo P, Amadori S. Variable patterns of response to rituximab treatment in adults with chronic idiopathic thrombocytopenic purpura. Blood 2002;99:3872-3. 8. Narat S, Gandla J, Hoffbrand AV, Hughes RG, Mehta AB. Rituximab in the treatment of refractory autoimmune cytopenias in adults. Haematologica 2005;90: 1273-4. 9. Zaja F, De Vita S, Russo D, et al. Rituximab for the treatment of type II mixed cryoglobulinemia. Arthritis Rheum 2002;46:2252-4. 10. Specks U, Fervenza FC, McDonald TJ, Hogan MC. Response of Wegener’s granulomatosis to anti-CD20 chimeric monoclonal antibody therapy. Arthritis Rheum 2001;44:2836-40. 11. Levine TD. Rituximab in the treatment of dermatomyositis: an open-label pilot study. Arthritis Rheum 2005;52:601-7. 12. Arzoo K, Sadeghi S, Liebman HA. Treatment of refractory antibody mediated autoimmune disorders with an antiCD20 monoclonal antibody (rituximab). Ann Rheum Dis 2002;61:922-4. 13. Dupuy A, Viguier M, Bedane C, et al. Treatment of refractory pemphigus vulgaris with rituximab (anti-CD20 monoclonal antibody). Arch Dermatol 2004;140: 91-6. 14. Espana A, Fernandez-Galar M, Lloret P, Sanchez-Ibarrola A, Panizo C. Long-term complete remission of severe pemphigus vulgaris with monoclonal anti-CD20 antibody therapy and immunophenotype correlations. J Am Acad Dermatol 2004;50: 974-6. 15. Morrison LH. Therapy of refractory pemphigus vulgaris with monoclonal antiCD20 antibody (rituximab). J Am Acad Dermatol 2004;51:817-9. 16. Wenzel J, Bauer R, Bieber T, Tuting T. Successful rituximab treatment of severe pemphigus vulgaris resistant to multiple immunosuppressants. Acta Derm Venereol 2005;85:185-6. 17. Schmidt E, Herzog S, Brocker EB, Zillikens D, Goebeler M. Long-standing remission of recalcitrant juvenile pemphigus vulgaris after adjuvant therapy with rituximab. Br J Dermatol 2005;153:449-51. 18. Arin MJ, Engert A, Krieg T, Hunzel- mann N. Anti-CD20 monoclonal antibody (rituximab) in the treatment of pemphigus. Br J Dermatol 2005;153:620-5. 19. Kong HH, Prose NS, Ware RE, Hall RP III. Successful treatment of refractory childhood pemphigus vulgaris with antiCD20 monoclonal antibody (rituximab). Pediatr Dermatol 2005;22:461-4. 20. Herrmann G, Hunzelmann N, Engert A. Treatment of pemphigus vulgaris with anti-CD20 monoclonal antibody (rituximab). Br J Dermatol 2003;148:602-3. 21. Goebeler M, Herzog S, Brocker EB, Zillikens D. Rapid response of treatmentresistant pemphigus foliaceus to the antiCD20 antibody rituximab. Br J Dermatol 2003;149:899-901. 22. El Tal AK, Posner MR, Spigelman Z, Ahmed AR. Rituximab: a monoclonal antibody to CD20 used in the treatment of pemphigus vulgaris. J Am Acad Dermatol 2006;55:449-59. 23. Ahmed AR, Spigelman Z, Cavacini LA, Posner MR. Treatment of pemphigus vulgaris with rituximab and intravenous immune globulin. N Engl J Med 2006; 355:1772-9. 24. Lever WF. Pemphigus and pemphigoid: a review of the advances made since 1964. J Am Acad Dermatol 1979;1:2-31. 25. MГјller R, Svoboda V, Wenzel E, et al. IgG reactivity against non-conformational NH2-terminal epitopes of the desmoglein 3 ectodomain relates to clinical activity and phenotype of pemphigus vulgaris. Exp Dermatol 2006;15:606-14. 26. Lim A, Lemercier B, Werth X, Lesjean Pottier S, Huetz F, Kourilsky P. Most human peripheral blood B cells display a unique heavy chain rearrangement. Int Immunol (in press). 27. Ballet JJ, Sulcebe G, Couderc LJ, et al. Impaired anti-pneumococcal antibody response in patients with AIDS-related persistent generalized lymphadenopathy. Clin Exp Immunol 1987;68:479-87. 28. Anzai H, Fujii Y, Nishifuji K, et al. Conformational epitope mapping of antibodies against desmoglein 3 in experimental murine pemphigus vulgaris. J Dermatol Sci 2004;35:133-42. 29. Sekiguchi M, Futei Y, Fujii Y, Iwasaki T, Nishikawa T, Amagai M. Dominant autoimmune epitopes recognized by pemphigus antibodies map to the N-terminal adhesive region of desmogleins. J Immunol 2001;167:5439-48. 30. Hacker MK, Janson M, Fairley JA, Lin MS. Isotypes and antigenic profiles of pemphigus foliaceus and pemphigus vulgaris. Clin Immunol 2002;105:64-74. 31. Amagai M, Komai A, Hashimoto T, et al. Usefulness of enzyme-linked immunosorbent assay using recombinant desmoВ gleins 1 and 3 for serodiagnosis of pemphigus. Br J Dermatol 1999;140:351-7. 32. Ahmed AR. Treatment of autoimmune mucocutaneous blistering diseases with intravenous immunoglobulin therapy. Expert Opin Investig Drugs 2004;13:1019-32. 33. Ahmed AR, Dahl MV. Consensus statement on the use of intravenous immunoglobulin therapy in the treatment of autoimmune mucocutaneous blistering diseases. Arch Dermatol 2003;139:10519. 34. Bermudez A, Marco F, Conde E, Mazo E, Recio M, Zubizaretta A. Fatal varicellazoster infection following rituximab and chemotherapy treatment in a patient with follicular lymphoma. Haematologica 2000; 85:894-5. 35. Quartier P, Tournilhac O, Archimbaud C, et al. Enteroviral meningoencephalitis after anti-CD20 (rituximab) treatment. Clin Infect Dis 2003;36:e47-e49. 36. Lehrnbecher T. Intravenous immunoglobulins in the prevention of infection in children with hematologic-oncologic diseases. Klin Padiatr 2001;213:Suppl 1:A103A105. (In German.) 37. Sullivan KM, Kopecky KJ, Jocom J, et al. Immunomodulatory and antimicrobial efficacy of intravenous immunoglobulin in bone marrow transplantation. N Engl J Med 1990;323:705-12. 38. Smith MR. Rituximab (monoclonal anti-CD20 antibody): mechanism of action and resistance. Oncogene 2003;22: 7359-68. 39. Maloney DG, Smith B, Rose A. Rituximab: mechanism of action and resistance. Semin Oncol 2002;29:Suppl 2:2-9. 40. Hoyer BF, Manz RA, Radbruch A, Hiepe F. Long-lived plasma cells and their contribution to autoimmunity. Ann N Y Acad Sci 2005;1050:124-33. Copyright В© 2007 Massachusetts Medical Society. full text of all journal articles on the world wide web Access to the complete text of the Journal on the Internet is free to all subscribers. To use this Web site, subscribers should go to the Journal’s home page (www.nejm.org) and register by entering their names and subscriber numbers as they appear on their mailing labels. After this one-time registration, subscribers can use their passwords to log on for electronic access to the entire Journal from any computer that is connected to the Internet. Features include a library of all issues since January 1993 and abstracts since January 1975, a full-text search capacity, and a personal archive for saving articles and search results of interest. All articles can be printed in a format that is virtually identical to that of the typeset pages. Beginning 6 months after publication, the full text of all Original Articles and Special Articles is available free to nonsubscribers who have completed a brief registration. 552 n engl j med 357;6  www.nejm.org  august 9, 2007 The n e w e ng l a n d j o u r na l of m e dic i n e original article Complement C3 Variant and the Risk of Age-Related Macular Degeneration John R.W. Yates, F.R.C.P., Tiina Sepp, Ph.D., Baljinder K. Matharu, M.Sc., Jane C. Khan, F.R.C.Ophth., Deborah A. Thurlby, R.G.N., M.Sc., Humma Shahid, M.R.C.Ophth., David G. Clayton, M.A., Caroline Hayward, Ph.D., Joanne Morgan, B.Sc., Alan F. Wright, Ph.D., F.R.C.P., Ana Maria Armbrecht, Ph.D., F.R.C.S., Baljean Dhillon, F.R.C.S., F.R.C.Ophth., Ian J. Deary, Ph.D., F.R.C.P.E., Elizabeth Redmond, R.G.N., M.Sc., Alan C. Bird, M.D., F.R.C.S., and Anthony T. Moore, F.R.C.S., F.R.C.Ophth., for the Genetic Factors in AMD Study Group* A bs t r ac t Background Age-related macular degeneration is the most common cause of blindness in Western populations. Susceptibility is influenced by age and by genetic and environmental factors. Complement activation is implicated in the pathogenesis. Methods We tested for an association between age-related macular degeneration and 13 singlenucleotide polymorphisms (SNPs) spanning the complement genes C3 and C5 in case subjects and control subjects from the southeastern region of England. All subjects were examined by an ophthalmologist and had independent grading of fundus photographs to confirm their disease status. To test for replication of the most significant findings, we genotyped a set of Scottish cases and controls. Results The common functional polymorphism rs2230199 (Arg80Gly) in the C3 gene, corresponding to the electrophoretic variants C3S (slow) and C3F (fast), was strongly associated with age-related macular degeneration in both the English group (603 cases and 350 controls, P = 5.9Г—10–5) and the Scottish group (244 cases and 351 controls, P = 5.0Г—10–5). The odds ratio for age-related macular degeneration in C3 S/F heterozygotes as compared with S/S homozygotes was 1.7 (95% confidence interval [CI], 1.3 to 2.1); for F/F homozygotes, the odds ratio was 2.6 (95% CI, 1.6 to 4.1). The estimated population attributable risk for C3F was 22%. Conclusions Complement C3 is important in the pathogenesis of age-related macular degeneration. This finding further underscores the influence of the complement pathway in the pathogenesis of this disease. n engl j med 357;6  www.nejm.org  august 9, 2007 From the Cambridge Institute for Medical Research, University of Cambridge, Cambridge (J.R.W.Y., T.S., B.K.M., J.C.K., D.A.T., H.S., D.G.C.); the Medical Research Council Human Genetics Unit, Edinburgh (C.H., J.M., A.F.W.); the Princess Alexandra Eye Pavilion, Edinburgh (A.M.A., B.D.); the University of Edinburgh, Edinburgh (I.J.D.); the Institute of Ophthalmology, University College London (E.R., A.C.B., A.T.M.); and Moorfields Eye Hospital, London (A.C.B., A.T.M.) — all in the United Kingdom. Address reprint requests to Dr. Yates at the Department of Medical Genetics, University of Cambridge, Cambridge Institute for Medical Research, Wellcome Trust/MRC Bldg., Box 139, Addenbrooke’s Hospital, Cambridge CB2 0XY, United Kingdom, or at jrwy1@cam. ac.uk. Drs. Yates and Sepp contributed equally to this article. *Other members of the Genetic Factors in Age-Related Macular Degeneration (AMD) Study Group are listed in the Appendix. This article (10.1056/NEJMoa072618) was published at www.nejm.org on July 18, 2007. N Engl J Med 2007;357:553-61. Copyright В© 2007 Massachusetts Medical Society. 553 The A  n e w e ng l a n d j o u r na l ge-related macular degeneration is the leading cause of visual impairment in the elderly and the most common cause of blindness in Western countries.1 It affects the macular region of the retina. The macula has a high density of photoreceptors and provides detailed central vision. In the early stages of the disease (referred to as age-related maculopathy), deposits called drusen develop between the retinal pigment epithelium and underlying choroid.1 Later, the disease is manifested as either extensive atrophy of the retinal pigment epithelium and overlying photoreceptor cells (geographic atrophy) or aberrant choroidal angiogenesis (choroidal neovascularization).1 Both of these conditions can lead to a loss of central vision. The pathogenesis of age-related macular degeneration is poorly understood. As with other late-onset chronic diseases, susceptibility is influenced by age, ethnic background, and a combination of environmental and genetic factors.1,2 Smoking status and family history are well-established determinants of risk.1,2 Recently, polymorphisms in the genes coding for complement factor H (CFH) and complement factor B (CFB) have been shown to be predictors of risk for age-related macular degeneration.3-11 Another susceptibility locus has been mapped to chromosome 10q26; the causative variation probably lies in a hypothetical gene called LOC387715 or in the promoter of the neighboring gene HTRA1.11-14 The population attributable risk associated with variants in CFH, CFB, and LOC387715/ HTRA1 is at least 50%.11 CFH and CFB are key components of the alternative complement pathway. Their involvement in age-related macular degeneration, together with the finding that drusen contain proteins associated with inflammation and immune-mediated processes,15 supports the hypothesis that inflammation and complement activation influence the pathogenesis of age-related macular degeneration. To test whether variants in other genes encoding proteins in the complement pathway influence susceptibility to age-related macular degeneration, we genotyped single-nucleotide polymorphisms (SNPs) spanning the complement genes C3 and C5, encoding central proteins in the complement cascade, in subjects with age-related macular degeneration and in control subjects. 554 of m e dic i n e Me thods Cases and Controls We studied three case–control groups, two in EnВ gland and one in Scotland. English group 1 comprised 446 case subjects with end-stage age-related macular degeneration (geographic atrophy or choroidal neovascularization) and 267 control subjects, who were spouses of the index patients. All subjects were recruited from ophthalmic clinics in eight hospitals in southeastern England from 2002 to 2004.7 English group 2 comprised 157 case subjects with end-stage age-related macular degeneration and 83 controls (67 spouses and 16 friends of index patients) recruited from 2003 to 2005, the majority from Moorfields Eye Hospital in London and the remainder from southeastern England. All subjects described themselves as “white” rather than “other” on a recruitment questionnaire. The Scottish group comprised 505 case subjects with age-related maculopathy or end-stage age-related macular degeneration and 351 control subjects. A total of 337 case subjects from the Lothian region were recruited from ophthalmic clinics in Edinburgh and 46 case subjects from hospitals in Dundee and Inverness from 2004 to 2006. Control subjects, who were recruited from the same sources in similar proportions, comprised 32 spouses and 174 subjects who had undergone cataract surgery. Another 122 case subjects and 145 controls came from the 1921 Lothian birth cohort.16 Written informed consent was obtained from all subjects. The research protocol was in keeping with the provisions of the Declaration of Helsinki, and approval was obtained from a multicenter research ethics committee and from research ethics committees for each institution. Subjects were examined by an ophthalmologist, and data were collected regarding medical history, lifestyle, and smoking history. Color, stereoscopic fundus photography of the macular region was performed in all subjects. For English subjects, the images were graded at the Reading Centre, Moorfields Eye Hospital, with the use of the International Classification of Age-Related Maculopathy and Macular Degeneration.17 For Scottish subjects, a study investigator graded images; for validation, images from 100 case subjects and n engl j med 357;6  www.nejm.org  august 9, 2007 Complement C3 Variant and Age-Related Macular Degener ation controls were independently graded at the Moorfields Reading Centre (kappa statistic, 0.84). Eight prospective English controls with age-related macular degeneration and 60 prospective Scottish controls with age-related maculopathy were reclassified as case subjects. Data on disease status, sex, age, and smoking history of subjects are provided in Table 1. Genotyping We extracted genomic DNA from peripheralblood leukocytes. We selected SNPs spanning the C3 and C5 genes from the International HapMap Project18 data (release 19) for the Centre d’Étude du Polymorphisme Humain (CEPH) population (Utah residents with ancestry from northern and western Europe). Criteria for the selection of SNPs were high heterozygosity with a minor allele frequency of at least 10%, tagging of the most common haplotypes, and coverage of the main blocks of linkage disequilibrium. The C3 SNP rs2230199 — which is predicted to result in a substitution of a glycine residue for arginine at position 80 (Arg80Gly) — generates the “fast” electrophoretic allotype of C3 (called C3F); the alternative allotype is “slow” (C3S).19,20 We included this SNP in the analysis to provide extra coverage and because of evidence of a functional difference between the two alleles. On the basis of our initial analysis, we included rs1047286 (Pro292Leu), which has a known association with rs2230199.20,21 Initial genotyping was carried out in English group 1. Markers of interest were genotyped in group 2 when samples became available. Data from the Scottish group were used for replication. We performed genotyping in English subjects with the use of a single-nucleotide primer extension assay (ABI Prism SNaPshot Multiplex Kit, Applied Biosystems) and a genetic analyzer (ABI Table 1. Disease Status, Sex, Age, and Smoking History of Subjects.* Variable English Subjects (Groups 1 and 2) Controls (N = 350) Case Subjects (N = 603) Scottish Subjects Controls (N = 351) Case Subjects (N = 505) Disease status — no. Age-related maculopathy 0 261 Geographic atrophy 143 55 Choroidal neovascularization 369 189 91 0 Geographic atrophy and choroidal Вneovascularization Sex — no. (%) Male 151 (43) 270 (45) 152 (43) Female 199 (57) 333 (55) 199 (57) 315 (62) 75.3В±7.8 79.4В±7.2 78.0В±8.5 77.8В±9.2 347 595 347 499 Never smoked 141 (41) 214 (36) 161 (46) 240 (48) Current or former smoker 206 (59) 381 (64) 186 (54) 259 (52) 0 pack-yr 141 (41) 214 (36) 0.1–20.0 pack-yr 126 (36) 166 (28) 20.1–40.0 pack-yr 61 (18) 136 (23) >40.0 pack-yr 19 (5) 79 (13) Mean age — yr†190 (38) Smoking history — no. (%) No. of subjects Quantity of cigarettes smoked†*Plus–minus values are means В±SD. †For the English subjects, P<0.001 for the comparisons between case and control subjects. Data on the quantity of cigarettes smoked were not collected for the Scottish subjects. n engl j med 357;6  www.nejm.org  august 9, 2007 555 The n e w e ng l a n d j o u r na l Prism 3100, Applied Biosystems) and in Scottish subjects — for rs2230199 and rs1047286 — with the use of competitive allele-specific polymerasechain-reaction assays (Taqman SNP Genotyping Assay, Applied Biosystems and KASPar SNP Genotyping System, KBiosciences, respectively). Manufacturers’ protocols were followed. Statistical Analysis We used the chi-square test for comparisons of categorical variables and allele and genotype frequencies and to check for Hardy–Weinberg equilibrium. All P values were calculated with two-sided tests, and no correction was made for multiple testing. The Mann–Whitney U test was used to compare the ages of case subjects and controls. Logistic-regression analysis was used to investigate interactions between genotype and other variables and to estimate odds ratios and 95% confidence intervals. The covariables of age and smoking history were included in the logistic model if univariate analysis had shown a significant difference. Odds ratios for categorical variables were estimated in relation to a reference category. Data were analyzed with the use of the SPSS statistical software package, version 11.0. The population attributable risk was calculated from the formula 100D ÷ (1 + D), in which D was equal to P1(RR1 – 1) + P2(RR2 – 1), where P1 and P2 are the frequencies of the at-risk genotypes, and RR1 and RR2 their associated relative risks, as compared with the low-risk genotype. For the purposes of estimation, odds ratios were equated to relative risks, since the disease prevalence is low. R e sult s In the initial screening, 12 SNPs spanning C3 and C5 (those listed in Table 2, excluding rs1047286) were genotyped in 446 case subjects with late-stage age-related macular degeneration and 267 control subjects (English group 1). No evidence of an association was found with variants in C5 (Table 2). In C3, the expressed SNP rs2230199 showed strong evidence of an association (P<0.001) and was genotyped in an additional 157 case subjects and 83 controls (English group 2). The enlarged sample also provided strong evidence of an association (P = 5.9Г—10–5) (Table 2). To test for replication of this finding, rs2230199 556 of m e dic i n e was genotyped by a different laboratory in 244 case subjects with late-stage age-related macular degeneration, 261 case subjects with age-related maculopathy, and 351 controls (Scottish group). Again, there was a highly significant association between the minor allele and age-related macular degeneration (P = 5.0Г—10–5) (Table 3). International HapMap Project18 data for the CEPH population showed that rs2230199 had an r2 value of 0.75 with rs2230203 but a low r2 value with other C3 SNPs in our marker panel and with other C3 SNPs in the HapMap data set. SNP rs2230203 did not show a significant association with agerelated macular degeneration in group 1 alone, but there was weak evidence of an association in groups 1 and 2 combined (Table 2). Because of the known association between the allotypes of rs2230199 and the expressed C3 SNP rs1047286, the English and Scottish subjects were genotyped for this marker (Tables 2 and 3). The minor allele frequency was significantly higher in case subjects than in controls in both groups, but the association was not as strong as for rs2230199. Stepwise logistic-regression analysis confirmed that rs2230199 is a significantly better predictor of risk for age-related macular degeneration. With this SNP in the model, adding rs1047286 made no contribution (P = 0.90). With rs1047286 in the model, adding rs2230199 produced a significant improvement in fit (P = 0.02). Odds ratios for age-related macular degeneration as a function of rs2230199 genotype are given in Table 4. Results for the English and Scottish groups were similar. In the combined data set, with the common CC genotype as the reference, the odds ratio was 1.7 for CG heterozygotes and 2.6 for GG homozygotes. The estimated population attributable risk for this variant was 22%. Subgroup analysis that was confined to case subjects with only choroidal neovascularization showed a highly significant association in both case–control groups. For case subjects with only geographic atrophy, the association was significant in the English group (P = 4.6Г—10–4) but not in the Scottish group, which had fewer subjects with geographic atrophy. The Scottish group included case subjects with age-related maculopathy, and in this subgroup the association fell just short of significance (Table 3). Data on other susceptibility loci for age-related macular degeneration were available for English group 1. Results for CFH Y402H have been pub- n engl j med 357;6  www.nejm.org  august 9, 2007 Pro496Pro Val542Val rs2230203 (6650782 bp, exon 13) rs2230204 (6649848 bp, exon 14) 94 (36) 109 (45) 68 (27) rs344550 (6622953 bp, intron 33) rs2277984 (6619511 bp, intron 36) 105 (41) rs344542 (6627517 bp, intron 27) rs2241393 (6625304 bp, intron 29) 97 (37) 126 (47) 235 (67) rs2287846 (6636557 bp, intron 22) Val802Ile Pro292Leu (HAV4-1 allotype) rs1047286 (6653262 bp, exon 9) 227 (65) 128 (50) 223 (64) n engl j med 357;6  www.nejm.org  august 9, 2007 82 (33) 132 (53) 100 (40) 126 (50) 106 (44) 122 (47) 119 (46) 121 (47) 113 (42) 99 (28) 106 (30) 109 (32) 108 (42) 10 (4) 40 (16) 13 (5) 60 (24) 28 (12) 45 (17) 35 (14) 42 (16) 27 (10) 16 (5) 17 (5) 14 (4) 20 (8) aa 0.20 0.42 0.25 0.48 0.33 0.41 0.36 0.39 0.31 0.19 0.20 0.20 0.29 MAF Aa 269 (63) 141 (33) 233 (59) 118 (28) 186 (44) 183 (42) 158 (36) 164 (38) 233 (52) 354 (59) 323 (54) 303 (51) 138 (33) 204 (47) 140 (35) 201 (47) 184 (43) 196 (45) 227 (52) 208 (48) 177 (40) 207 (34) 230 (38) 242 (41) 159 (36) 17 (4) 86 (20) 24 (6) 108 (25) 53 (13) 57 (13) 54 (12) 64 (15) 34 (8) 41 (7) 49 (8) 45 (8) 30 (7) aa Case Subjects number (percent) 248 (57) AA 0.20 0.44 0.24 0.49 0.34 0.36 0.38 0.38 0.28 0.24 0.27 0.28 0.25 MAF 0.98 0.62 0.53 0.89 0.73 0.06 0.53 0.74 0.13 1.00 0.31 0.47 0.80 0.92 0.17 0.34 0.87 0.31 0.03 2.3Г—10в€’3 4.0Г—10в€’4 0.007 0.23 2.8Г—10в€’4 0.12 5.9Г—10в€’5 Genotype P Value†Allele *Because of genotyping failures, data were not available for all subjects. Genotype frequencies are given as percentages of subjects genotyped. The location of single-nucleotide polyВ morphisms (SNPs) in C3 and C5 is specified by the position on a contig map of chromosomes 19 and 9, respectively, from the National Center for Biotechnology Information’s SNP Database, build 127. The numbering of the C3 amino acid sequence excludes the 22 residues of the signal peptide present in precursor C3 (pro-C3). Percentages may not total 100 because of rounding. “A” denotes common allele, “a” minor allele, and MAF minor allele frequency. †P values were calculated with the chi-square test and are for comparisons of allele and genotype frequencies between case subjects and controls. 160 (63) 79 (31) rs17611 (31090405 bp, exon 19) rs7026551 (31054338 bp, intron 31) 137 (55) rs7033790 (31109597 bp, intron 8) C5 Controls Aa number (percent) Arg80Gly (slow/fast allotype) AA rs2230199 (6658387 bp, exon 3) Amino Acid Data rs2250656 (6658534 bp, intron 2) C3 Gene and SNP ID (Location) Table 2. Genotyping Results for English Subjects.* Complement C3 Variant and Age-Related Macular Degener ation 557 3.4Г—10в€’3 7.3Г—10в€’4 0.29 18 (8) 0.12 2.2Г—10в€’3 0.06 0.27 5.2Г—10в€’4 0.24 13 (5) 94 (41) 116 (51) 0.20 13 (4) Age-related macular degeneration Pro292Leu (HAV4-1 allotype) rs1047286 Arg80Gly (slow/fast allotype) rs2230199 210 (64) 103 (32) 141 (56) 96 (38) 35 (7) 0.20 0.20 215 (65) 103 (31) All subjects 14 (4) 215 (65) 103 (31) Age-related maculopathy 14 (4) 117 (49) 100 (42) 0.20 215 (65) 103 (31) Age-related macular degeneration 14 (4) 258 (53) 196 (40) 5.0Г—10в€’5 22 (9) aa Aa number (percent) AA MAF aa number (percent) AA Aa 0.30 3.3Г—10в€’4 Genotype Allele MAF P Value†Case Subjects Controls Amino Acid Data C3 Gene SNP ID Table 3. Genotyping Results for Scottish Replication Group.* 558 *Because of genotyping failures, data were not available for all subjects. Genotype frequencies are given as percentages of subjects genotyped. The numbering of the C3 amino acid Вsequence excludes the 22 residues of the signal peptide present in precursor C3 (pro-C3). “A” denotes common allele, “a” minor allele, and MAF minor allele frequency. †P values were calculated with the chi-square test and are for comparisons of allele and genotype frequencies between case subjects and controls. n e w e ng l a n d j o u r na l The of m e dic i n e lished previously and are in agreement with other reports.7 Odds ratios and population attributable risks for LOC387715 (rs10490924) and CFB (rs641153) are given in Table 5. The results are similar to those of other studies, except that we found a lower odds ratio for rs10490924 homozygotes. When these variables were included in the stepwise logistic model, C3 rs2230199 remained significant, with an odds ratio of 1.4 for CG heterozygotes and 3.3 for GG homozygotes (with CC genotype as the reference), confirming that these susceptibility loci are independent risk factors. Dis cus sion Our study showed a strong association between the complement C3 S/F (Arg80Gly) polymorphism and age-related macular degeneration, with similar findings for geographic atrophy and choroidal neovascularization. The C3F allele frequency is approximately 20% in white populations but lower in other ethnic groups. For age-related maculopathy, the association fell just short of significance, raising the possibility that this polymorphism has less influence on the earlier stages of the disease. The complement system comprises more than 30 plasma and cell-surface proteins. It mediates the host defense against pathogens and the elimination of immune complexes and apoptotic cells; it also facilitates adaptive immune responses.22 C3 is the most abundant complement component, synthesized predominantly in the liver but to a lesser extent in other cells and tissues. Significant C3 messenger RNA is detectable in the neural retina, choroid, retinal pigment epithelium, and cultured retinal-pigment-epithelium cells.15 Cleavage of C3 into C3a and C3b is the central step in complement activation and can be initiated by the classic antibody-mediated pathway, the lectin pathway, or the alternative complement pathway.22 C3b attaches to pathogens or other target surfaces and binds factor B, which is then cleaved. The resulting C3bBb complex has C3 convertase activity, which amplifies the response by further cleavage of C3 and leads to the formation of C3b2Bb complexes with C5 convertase activity. This brings about cleavage of component C5 and recruitment by C5b of components C6 through C9 to form a large molecular pore on target membranes (the membrane attack complex), resulting in cell lysis.22 n engl j med 357;6  www.nejm.org  august 9, 2007 Complement C3 Variant and Age-Related Macular Degener ation Drusen contain C3 and its activation products, as well as C5, membrane attack complex, and CFH,6,15 supporting the hypothesis that local inflammation and activation of the complement cascade contribute to the pathogenesis of age-related macular degeneration. Further support for this hypothesis comes from conclusive evidence that variants in CFH influence susceptibility to age-related macular degeneration.3-9 CFH is a key regulator of the alternative complement pathway and prevents uncontrolled complement activation. Variants in factor B also apВ pear to influence susceptibility to age-related macular degeneration.10,11 In mice, activation of complement and formation of the membrane attack complex are essential for the development of laser-induced choroidal neovascularization. Indeed, the finding that choroidal neovascularization cannot be induced by laser coagulation in C3в€’/в€’ mice demonstrates the key role of C3 in this process.23 As a result of cleavage of C3 to form C3b, the molecule undergoes conformational changes that expose several binding sites, including the thioВ ester moiety, which is essential for C3b binding to target surfaces.24 Exposure of this activated acyl-imidazole intermediate requires a substantial relocation of the thioester-containing domain to a position adjacent to the first macroglobulin domain.24 Arg80 together with Arg72 and Lys82 forms a positively charged patch on the surface of this domain, which, in C3b, is brought into close proximity with the negatively charged carboxyl groups of several amino acids on the surface of the thioester-containing domain (Fig. 1). Substitution of an uncharged glycine for the positively charged Arg80 is predicted to weaken the interaction between these oppositely charged surfaces and could potentially influence thioester activity or other binding interactions of the thioВ ester-containing domain, including a probable C3b/C3d binding site with CFH.25 It follows that there could well be functional differences between the C3 S/F variants. Direct experimental evidence of functional differences in vitro between the C3 S/F allotypes is not conclusive. Arvilommi26 reported that erythrocytes coated with C3F showed greater rosetting with peripheral-blood mononuclear cells than those coated with C3S. Welch et al.27 studied uptake on sheep erythrocytes, hemolytic activity, conversion to inactive C3b, and capacity to solu- Table 4. Complement C3 rs2230199 Genotype (C3 S/F Allotype) and Odds Ratios for Age-Related Macular Degeneration.* Group Odds Ratio (95% CI) CG (C3 S/F Allotype) GG (C3 F/F Allotype) English subjects 1.6 (1.2–2.2) 2.4 (1.3–4.4) Scottish subjects 1.8 (1.2–2.6) 2.9 (1.4–5.9) Combined groups 1.7 (1.3–2.1) 2.6 (1.6–4.1) *Odds ratios are for the comparison with the CC genotype (C3 S/S allotype). Table 5. Odds Ratios for Age-Related Macular Degeneration and Population Attributable Risk for Variants at the Susceptibility Loci CFH, CFB, and LOC387715 in English Group 1.* Locus (Variant) Odds Ratio (95% CI) Population Attributable Risk Aa aa CFH (Y402H)7 3.1 (2.0–4.6) 6.3 (3.8–10.4) 63 CFB (rs641153) 0.5 (0.3–0.8) 0.2 (0.02–1.8) 77 LOC387715 (rs10490924) 2.4 (1.6–3.6) 2.4 (1.5–3.8) 43 % *Odds ratios are for the comparison with the AA genotype. “A” denotes common allele, and “a” minor allele. bilize preformed immune complexes. The only significant difference was that C3F had lower activity than C3S in a hemolytic assay using sensitized sheep erythrocytes as a result of a small difference in cell-surface binding. BartГіk and Walport28 found no differences between binding of C3S and C3F and the major complement receptor types 1, 2, and 3. On the other hand, there is compelling indirect evidence of a functional difference between C3S and C3F. A recent study has shown that the C3 S/F genotype is an important determinant of the long-term outcome of renal transplantation.29 In recipients who were C3S homozygotes, graft survival was substantially prolonged and renal function significantly better with C3 F/F and C3 F/S donor kidneys than with C3 S/S kidneys. Several associations of disease with C3F have been reported, including IgA nephropathy,30 systemic vasculitis,31 partial lipodystrophy, and membranoproliferative glomerulonephritis type II (MPGNII).32,33 The association with MPGNII is particularly relevant. This is a rare disease characterized by complement-containing dense deposits in the glomerular basement membrane of the n engl j med 357;6  www.nejm.org  august 9, 2007 559 The n e w e ng l a n d j o u r na l of m e dic i n e ated with serum C3 nephritic factor,34 an autoantibody directed against the C3bBb complex, but rare cases associated with mutations in CFH have been reported.35 A similar form of glomerulonephritis develops in CFH-deficient pigs36 and CFH knockout mice.37 The interface of the capillary tuft, the glomerular basement membrane, and the glomerular epithelial cells in the kidney is similar in structure to the interface involving choriocapillaris, Bruch’s membrane, and retinal pigment epithelium in the eye, and macular drusen similar to those in age-related macular degeneration develop in patients with MPGNII, but at a much younger age.38 These lesions are structurally and compositionally identical to those in patients with age-related macular degeneration and show immunoreactivity to complement C5 and C5b-9 complexes.39 Drusen have also been reported in patients with partial lipodystrophy.40 The association of MPGNII and partial lipodystrophy with C3F fits well with our current findings. In summary, our study shows a strong association between the C3F variant and age-related macular degeneration, and there is evidence of functional differences between the C3 S/F allotypes. It follows that C3F is likely to have a causal role in the disorder. The estimated population attributable risk in the white population is 22%. These findings add to our growing understanding of the genetics of age-related macular degeneration and provide conclusive evidence that the complement pathway has a key role in the pathogenesis of this common and debilitating condition. Figure 1. Structure of Complement C3b, Showing the Location of Arg80. Ribbon representation of the structure of complement C3b, as proposed by Janssen et al.,24 shows the interface region between the macroglobulin 1 domain (MG1) (light blue) and the thioester-containing domain (orange). The residues participating in the formation of the thioester bond are shown in yellow. Arg80 (red) is located in MG1, adjacent to two other positively charged amino acids, Arg72 and Lys82 (purple). These residues are approximately 4 Г… from the negatively charged amino acids Asp1007, Glu1008, Glu1010, and Glu1013 (dark blue) in the thioester-containing domain. The first three of these residues contribute to a probable C3b/C3d binding site with complement factor H.25 Arg80 may also have interactions with negatively charged residues (not shown) in the complement C1r/C1s–Uegf– Bmp1–containing domain, adjacent to the thioester-containing domain. kidney.34 The condition is caused by uncontrolled activation of the alternative complement pathway. In the majority of patients, the condition is associ- 560 Supported by grants from the Medical Research Council, United Kingdom (to Drs. Yates, Clayton, Bird, and Moore), the Chief Scientist Office, Scotland (to Dr. Dhillon), the Macular Vision Research Foundation (to Dr. Wright), and the Wellcome Trust and the Juvenile Diabetes Research Foundation (to Dr. Clayton). The Lothian Birth Cohort collection was supported by the Biotechnology and Biological Sciences Research Council. Dr. Deary is the recipient of a Royal Society–Wolfson Research Merit Award. Dr. Dhillon reports receiving consulting fees from Novartis and Pfizer. No other potential conflict of interest relevant to this article was reported. We thank members of the Scottish Macula Society Study Group (M. Gavin, F. Imrie, N. Lois, R. Murray, A. Purdie, A. Pyott, S. Roxburgh, C. Styles, M. Virdi, and W. Wykes) for their help in the recruitment of patients for our study; clinic staff and medical photographers at the participating clinics for their help; Tunde Peto and colleagues at the Reading Centre, Moorfields Eye Hospital, London, for grading the fundus photographs; the staff at Tepnel Life Sciences for performing the DNA extractions; Roger Williams for his helpful discussion about C3b protein structure; the International HapMap Consortium for the use of data; and all the patients and their families who participated in the study. n engl j med 357;6  www.nejm.org  august 9, 2007 Complement C3 Variant and Age-Related Macular Degener ation Appendix The following investigators are members of the Genetic Factors in Age-Related Macular Degeneration Study Group: S.S. Bhattacharya, P. Bishop, P. Black, Z. Butt, V. Chong, N.E. Day, C. Edelsten, A. Fitt, D.W. Flanagan, A. Glenn, S. Harding, C. Jakeman, C. Jones, R.J. Lamb, A. Lotery, V. Moffatt, C.M. Moorman, T. Peto, R.J. Pushpanathan, and T. Rimmer. References 1. de Jong PTMV. Age-related macular de- generation. N Engl J Med 2006;355:147485. 2. Haddad S, Chen CA, Santangelo SL, Seddon JM. The genetics of age-related macular degeneration: a review of progress to date. Surv Ophthalmol 2006;51:316-63. 3. Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science 2005;308:385-9. 4. Haines JL, Hauser MA, Schmidt S, et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 2005;308:419-21. 5. Edwards AO, Ritter R III, Abel KJ, Manning A, Panhuysen C, Farrer LA. Complement factor H polymorphism and age-related macular degeneration. Science 2005;308:421-4. 6. Hageman GS, Anderson DH, Johnson LV, et al. A common haplotype in the complement regulatory gene factor H (HF1/ CFH) predisposes individuals to age-related macular degeneration. Proc Natl Acad Sci U S A 2005;102:7227-32. 7. Sepp T, Khan JC, Thurlby DA, et al. Complement factor H variant Y402H is a major risk determinant for geographic atrophy and choroidal neovascularization in smokers and nonsmokers. Invest Ophthalmol Vis Sci 2006;47:536-40. 8. Li M, Atmaca-Sonmez P, Othman M, et al. CFH haplotypes without the Y402H coding variant show strong association with susceptibility to age-related macular degeneration. Nat Genet 2006;38:1049-54. 9. Hughes AE, Orr N, Esfandiary H, DiazTorres M, Goodship T, Chakravarthy U. A common CFH haplotype, with deletion of CFHR1 and CFHR3, is associated with lower risk of age-related macular degeneration. Nat Genet 2006;38:1173-7. [Erratum, Nat Genet 2007;39:567.] 10. Gold B, Merriam JE, Zernant J, et al. Variation in factor B (BF) and complement component 2 (C2) genes is associated with age-related macular degeneration. Nat Genet 2006;38:458-62. 11. Maller J, George S, Purcell S, et al. Common variation in three genes, including a noncoding variant in CFH, strongly influences risk of age-related macular degeneration. Nat Genet 2006;38:1055-9. 12. Jakobsdottir J, Conley YP, Weeks DE, Mah TS, Ferrell RE, Gorin MB. Susceptibility genes for age-related maculopathy on chromosome 10q26. Am J Hum Genet 2005;77:389-407. 13. Dewan A, Liu M, Hartman S, et al. HTRA1 promoter polymorphism in wet age-related macular degeneration. Science 2006;314:989-92. 14. Yang Z, Camp NJ, Sun H, et al. A vari- ant of the HTRA1 gene increases susceptibility to age-related macular degeneration. Science 2006;314:992-3. 15. Mullins RF, Russell SR, Anderson DH, Hageman GS. Drusen associated with aging and age-related macular degeneration contain proteins common to extracellular deposits associated with atherosclerosis, elastosis, amyloidosis, and dense deposit disease. FASEB J 2000;14:835-46. 16. Deary IJ, Whiteman MC, Starr JM, Whalley LJ, Fox HC. The impact of childhood intelligence on later life: following up the Scottish mental surveys of 1932 and 1947. J Pers Soc Psychol 2004;86:130-47. 17. Bird AC, Bressler NM, Bressler SB, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. Surv Ophthalmol 1995;39:367-74. 18. The International HapMap Consortium. The International HapMap Project. Nature 2003;426:789-96. 19. Azen EA, Smithies O. Genetic polymorphism of C’3(beta1C-globulin) in human serum. Science 1968;162:905-7. 20. Botto M, Fong KY, So AK, Koch C, Walport MJ. Molecular basis of polymorphisms of human complement component C3. J Exp Med 1990;172:1011-7. 21. Koch C, Behrendt N. A novel polymorphism of human complement component C3 detected by means of a monoclonal antibody. Immunogenetics 1986;23:322-5. 22. Walport MJ. Complement (first of two parts). N Engl J Med 2001;344:105866. 23. Bora PS, Hu Z, Tezel TH, et al. Immunotherapy for choroidal neovascularization in a laser-induced mouse model simulating exudative (wet) macular degeneration. Proc Natl Acad Sci U S A 2003;100:2679-84. 24. Janssen BJ, Christodoulidou A, McCarthy A, Lambris JD, Gros P. Structure of C3b reveals conformational changes that underlie complement activity. Nature 2006; 444:213-6. 25. Jokiranta TS, Jaakola VP, Lehtinen MJ, PГ¤repalo M, Meri S, Goldman A. Structure of complement factor H carboxyl-terminus reveals molecular basis of atypical haemolytic uremic syndrome. EMBO J 2006;25:1784-94. 26. Arvilommi H. Capacity of complement c3 phenotypes to bind on to mononuclear cells in man. Nature 1974;251:740-1. 27. Welch TR, Beischel L, Kleesattel A. Functional consequences of the genetic polymorphism of the third component of complement. J Pediatr 1990;116:S92-S97. 28. BartГіk I, Walport MJ. Comparison of the binding of C3S and C3F to complement receptors types 1, 2, and 3. J Immunol 1995;154:5367-75. 29. Brown KM, Kondeatis E, Vaughan RW, et al. Influence of donor C3 allotype on late renal-transplantation outcome. N Engl J Med 2006;354:2014-23. 30. Rambausek M, van den Wall Bake AW, Schumacher-Ach R, et al. Genetic polymorphism of C3 and Bf in IgA nephropathy. Nephrol Dial Transplant 1987;2: 208-11. 31. Finn JE, Zhang L, Agrawal S, Jayne DR, Oliveira DB, Mathieson PW. Molecular analysis of C3 allotypes in patients with systemic vasculitis. Nephrol Dial Transplant 1994;9:1564-7. 32. Finn JE, Mathieson PW. Molecular analysis of C3 allotypes in patients with nephritic factor. Clin Exp Immunol 1993; 91:410-4. 33. McLean RH, Winkelstein JA. Genetically determined variation in the complement system: relationship to disease. J Pediatr 1984;105:179-88. 34. Appel GB, Cook HT, Hageman G, et al. Membranoproliferative glomerulonephritis type II (dense deposit disease): an update. J Am Soc Nephrol 2005;16: 1392-403. 35. Abrera-Abeleda MA, Nishimura C, Smith JL, et al. Variations in the complement regulatory genes factor H (CFH) and factor H related 5 (CFHR5) are associated with membranoproliferative glomerulonephritis type II (dense deposit disease). J Med Genet 2006;43:582-9. 36. HГёgГҐsen K, Jansen JH, Mollnes TE, Hovdenes J, Harboe M. Hereditary porcine membranoproliferative glomerulonephritis type II is caused by factor H deficiency. J Clin Invest 1995;95:1054-61. 37. Pickering MC, Cook HT, Warren J, et al. Uncontrolled C3 activation causes membranoproliferative glomerulonephritis in mice deficient in complement factor H. Nat Genet 2002;31:424-8. 38. Colville D, Guymer R, Sinclair RA, Savige J. Visual impairment caused by retinal abnormalities in mesangiocapillary (membranoproliferative) glomerulonephritis type II (“dense deposit disease”). Am J Kidney Dis 2003;42:E2-E5. 39. Mullins RF, Aptsiauri N, Hageman GS. Structure and composition of drusen associated with glomerulonephritis: implications for the role of complement activation in drusen biogenesis. Eye 2001;15: 390-5. 40. Patel D, Page B. Ocular complications in acquired partial lipodystrophy. Postgrad Med J 2006;82:774. Copyright В© 2007 Massachusetts Medical Society. n engl j med 357;6  www.nejm.org  august 9, 2007 561 The n e w e ng l a n d j o u r na l of m e dic i n e original article NXY-059 for the Treatment of Acute Ischemic Stroke Ashfaq Shuaib, M.D., Kennedy R. Lees, M.D., Patrick Lyden, M.D., James Grotta, M.D., Antonio Davalos, M.D., Stephen M. Davis, M.D., Hans-Christoph Diener, M.D., Tim Ashwood, Ph.D., Warren W. Wasiewski, M.D., and Ugochi Emeribe, Ph.D., for the SAINT II Trial Investigators* A bs t r ac t Background From the Division of Neurology, University of Alberta, Edmonton, Canada (A.S.); the Acute Stroke Unit and Cerebrovascular Clinic, University Department of Medicine and Therapeutics, Gardiner Institute, Western Infirmary, Glasgow, United Kingdom (K.R.L.); the University of California San Diego Stroke Center, San Diego (P.L.); the Department of Neurology, University of Texas–Houston Medical School, Houston (J.G.); the Department of Neurosciences, Hospital Universitari Germans Trias i Pujol, Universitat AutГІnoma de Barcelona, Badalona, Spain (A.D.); the Department of Neurology, Royal Melbourne Hospital, University of Melbourne, ParkВ ville, Australia (S.M.D.); the Department of Neurology, University Duisburg–Essen, Essen, Germany (H.-C.D.); AstraZeneca R&D SГ¶dertГ¤lje, Medical Neuroscience, SГ¶dertГ¤lje, Sweden (T.A.); and AstraВ Zeneca, Wilmington, DE (W.W.W., U.E.). Address reprint requests to Dr. Lees at the Acute Stroke Unit and Cerebrovascular Clinic, University Department of Medicine and Therapeutics, Gardiner Institute, Western Infirmary, 44 Church St., Glasgow G11 6NT, United Kingdom, or at k.r.lees@clinmed.gla.ac.uk. *The investigators participating in the Stroke–Acute Ischemic NXY Treatment II (SAINT II) trial are listed in the Appendix. N Engl J Med 2007;357:562-71. The free-radical–trapping agent NXY-059 showed promise as a neuroprotectant in the Stroke–Acute Ischemic NXY Treatment I (SAINT I) trial, reducing disability when given to patients who had acute ischemic stroke. We sought confirmation of efficacy in a second, larger trial. Methods We enrolled 3306 patients with acute ischemic stroke in a randomized, doubleblind trial to receive a 72-hour infusion of intravenous NXY-059 or placebo within 6 hours after the onset of stroke symptoms. Our primary end point was the distribution of disability scores on the modified Rankin scale at 90 days. We examined scores on neurologic and activities-of-daily-living scales as secondary end points. We also tested the hypothesis that NXY-059 would reduce alteplase-related intracranial hemorrhages. Results The efficacy analysis was based on 3195 patients. Prognostic factors were well balanced between the treatment groups. Mortality was equal in the two groups, and adverse-event rates were similar. The distribution of scores on the modified Rankin scale did not differ between the group treated with NXY-059 (1588 patients) and the placebo group (1607 patients; P = 0.33 by the Cochran–Mantel–Haenszel test; odds ratio for limiting disability, 0.94; 95% confidence interval [CI], 0.83 to 1.06). Analysis of categorized scores on the modified Rankin scale confirmed the lack of benefit: the odds ratio for trichotomization into modified Rankin scale scores of 0 to 1 versus 2 to 3 versus 4 to 6 was 0.92 (95% CI, 0.80 to 1.06). There was no evidence of efficacy for any of the secondary end points. Among patients treated with alteplase, there was no difference between the NXY-059 group and the placebo group in the frequency of symptomatic or asymptomatic hemorrhage. Copyright В© 2007 Massachusetts Medical Society. Conclusions NXY-059 is ineffective for the treatment of acute ischemic stroke within 6 hours after the onset of symptoms. (ClinicalTrials.gov number, NCT00061022.) 562 n engl j med 357;6  www.nejm.org  august 9, 2007 NXY-059 for Acute Ischemic Stroke C urrently, thrombolysis with alteВ plase (tissue plasminogen activator [rt-PA]) is the only widely approved treatment for acute stroke, and it is underused. There is an urgent need for new therapies that are safer and can be offered to a higher percentage of patients. Cerebral tissue can be protected in animal models by a variety of agents that attenuate neuronal injury after ischemia,1 but none of these putative neuroprotectants have been confirmed as an effective therapy in clinical trials. NXY-059, a free-radical–trapping agent, has been extensively tested in animal models of focal ischemic stroke and has been shown to improve functional recovery and reduce the size of the cerebral infarction.2 A large study reported recently showed that NXY059 was significantly better than placebo in improving the outcome in patients with ischemic stroke treated within 6 hours after the onset of symptoms.3 Further support for the suggestion that NXY-059 is a true biologic signal came from post hoc analysis of the data, which also revealed that treatment with NXY-059 significantly reduced the incidence of intracranial hemorrhage among patients in whom alteplase was also used.3 We sought to confirm the results of the Stroke–Acute Ischemic NXY Treatment I (SAINT I) trial with a larger trial, SAINT II. Me thods Study design This randomized, double-blind, placebo-controlled study enrolled 3306 patients from May 2003 through June 2006. The study involved 362 centers from 31 countries and was approved by local or national institutional review boards as appropriate. Patients were assigned to treatment only after they had given informed consent or, for patients who were unable to do so, after consent had been obtained from an acceptable surrogate. The study was part of the SAINT program, which consists of two large, independent, doubleblind studies. Its design and conduct were developed by a steering committee of stroke experts from Europe, North America, and Australia. The steering committee had complete access to all data and was responsible for writing the manuscript. An independent data and safety monitoring committee was responsible for safety reviews and futility analysis. The sponsor, AstraZeneca, was responsible for operational aspects of the trial, including collecting and storing the data, and performing analyses according to the approved plan. The academic authors vouch for the completeness and veracity of the data and analyses. We originally planned to enroll 1700 patients in SAINT II, but on the basis of the results of SAINT I,3 we planned to increase the power of the trial by enlarging the study population to 3200 paВ tients without unblinding of any SAINT II data.4 Patients Patients were eligible for enrollment if they were 18 years of age or older and had a clinical diagnosis of an acute ischemic stroke with an onset within the previous 6 hours. They had to score at least six points on the National Institutes of Health Stroke Scale (NIHSS),5 with at least two points for limb weakness. All patients received appropriate routine stroke care according to local treatment practice, including alteplase for eligible patients presenting within 3 hours after the onset of the stroke. For patients receiving alteplase, treatment with the study drug had to be started within 30 minutes after completion of the alteplase infusion. Study intervention Patients were randomly assigned by a computergenerated coding system to receive an intravenous infusion of either NXY-059 or placebo. The treating centers were required to maintain an average time of no more than 4 hours to the start of infusion of the study drug. Randomization was stratified according to country, NIHSS score at baseline, side of the infarction, and intention to treat with alteplase. AstraZeneca supplied the study drug as a concentrate to be diluted to 15 mg per milliliter in 500 ml of 0.9% saline solution. The initial infusion rate was 2270 mg per hour, and the rate was reduced after an hour to 480 to 960 mg (32 to 64 ml) per hour for a further 71 hours, with the aim of maintaining a target serum concentration of 260 Ојmol of unbound study drug per liter. The infusion rate was guided by the estimated rate of creatinine clearance, based on the serum creatinine concentration.6 The infusion rate was adjusted to 32 ml per hour for clearance rates of 30 to 50 ml per minute, 44 ml per hour for clearance rates of 51 to 80 ml per minute, and 64 ml per hour for clearance rates greater than 80 ml per minute. For patients with clearance rates of less than 30 ml per minute, treatment was withdrawn. n engl j med 357;6  www.nejm.org  august 9, 2007 563 The n e w e ng l a n d j o u r na l Clinical Assessment Patients were assessed at various times throughout the study, including at the time of enrollment, 24 and 72 hours after the start of infusion of the study drug, and on days 7, 30, and 90. Initial assessments included a physical examination, neuroВ imaging, and an NIHSS assessment to determine the severity of the stroke. The examiners were trained and certified in the use of the NIHSS examination (scores range from 0 to 42, with a higher score indicating greater stroke severity).5 Assessments after completion of infusion of the study drug were primarily functional or neuroВ logic, including the score on the modified Rankin scale7 (assessed on days 7, 30, and 90), the NIHSS (days 7 and 90), and the Barthel index8 (days 7, 30, and 90). The modified Rankin scale is a global disability scale with a range from 0, indicating no residual symptoms, to 5, for patients who are bedridden and require constant care. In this study, patients who died were assigned a score of 5 on the modified Rankin scale. The investigators were trained, tested, and certified in the use of the modified Rankin scale according to a method involving the use of a DVD developed specifically for this trial.9 The NIHSS quantifies the level of neurologic deficit, with higher scores at day 90 predictive of dependence. The Barthel index measures activities of daily living; scores range from 0 to 100, with 0 indicating complete dependence and 100 indicating independence. of m e dic i n e Figure 1 (facing page). Enrollment, Group Assignment, and Follow-up. After randomization, 24 patients received the wrong treatment kit. Fourteen patients assigned to placebo received at least some NXY-059; these patients were considered in the efficacy analysis to have been treated with placebo and were considered in the safety analysis to have been treated with NXY-059. Ten patients Вassigned to NXY-059 were treated only with placebo; these patients were considered in the efficacy analysis to have been treated with NXY-059 and were considered in the safety analysis to have been treated with placebo. The efficacy analysis included all patients who underwent randomization and received any investigational treatment and for whom stratification data and any post-treatment assessment data were available. The last observation was carried forward for survivors who were unable to undergo assessment with the modified Rankin scale at 90 days. Patients who died were assigned a score of 5 on the scale (worst outcome) and were considered to have a valid assessment; 3126 patients (97.8%) had a valid 90-day assessment, and 69 (2.2%) had an earlier observation carried forward. The per protocol population (2858 patients, 88.2% of all treated patients) consisted of patients for whom there were no major protocol violations and who received at least 75% of the target dose for their rate of creatinine clearance. Patients in whom the study drug was stopped because of progressive stroke or death were retained in the per protocol population. rhage was defined as the presence of any blood on imaging after alteplase treatment in the absence of such worsening of the NIHSS score.3 Patients meeting the criterion for progressive stroke (an increase of at least four points on the Safety Assessments NIHSS score) or new stroke in the first week also Vital signs were recorded at enrollment and at underwent repeated imaging studies. Follow-up specified times throughout the infusion and dur- scans were read centrally by readers who were ing the follow-up period. Routine laboratory data unaware of treatment assignments. were obtained at the time of enrollment and at 24 hours, 72 hours, and 7 days. Electrocardiograms Statistical Analysis were obtained at enrollment and at 24 hours, 72 The analyses were prespecified. For the efficacy hours, and (if the findings at 72 hours were analysis, we included all patients with baseline Вabnormal) 7 days. Laboratory and electrocardio- data who had commenced any treatment and had graphic results were analyzed centrally. To deter- undergone any post-treatment assessment. The mine whether NXY-059 had any effect on hemor- patients were analyzed according to the treatment rhagic transformation (intracerebral hemorrhage) assignment for efficacy outcomes and according after treatment with alteplase, brain imaging was to the treatment actually received for safety outrepeated after 72 hours in patients receiving con- comes. The primary outcome measure was the comitant alteplase. On the basis of the results of score on the modified Rankin scale at 90 days or SAINT I, we defined symptomatic intracerebral the last rating, analyzed across the whole distrihemorrhage as a worsening in the NIHSS score bution of scores with the use of the Cochran– by four or more points within 36 hours plus the Mantel–Haenszel test, with adjustment for stratipresence of any blood on imaging after alteplase fication variables (NIHSS score, side of the infarct, treatment; asymptomatic intracerebral hemor- and use or nonuse of alteplase) and with the use 564 n engl j med 357;6  www.nejm.org  august 9, 2007 NXY-059 for Acute Ischemic Stroke 3306 Patients underwent randomization 1660 Were assigned to placebo 1646 Were assigned to NXY-059 65 Did not start treatment and were excluded from analysis 1635 Started treatment 1606 Started treatment 14 Who were assigned to placebo and 10 Who were assigned to NXY-059 crossed over to the alternative treatment group 1631 Received only placebo and were included in the safety population 1610 Received some NXY-059 and were included in the safety population 45 Withdrew or were lost to follow-up before first assessment 1 Was not included in efficacy analysis because of incomplete stratification data 1313 Underwent modified Rankin scale assessment at day 90 27 Withdrew or were lost to follow-up by day 90, with last observation carried forward 267 Died, assigned score of 5 on the modified Rankin scale 1279 Underwent modified Rankin scale assessment at day 90 42 Withdrew or were lost to follow-up by day 90, with last observation carried forward 267 Died, assigned score of 5 on the modified Rankin scale 1607 Were included in the efficacy analysis 1588 Were included in the efficacy analysis 337 Received <75% infusion or had protocol exclusion 1441 Were included in the per protocol analysis 1417 Were included in the per protocol analysis of modified ridit scores10 (i.e., the midrank score linked to the van Elteren test that allowed us to Г· [the number of observations + 1]), to account analyze the modified Rankin scale as an ordinal AUTHOR: Shuaib (Lees) ICM for ordered categories. The generalized Cochran– rather thanRETAKE a binary1st outcome, without assuming 2nd REG F FIGURE: 1 of 3 Mantel–Haenszel test is a nonparametric method proportional odds.113rdDichotomized and trichotoCASE Revised Line 4-C SIZE H/T H/T 33p9 Enon Combo n engl j med 357;6  www.nejm.org  august 9, 2007 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. EMail ARTIST: ts JOB: 35606 ISSUE: 08-09-07 565 The n e w e ng l a n d j o u r na l mized scores on the modified Rankin scale were also analyzed. The sample size of 3200 patients was chosen to provide at least 80% power to detect a common odds ratio of 1.2 (across all cutoff points of the modified Rankin scale), the result that was seen in the SAINT I study.3 Additional measurements of the modified Rankin scale were completed at 7 and 30 days. Neurologic function was assessed on the basis of the total NIHSS score, the first secondary end point, at 90 days or at the time of the last rating, and it was also analyzed by means of the Cochran–Mantel–Haenszel test with a modВ ified ridit score and adjustment for the baseline NIHSS score, side of the infarct, and use or nonuse of alteplase.10,11 We ordered the analysis of efficacy outcomes hierarchically, avoiding the need for further adjustment for multiplicity, because formal statistical testing was performed only if the preceding Table 1. Baseline Characteristics of the Patients.* Characteristic Mean age — yr Male sex — no. (%) Placebo (N = 1631) 69.0 NXY-059 (N = 1610) 68.8 870 (53.3) 898 (55.8) Mean time from onset of stroke to treatment — hr:min 3:49 3:46 Mean NIHSS score 13.0 13.0 Treatment or intention to treat with alteplase — no. (%) 716 (43.9) 710 (44.1) Mean time from onset of stroke to administration of alteplase — hr:min 2:24 2:22 Mean age — yr 68.6 67.7 Mean NIHSS score at trial entry 13.8 14.1 1246 (76.4) 1243 (77.2) 356 (21.8) 357 (22.2) Transient ischemic attack 161 (9.9) 135 (8.4) Ischemic heart disease 536 (32.9) 531 (33.0) Atrial fibrillation 499 (30.6) 438 (27.2) Diabetes mellitus 406 (24.9) 386 (24.0) Use of antiplatelet drugs 566 (34.7) 590 (36.6) Cardioembolic stroke†775 (47.6) 738 (46.1) History — no. (%) Hypertension Stroke *Scores on the NIHSS (National Institutes of Health Stroke Scale) range from 0, indicating normal functioning, to 42, indicating most severe impairment. †Percentages are based on 1627 patients in the placebo group and 1600 in the NXY-059 group. 566 of m e dic i n e end point was significant. The primary end point, the score on the modified Rankin scale, was the first outcome, and a positive trial would have been declared if this end point had been significant, irrespective of end points lower in the hierarchy. Safety end points included death, serious and nonserious adverse events, laboratory measurements, vital signs, and neuroimaging data. The incidence of intracranial hemorrhage in patients who were treated concomitantly with alteplase was prospectively analyzed with the chi-square test. Descriptive statistics (number and frequency) were used to summarize all types of intracranial hemorrhage for each treatment group. R e sult s Baseline characteristics Of the 3306 patients randomly assigned to treatment, 3241 were treated with NXY-059 or placebo (Fig. 1). In 65 patients, the infusion was not started, most commonly because of delayed recognition that the patient did not meet the eligibility criteria (20 patients assigned to NXY-059 and 19 assigned to placebo). The investigators became aware of the study-drug assignment in five cases. End-of-study assessment of drug infusion was completed in 3074 patients (1542 [95.8%] of those receiving NXY-059 and 1532 [93.9%] of those receiving placebo), and 2593 patients (80.0%) completed the 90-day follow-up assessment. Among the 3241 patients treated, modified-Rankin-scale outcome data were unavailable for 46 (23 assigned to NXY-059 and 23 assigned to placebo). The baseline characteristics of the patients are shown in Table 1. The mean time from the onset of symptoms to the start of infusion of the study drug was 3 hours 48 minutes. A total of 1426 patients (44.0%) received treatment with alteplase. According to extrapolation from measured concentrations, in 96.6% of NXY-059–treated patients, a target plasma unbound concentration of 150 Ојmol per liter was reached, which is well above the levels that have been shown to be neuroprotective in animal models of stroke. Clinical Outcomes The distribution of scores on the modified Rankin scale at 90 days was similar in the two groups (P = 0.33 by the Cochran–Mantel–Haenszel test; number of patients, 3195; odds ratio for a favor- n engl j med 357;6  www.nejm.org  august 9, 2007 NXY-059 for Acute Ischemic Stroke able outcome, 0.94; 95% confidence interval [CI], 0.83 to 1.06) (Fig. 2). We evaluated all possible dichotomizations of the scale as well as the trichotomization into categories 0 to 1, 2 to 3, and 4 to 5, as has been tested elsewhere.3 There were no significant differences between the two groups in any of the cutoff points: the P value for the trichotomization was 0.23 (odds ratio, 0.92; 95% CI, 0.80 to 1.06). Analysis of the group of patients who received at least 75% of the infusion and who were in full compliance with the protocol also did not show a significant difference between the two groups (P = 0.25 by the Cochran– Mantel–Haenszel test; odds ratio, 0.93; 95% CI, 0.81 to 1.06). There was no improvement in disability among survivors in the NXY-059 group at 7, 30, or 90 days, as measured by the Cochran– Mantel–Haenszel test (day 90, P = 0.53; odds ratio, 0.96; 95% CI, 0.83 to 1.10). NXY-059 had no effect on any of the prespecified secondary end points. The total NIHSS score at the last rating in the NXY-059 group was not significantly different from that in the placebo group (P = 0.73 by the Cochran–Mantel–HaenВ szel test; Mann–Whitney U statistic, 0.50; 95% CI, 0.48 to 0.52). In addition, there was no significant difference between the groups in the percentage of patients who had a complete recovery, as measured by an NIHSS score of 0 versus 1 to 42 (16.3% in the NXY-059 group and 16.6% in the placebo group), or a nearly complete recovery, as measured by an NIHSS score of 0 to 1 versus 2 to 42 (27.6% in both groups). Finally, there was no significant difference between the groups in the percentage of patients with a Barthel index score of 95 or more (40.9% in the NXY-059 group and 42.3% in the placebo group). Score 0 1 Placebo 10.3 18.4 NXY-059 9.8 17.6 2 3 14.7 15.0 14.0 14.7 5 or Death 4 17.4 24.2 17.8 26.1 Proportion of Patients in the Efficacy Population (%) Figure 2. Primary Outcome at 90 Days According to 1st AUTHOR: Shuaib (Lees) the ICM Score on the Modified Rankin Scale. RETAKE REG F CASE EMail Enon 2nd 3rd FIGURE: 2 of 3 There were no significant interactions between the treatment effect of NXY-059 and the time from the onset of symptoms to treatment (4 hours or less vs. more than 4 hours), presence of diabetes or hypertension, severity of stroke, or use of alteВ plase (Fig. 3). Safety Analysis There were 534 deaths, 267 in each treatment group (16.5% of patients). The mean (В±SE) time from randomization to death was 24.3В±1.4 days in the NXY-059 group and 21.9В±1.4 days in the placebo group (P = 0.98 by the log-rank test). Few deaths were reported during the drug infusion: 18 in the NXY-059 group (1.1%) and 18 in the placebo group (1.1%). The most common causes of death were neurologic damage from the initial stroke (in 83 patients in the NXY-059 group [31.1%] and 107 in the placebo group [40.1%]) and bronchopneumonia (41 in the NXY-059 group [15.4%] and 34 in the placebo group [12.7%]). Adverse events were reported in 84.2% of patients in the NXY-059 group and 84.5% of patients in Variable Odds Ratio (95% CI) ≤4 hr >4 hr 0.91 (0.78–1.06) 0.98 (0.79–1.22) Use of alteplase No use of alteplase 0.90 (0.74–1.08) 0.97 (0.82–1.15) NIHSS 6–9 NIHSS 10–14 NIHSS 15–19 NIHSS ≥20 0.85 (0.69–1.05) 0.92 (0.74–1.13) 1.14 (0.83–1.52) 1.00 (0.71–1.41) 0.5 1.0 Placebo Better 2.0 NXY-059 Better Figure 3. Treatment Interactions with Important Covariates. There was no significant interaction with any stratification variable or preRETAKE 1st AUTHOR: Shuaib (Lees) ICM specified covariate. The primary outcome measure was the score on the 3 of 3or the last rating, as analyzed2nd REGscale F FIGURE: modified Rankin at 90 days with the 3rd CASE Cochran–Mantel–Haenszel test with a modified ridit score, Revised adjusted for Line 4-C EMail baseline stratification variables. The Cochran–Mantel–Haenszel test conSIZE ARTIST: ts H/T scale, H/Twith deaths 22p3 assigned a siders the full Enon range of the modified Rankin Combo modified Rankin score of 5. Odds ratios were estimated by logistic regresAUTHOR, PLEASE NOTE: sion, adjusted forFigure baseline stratification variables, and are shown with their has been redrawn and type has been reset. estimated 95% confidence intervals. Interactions Please check carefully. between covariates and treatment effect were analyzed with the Cochran–Mantel–Haenszel test: P = 0.82 for JOB: time 35706 to treatment, P = 0.61 for use of alteplase, and P = 0.70 ISSUE: 08-09-07 for severity of stroke according to the National Institutes of Health Stroke Scale (NIHSS) category. Since none of these were significant, the individual odds ratios and their 95% confidence intervals are provided only for illustration. The size of the squares corresponds to the size of each subgroup. Revised ARTIST: ts Line 4-C SIZE H/T H/T 22p3 Combo n engl j med 357;6  www.nejm.org  august 9, 2007 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. JOB: 35706 ISSUE: 08-09-07 567 n e w e ng l a n d j o u r na l The the placebo group. Serious adverse events were reported in 39.6% of patients in the NXY-059 group and 40.2% of patients in the placebo group (Table 2). The percentage of patients who discontinued medication was 4.5% in the NXY-059 group and 6.3% in the placebo group. The only adverse event that occurred significantly more frequently in the NXY-059 group than in the placebo group was hypokalemia. Hypokalemia occurred in 12.1% of NXY-059–treated and 9.2% of placebo-treated patients at any stage and in 9.1% and 6.3% of patients, respectively, during the infusion but was not associated with any cardiac or Table 2. Safety Outcomes Recorded during 90 Days of Follow-up.* Variable Placebo (N = 1631) NXY-059 (N = 1610) no. (%) Serious adverse events Stroke in evolution 157 (9.6) 150 (9.3) Ischemic stroke 62 (3.8) 55 (3.4) Pneumonia 37 (2.3) 39 (2.4) Hemorrhagic transformation stroke 28 (1.7) 30 (1.9) Aspiration pneumonia 20 (1.2) 26 (1.6) Brain edema 28 (1.7) 24 (1.5) Cerebral hemorrhage 25 (1.5) 23 (1.4) Sepsis 9 (0.6) 22 (1.4) 25 (1.5) 18 (1.1) 7 (0.4) 16 (1.0) Pyrexia 268 (16.4) 289 (17.9) Headache 227 (13.9) 256 (15.9) Hypokalemia 150 (9.2) 195 (12.1) Constipation 151 (9.3) 170 (10.6) Urinary tract infection 161 (9.9) 164 (10.2) Stroke in evolution 164 (10.1) 152 (9.4) Atrial fibrillation 103 (6.3) 111 (6.9) Nausea 113 (6.9) 111 (6.9) Pneumonia 90 (5.5) 103 (6.4) Insomnia 79 (4.8) 101 (6.3) Myocardial infarction Atrial fibrillation Adverse events *The events included are the 10 most common serious adverse events and the 10 most common adverse events in the NXY-059 group (adverse events include those that were also coded as serious). In the analysis of safety, patients were considered as treated and not as randomly assigned to treatment. Because of the large number of potential adverse events that could be examined (>100), formal statistical testing was not conducted; as a guide, a difference of 1.5% or more between groups will occur with a probability of approximately 0.05 before adjustment for multiplicity. 568 of m e dic i n e other complications. Hypokalemia resolved within 7 days. In our prespecified analysis of patients treated with alteplase, there were no significant differences between the NXY-059 group and the placebo group in the percentage of patients with symptomatic cerebral hemorrhage (4.6% and 5.3%, respectively; P = 0.57), asymptomatic cerebral hemВ orrhage (17.9% and 16.1%, post hoc analysis), or overall cerebral hemorrhage (22.5% vs. 21.4%, P = 0.60). Dis cus sion This second trial of NXY-059 included a generous sample of patients with acute ischemic stroke. Although the trial was adequately powered to detect a clinically useful difference in the primary end point, the modified Rankin score, we failed to confirm the efficacy of NXY-059. SAINT I showed promising results, with reducВ tion of global disability.3 The effect on disability was moderate but was thought to be consistent with a neuroprotective action. Although there were no significant effects on the prespecified secondary end points, post hoc analyses showed supportive trends for other end points.4 Moreover, patients treated with alteplase and NXY-059 had fewer cerebral hemorrhages.3 We had refined the SAINT II protocol after the successful SAINT I trial; changes included an increase in the sample size from 1700 to 3200 patients, a revised approach to analysis of the NIHSS score, and a proВ spective analysis of intracerebral hemorrhage. However, none of the benefits demonstrated in SAINT I were confirmed in the SAINT II study. With the exception of mild, asymptomatic hypokalemia, the numbers and types of adverse events and serious adverse events, including neurologic events, were similar in the two groups. Faced with conflicting results from the two pivotal trials of NXY-059, we must examine possible explanations. These trials followed nearly identical protocols, with minimal differences in statistical analysis. With the exception of a higher frequency of alteplase use in SAINT II (44% vs. 29%), the baseline characteristics and demographВ ic features of the study populations were similar. In both trials, the average time to treatment was less than 4 hours and target plasma drug concentrations were achieved and maintained in more than 95% of patients. n engl j med 357;6  www.nejm.org  august 9, 2007 NXY-059 for Acute Ischemic Stroke We first considered whether the conflicting results of the two trials might be related to the higher rate of alteplase use in SAINT II. However, we found no evidence of an interaction between alteplase use and the effect of NXY-059 in either trial. Although we cannot completely rule out a ceiling effect in SAINT II resulting from an already maximal improvement due to alteplase use, monotherapy with NXY-059 was also ineffective. From these data, we cannot draw any conclusion about the arguments for or against includВ ing patients treated with alteplase in future trials of putative neuroprotectants. We did not use perfusion imaging as a selection criterion for this trial. It is conceivable that any treatment effect might have been diluted by the inclusion of patients with established infarction or without a perfusion deficit at the time of randomization. However, because of the large sample size and the expectedly high proportion of patients in whom penumbra would still have been present within 4 hours after the onset of stroke, we do not think that the use of imaging would have transformed the outcome of this trial. In addition, we did not collect data on the subtype of stroke, but we find no evidence from our data on the severity of stroke that the treatment effect was likely to have been influenced by the subtype of stroke. We do not consider that our statistical approach was responsible for the false positive result in SAINT I. In both trials, the same method was used to analyze the results for the primary end point — namely, comparison of the distribution of disability scores rather than simple dichotomy. Our analysis takes into account any potential harm by requiring that any deleterious effect at one end of the scale be more than balanced by a benefit at other levels if significance is to be achieved. We consider that the disparity between the two studies occurred by chance, possibly because of the inclusion of patients with a latent poorer prognosis in the placebo group in SAINT I. However, there was no notable imbalance between the treatment groups with respect to any single measured variable or combination of variables. The likelihood that our prior trial was positive simply because of the play of chance underscores the need for replication by a second pivotal trial. The observed reduction in the rate of hemorrhagic transformation associated with NXY-059 after thrombolysis in SAINT I was biologically plausible, given the role of free-radical–mediated disruption of the blood–brain barrier. Vasculoprotection with NXY-059 during thrombolysis was consistent with the putative mechanism of the drug.12,13 The absence of this finding in SAINT II provides further confirmation of the discrepancy between the trials and suggests that this was also a chance finding or the result of differences in the study populations. Stroke Therapy Academic Industry Roundtable (STAIR) criteria were designed to help in the development of drug therapy for acute stroke.14‑16 Even though it met all these criteria, the SAINT II study showed no significant effect in patients with acute ischemic stroke. It is possible that the animal models of acute focal infarction are not relevant to the patient population; they certainly are insufficient to guarantee a positive clinicaltrial result. The molecular heterogeneity and pharmacodynamics in elderly patients may differ from those in the healthy and relatively young animals used for preclinical studies. The clear failure to demonstrate a benefit of NXY-059 in the SAINT II study suggests that we need to reevaluate the strategies that have been used in the development of drugs for neuroprotection. More emphasis on phase 2 studies in patients, involving a surrogate outcome measure that is more sensitive to treatment effects even if it is not acceptable for drug-registration purposes, may be necessary to supplement the preclinical data.17 In summary, SAINT II provides clear evidence that the promise offered by the preclinical data and the positive findings of SAINT I has been a false dawn. The most reasonable interpretation is that NXY-059 is safe but ineffective for the treatment of acute ischemic stroke. Drs. Lees, Grotta, and Davis report receiving fees and expenses from AstraZeneca for steering-committee work and lectures. Dr. Davis reports receiving consulting or speaking fees from Novo Nordisk, Pfizer, Sanofi-Aventis, Bristol-Myers Squibb, Boehringer Ingelheim, Paion, and Servier; Dr. Davalos, consulting or speaking fees AstraZeneca, Boehringer Ingelheim, Pfizer, Merck Sharpe & Dohme, Sanofi-Synthelabo, Bristol-Myers Squibb, Bayer, Paion, Forest Pharmaceuticals, Daiichi Asubio, Eli Lilly, Fujisawa, Novo Nordisk, and Ferrer International; Dr. Diener, consulting or speaking fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, BASF, Abbott, Novartis, Parke-Davis, Merck Sharpe & Dohme, Servier, Sanofi-Synthelabo, Bayer, Fresenius, and Janssen-Cilag; Dr. Lyden, consulting or speaking fees from AstraZeneca, Bayer, Mitsubishi, Pfizer, Lilly, and Merck and research contracts with AstraZeneca and Bayer; Dr. Grotta, research support from AstraZeneca, NovoNordisk, and Boehringer Ingleheim; and Dr. Shuaib, consulting or n engl j med 357;6  www.nejm.org  august 9, 2007 569 The n e w e ng l a n d j o u r na l speaking fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Pfizer, Roche, Merck, and Sanofi-Synthelabo. Drs. Ashwood, WasiewВski, and Emeribe report being employees of AstraZeneca and holding stock in AstraZeneca. The SAINT trials were sponsored by AstraZeneca. NXY-059 is subject to a partnership agreement between AstraZeneca and Renovis; Renovis had no influence on the conduct, analysis, or interpretation of the study but was given an opportunity to review and comment on of m e dic i n e the manuscript. No other potential conflict of interest relevant to this article was reported. We thank the patients and their relatives; the clinical and research teams of the stroke units; the AstraZeneca coordinating and monitoring staff who participated in this trial; Dr. Tomas Odergren for his substantial contributions to the development of NXY-059 throughout AstraZeneca’s program; and the scientific, data-management, and statistical teams. APPENDIX The following investigators participated in the SAINT II trial: Steering committee — K.R. Lees, Glasgow, United Kingdom (chair); A. Shuaib (principal investigator), Edmonton, AB, Canada; T. Ashwood, SГ¶dertГ¤lje, Sweden (sponsor representative); A. Davalos, Barcelona; S. Davis, Melbourne, Australia; H.C. Diener, Essen, Germany; J. Grotta, Houston; P. Lyden, San Diego, CA; W. Wasiewski, Wilmington, DE (sponsor representative). Data and safety monitoring board — S. Pocock, London (chair); H. Adams, Iowa City, IA; P. Bath, Nottingham, United Kingdom; D. Oakes, Rochester, NY; N.G. Wahlgren, Stockholm. Study team leader — C. Baker, Wilmington, DE. Study team physicians — W.W. Wasiewski, Wilmington, DE; L. Rodichok, Wilmington, DE; H.G. Hardemark, SГ¶dertГ¤lje, Sweden. Study team statisticians — V. Alderfer, Wilmington, DE; U. Emeribe, Wilmington, DE. Contract research organizations — PPD Development, Covance Central Laboratory Services, Perceptive Informatics, Parexel International, eResearch Technology, Fisher Clinical Services, TEVA Pharmaceutical Industries. Medical science director — L. O’Dowd. Clinical centers: Argentina — R. Rey, S. Ameriso, E. Reich, F. Buonanotte, R.R. Escalante, M.M. Esnaola y Rojas, E. Gatto; Austria — M. Brainin, W. Grisold, F. Aichner, G. Ladurner, F. Gruber; Australia — S. Davis, C. Levi, C. Bladin, G. Donnan, J. Sturm, D. Schultz, C. Anderson, A. Barber; Belgium — G. Vanhooren, P. De Deyn, V. Thijs; Bulgaria — P. Stamenova, D. Baldaranov, D. Minchev, A. Tunev, V. Platikanov, T. Notcheva; Brazil — A. Massaro, E. Evaristo, A. Gomes Neto, L. Barea, M.A. Friedrich, S.C. Martina, J. Fernandes; Canada — A. Shuaib, D. Selchen, P. Teal, S. Phillips, C. Voll, D. Howse, J. Teitelbaum, D. Rivest, H. Desai, R. Arts, D. Stewart, A. Durocher, M. Lamothe, L. Berger, D. Gladstone, P. Bailey, M. Hill; Chile — V. DГaz Tapia, A. Hoppe, R. Maturana Dasori; China — C. Lu, X. Wang, S. Ding, Y. Wang, L. Cui, Y. Huang, J. Sheng Zeng, E. Xu, Z. Zhang, L. Miao; Czech Republic — G. Waberzinek, K. UrbГЎnek, J. Bauer, M. Bar, D. VГЎclavГk, E. Ehler, H. Lachmann, O. Е koda; France — A. Bonafe, J. Boulliat, P. Amarenco, F. Ziegler, T. Moulin, D. Sablot, M. Bataillard, J.F. Albucher, F. Rouanet, F. Nicoli, I. Crassard, F. Pico, H. Hosseini; Germany — J. Glahn, D. Schneider, M. Rosenkranz, A. Hetzel, P. Vogel, G. Hamann, P. Ringleb; Greece — K. Vemmos, K. Karageorgio, G. Georgiadis; Hong Kong, China — L. Wong, T. Hong Tsoi; Hungary — S. HorvГЎth, A. CsГЎnyi, C. BГ©la, N. Szegedi; Israel — D. Yarnitsky, J. Streifler, R. Milo, B. Weller, B. Gross, D. Tanne, T. Lampl, J. Rabey, N. Bornstein, S. Honigman, I. Wirguin, R. Leker; Korea — J.S. Kim, B.C. Lee; Mexico — C. Brito Cantu, S. Ruiz, M. Hector, J. Rodriguez, L. Rivera, G. Aguayo, F. Leon, B. Vega, G. Osorno; Philippines — A. Aquino, C. Chua, M.C. San Jose, A. DГaz, J. Navarro, A. Baroque; Poland — A. CzЕ‚onkowska, A. KuczyЕ„ska, B. GaweЕ‚, A. Buczek, M. Jackowski, M. Glonek, P. Nowacki, G. Chabik, Z. Stelmasiak, H. Kwieciski; Portugal — A. Vasco Salgado, L. Cunha, M. Tuna, G. Goncalves, T. Pinho e Melo, M. Rodigues; Russia — V. Skvortsova, Z. Suslina, A. Lebedeva, Y. Kolomoyetz, V. Shmirev, A. Skoromets, A. Fedin; Singapore — R. Gan, B. Chan, H.M. Chang; Slovakia — M. DvorГЎk, M. Brozman, E. KurДЌa, J. Vyletelka, J. HerГ©nВyiuvГЎ; South Africa — M. Bassoon, J. Thorne, J.S. Roos, M. Isaacs; Spain — F. Rubio, J.S. Leal, J. Roquer, A. Chamorro, J. Vivancos, J. Castillo, M. Lozano, C. Molina; Switzerland — H. Mattle, B. Tettenborn, J. Bogousslavsky, H. HungerbГјhler, R. Baumgartner, P. Lyrer; Taiwan — H.H. Hu, S.T. Chen; United States — M. Harris, M. Sauter, N. Culligan, W. Truax, D. Koons, R. Hull, W. Holt, K. Madden, F. Abbott, S. Braheny, C. Chang, B. Cucchiara, C. Graffagnino, J. Gross, J. Grotta, P. Katz, R. Kelley, N. Papamitsakis, J. Freiberg, J. Schim, J. Harris, V. Salanga, A. Bernstein, M. Brody, C. Gomez, A. Ahuja, F. Chang, D. Chiu, M. Concha, J. Couch, B. Dandapani, B. Demaerschalk, F. Diamond, B. Dihenia, J. Dissin, R. Jackel, M. Jacoby, K. John, D. Krieger, L. Labiche, L. Larsen, D. Leifer, E. Wilson, M. Young, R. Reichwein, M. Reiss, R. Ringel, N. Rodgers-Neame, J. Sander, D. Saur, R. Schechter, C. Villar, D. Chen, I. Altafullah, P. Ash, J. Wulff, C. Imbus, A. Felix, C. Kososky, T. Habiger, C.H. Liu, S. Mallenbaum, K. Ng, R. Brooks, K. Levin, H. Sachdev, J. Bertoni, R. Stephens, S. Fox, D. Brock, E. Crisostomo, J. Wang, M. Nash, P. Akins, N. Badjatia, D. Wright, D. Lefkowitz, J. Liss, P. Mazzeo, J. McDowell, M. Tremwel, E. Albakri, J. Belden, T. Bell, P. Blachman, C. Boutwell, F. Campanella, A. Walker, V. Erlich, J. Gebel, L. Glass, B. Grayum, J. Hanna, D. Heiselman, W. Hickling, J. Hollander, N. Iannuzzi, T. Henmen, A. Majid, M. Moonis, C. Morgan, G. Newman, R. O’Connor, E. Oribe, T. Wei, M. Schneck, I. Silverman, R. Smith, S. Starkman, M. Tabbaa, D. Tamulonis, M. Torbey, L. Wechsler, A. Turel, J. Waxler, V. Mangeshkumar, R. Libman, S. Martino, D. Morris, H. Edmonds, S. Cohen, F. Munschauer, J. Bobenhouse, R. Taylor, W. Honeycutt, C. Brondos, S. Wolf, J. Jacobsen, R. Paschall, D. Hill, L. Brass, D. Dietrich, H. Kirshner, C. Fanale, W. Justiz, G. Albers, W. Clark, T. Ashizawa, J. Stafford, M. Rubin, G. Ferencz, W. Likosky, J. Frey, C. Perkins, E. Hekler, G. Howell, M. Alberts; United Kingdom: K.R. Lees, G.A. Ford, K. Muir. References 1. O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH, Howells DW. 1026 Experimental treatments in acute stroke. Ann Neurol 2006;59:467-77. 2. Green AR, Shuaib A. Therapeutic strategies for the treatment of stroke. Drug Discov Today 2006;11:681-93. 3. Lees KR, Zivin JA, Ashwood T, et al. NXY-057 for acute ischemic stroke. N Engl J Med 2006;354:588-600. 4. Lees KR, Davalos A, Davis SM, et al. Additional outcomes and subgroup analyses of NXY-059 for acute ischemic stroke in the SAINT I Trial. Stroke 2006;37:2970-8. 570 5. Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989;20:864-70. 6. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976;16:31-41. 7. van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988;19:604-7. 8. Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J 1965;14:61-5. 9. Quinn TJ, Lees KR, Hardemark HG, Dawson J, Walters MR. Initial experience of a digital training resource for modified Rankin scale assessment in clinical trials. Stroke (in press). 10. Koch GG, Edwards S. Clinical efficacy trials with ordinal data. In: Peace KK, ed. Biopharmaceutical statistics for drug development. New York: Marcel Dekker, 1988:403-57. 11. Stokes ME, Davis CS, Koch GG. Categorical data analysis using the SAS system. 2nd ed. Cary, NC: SAS Institute, 2000. n engl j med 357;6  www.nejm.org  august 9, 2007 NXY-059 for Acute Ischemic Stroke 12. Kuroda S, Tsuchidate R, Smith M-L, Maples KR, SiesjГ¶ BK. Neuroprotective effects of a novel nitrone, NXY-059, after transient focal cerebral ischemia. J Cereb Blood Flow Metab 1999;19:778-87. 13. Lapchak PA, Araujo DM, Song D, Wei J, Purdy R, Zivin JA. Effects of the spin trap agent disodium-[tert-butylimino)methyl] benzene-1,3-disulfonate N-Oxide (generic NXY-059) on intracerebral hemorrhage in a rabbit large clot embolic stroke model: combination studies with tissue plas- minogen activator. Stroke 2002;33:166570. 14. Stroke Therapy Academic Industry Roundtable (STAIR). Recommendations for standards regarding preclinical neuroprotective and restorative drug development. Stroke 1999;30:2752-8. 15. Stroke Therapy Academic Industry Roundtable II (STAIR-II). Recommendations for clinical trial evaluation of acute stroke therapies. Stroke 2001;32:1598-606. 16. Fisher M, Stroke Therapy Academic Industry Roundtable. RecommendaВtions for advancing development of acute stroke therapies: Stroke Therapy Academic Industry Roundtable 3. Stroke 2003;34:153946. 17. MR Stroke Collaborative Group, Phan TG, Donnan GA, Davis SM, Byrnes G. Proof of principle phase II MRI studies in stroke: sample size estimates from dichotomous and continuous data. Stroke 2006; 37:2521-5. Copyright В© 2007 Massachusetts Medical Society. n engl j med 357;6  www.nejm.org  august 9, 2007 571 The n e w e ng l a n d j o u r na l of m e dic i n e clinical practice Acute Ischemic Stroke H. Bart van der Worp, M.D., Ph.D., and Jan van Gijn, F.R.C.P. This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the authors’ clinical recommendations. A 62-year-old man has sudden weakness of the left arm and leg and slurred speech. Except for untreated hypertension, his medical history is unremarkable. He is a current smoker with a smoking history of 45 pack-years. On arrival at the emergency department 1 hour 15 minutes after the onset of symptoms, he reports no headache or vomiting. His blood pressure is 180/100 mm Hg, and his pulse is 76 beats per minute and is regular. Neurologic examination shows dysarthria, a left homonymous hemianopia, severe left-sided weakness, and a failure to register light touch on the left side of the body when both sides are touched simultaneously (left tactile extinction). How should this patient be evaluated and treated in the short term? The Cl inic a l Probl e m From the Department of Neurology, Rudolf Magnus Institute of Neuroscience, University Medical Center Utrecht, Utrecht, the Netherlands. Address reprint requests to Dr. van der Worp at the Department of Neurology, Rudolf Magnus Institute of Neuroscience, University MedВ ical Center Utrecht, Heidelberglaan 100, 3584 CX Utrecht, the Netherlands, or at h.b.vanderworp@umcutrecht.nl. N Engl J Med 2007;357:572-9. Copyright В© 2007 Massachusetts Medical Society. Stroke ranks second after ischemic heart disease as a cause of lost disability-adjusted life-years in high-income countries and as a cause of death worldwide.1 The incidence of stroke varies among countries and increases exponentially with age. In Western societies, about 80% of strokes are caused by focal cerebral ischemia due to arterial occlusion, and the remaining 20% are caused by hemorrhages.2 Ischemic brain injury is thought to result from a cascade of events from energy depletion to cell death. Intermediate factors include an excess of extracellular excitatory amino acids, free-radical formation, and inflammation.3 Initially after arterial occlusion, a central core of very low perfusion is surrounded by an area of dysfunction caused by metabolic and ionic disturbances but in which structural integrity is preserved (the ischemic penumbra). In the first minutes to hours, therefore, clinical deficits do not necessarily reflect irreversible damage. Depending on the rate of residual blood flow and the duration of ischemia, the penumbra will eventually be incorporated into the infarct if reperfusion is not achieved (Fig. 1).3 Thirty-day case fatality rates for ischemic stroke in Western societies generally range between 10 and 17%.2 The likelihood of a poor outcome after stroke increases with increasing age, with the coexistence of diseases such as ischemic heart disease and diabetes mellitus, and with increasing size of the infarct. The likelihood also varies according to the infarct site. Mortality in the first month after stroke has been reported to range from 2.5% in patients with lacunar infarcts4 to 78% in patients with space-occupying hemispheric infarction.5 S t r ategie s a nd E v idence Acute stroke is typically characterized by the sudden onset of a focal neurologic deficit, though some patients have a stepwise or gradual progression of symptoms. Common deficits include dysphasia, dysarthria, hemianopia, weakness, ataxia, sensory loss, and neglect. Symptoms and signs are unilateral, and consciousness is 572 n engl j med 357;6  www.nejm.org  august 9, 2007 clinical pr actice generally normal or impaired only slightly, except rare cases, such as if infective endocarditis is in the case of some infarcts in the posterior cir- suspected. In the days thereafter, transthoracic culation. echocardiography or, preferably, transesophageal echocardiography may be indicated to rule out Initial Assessment cardioembolism. In the majority of cases of stroke, making the diagnosis is straightforward. However, especially Imaging in patients with unusual features (e.g., gradual on- Cerebral infarction cannot be distinguished with set, seizure at the onset of symptoms, or impaired certainty from intracerebral hemorrhage on the consciousness), the differential diagnosis should basis of symptoms and signs alone. In all patients include migraine, postictal paresis, hypoglyce- with suspected ischemic stroke, computed tomogmia, conversion disorder, subdural hematoma, raphy (CT) or magnetic resonance imaging (MRI) and brain tumors. of the brain is therefore required. Noncontrast Atherosclerosis (leading to thromboembolism CT may suffice (Fig. 2); as compared with MRI, or local occlusion) and cardioembolism are the it is more widely available, faster, less susceptible leading causes of brain ischemia. However, un- to motion artifacts, and less expensive. Both CT usual causes should be considered, especially if and MRI have a high sensitivity for acute intrapatients are younger (e.g., below 50 years of age) cranial hemorrhage, but MRI has a much higher and have no apparent cardiovascular risk factors. sensitivity than CT for acute ischemic changes, Some clinical clues that suggest alternative diag- especially in the posterior fossa and in the first noses are ptosis and miosis contralateral to the deficit (carotid-artery dissection), fever and a cardiac murmur (infective endocarditis), and headache and an elevated erythrocyte sedimentation rate in patients older than 50 years of age (giantcell arteritis). Deficits should be assessed by careful neurologic examination. Several scales have been developed to quantify the severity of the neurologic Figure 1. Progression over Time (Left to Right) of the Infarct Core (Red), with Irreversible Damage at the Expense of the Ischemic Penumbra (Green). deficit, mainly for use in research studies; the National Institutes of Health Stroke Scale6 is most often used. An irregular pulse suggests atrial fibrillation. A very high blood pressure may signal hypertensive encephalopathy and precludes B A C thrombolysis if sustained at or above 185/110 RETAKE 1st mm Hg. Carotid bruits lack sufficient sensitivity AUTHOR Van De Worp ICM 2nd REG F FIGURE f1 and specificity for a diagnosis of severe carotid 3rd CASE 7 TITLE stenosis. Revised EMail Line 4-C Laboratory testing during the acute phase SIZE Enon ARTIST: mleahy H/T H/T 22p3 should include measurement of the glucose level FILL Combo (since hypoglycemia may also cause focal neuroAUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. logic deficits), a complete blood count, and meaPlease check carefully. surement of the prothrombin time and partialJOB: 35706 ISSUE: 08-09-07 thromboplastin time, particularly if thrombolysis Figure 2. CT Scans Obtained 1 Hour 40 Minutes after the Onset of Symptoms is considered. An electrocardiogram may reveal Suggestive of Cortical Stroke in the Territory of the Right Middle Cerebral atrial fibrillation or an acute or previous myoArtery. cardial infarction as potential causes of thromboВ An unenhanced CT scan (Panel A) shows a slight loss of differentiation of embolism. Because stroke may be complicated by gray and white matter in the basal ganglia (arrows). A CT angiographic image myocardial ischemia and arrhythmias, cardiac shows occlusion of the first segment of the right middle cerebral artery monitoring is recommended for at least the first (Panel B, arrow) and atherosclerotic lesions in the carotid bifurcation RETAKE 1st AUTHOR carotid VanDeartery Worp is not shown. ICMThe external В(Panel C, arrow). 24 hours.8 Echocardiography in the first hours 2nd REG F FIGURE 2a-c after the onset of stroke is necessary only in 3rd CASE TITLE EMail Enon n engl j med 357;6  www.nejm.org  ARTIST: mleahy augustFILL 9, 2007 Line H/T Combo 4-C H/T Revised SIZE 22p3 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. JOB: 35706 ISSUE: 08-09-07 573 n e w e ng l a n d j o u r na l The hours after an ischeВmic stroke.9 Cytotoxic edema is detectable within minutes after the onset of ischemia, with a reduced apparent diffusion coefficient on diffusion-weighted imaging (Fig. 3).10 However, it remains unclear whether early visualization of ischemia has important implications for management. For patients in whom acute invasive treatment strategies (such as intraarterial thrombolysis or mechanical clot retrieval) are considered, urgent CT or magnetic resonance angiography is useful to identify the site of arterial occlusion (Fig. 2). Either method can provide complete visualization from the aortic arch to the circle of Willis and beyond.10 Carotid duplex ultrasonography and transcranial Doppler ultrasonography have also been used to detect the site of occlusion.10 intravenous Thrombolysis The National Institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator (NINDS rt-PA) Stroke Study, a multicenter, randomized trial, has demonstrated the efficacy of treatment with intravenous rt-PA (alteplase) started within 3 hours after the onset of symptoms.11 Among patients treated with rt-PA (0.9 mg per kilogram of body weight, with 10% of the dose administered as a bolus and the rest infused over 1 hour and a maximum total dose of 90 mg), 31 to 50% had a favorable neurologic or functional outcome at 3 months (depending on the scale used), as compared with 20 to 38% of patients given placebo; mortality rates were similar in the two groups. Symptomatic intracranial hemorrhage A B C Figure 3. MRI Scans Obtained 2 Days after the Onset of Ischemic Stroke in the Territory of the Right Middle Cerebral Artery. RETAKE 1st AUTHOR Van De Worp A hyperintense ICM lesion in the temporal and frontal lobes and in the basal gan2nd REG F FIGURE 3 a,c glia is shown on fluid-attenuated inversion recovery (Panel A) and 3rddiffusionCASE TITLE Revised weighted imaging (Panel B), corresponding to a reduced apparent diffusion EMail Line 4-C coefficient (Panel C). Similar changes may be observed on diffusion-weighted SIZE Enon ARTIST: mleahy H/T H/T imaging in the FILL first hours after the onset of symptoms. 22p3 Combo AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. 574 JOB: 35706 ISSUE: of m e dic i n e occurred in 6.4% of patients treated with intravenous rt-PA and in 0.6% of controls. Four other trials of intravenous rt-PA therapy given within 6 hours after the onset of symptoms (with few patients treated within 3 hours) failed to find a benefit of thrombolysis separately, but if analyzed in combination, they provided support for a benefit of treatment administered within the first 3 hours after stroke.12,13 Even within the 3-hour time frame, the benefit of rt-PA is greater the sooner treatment is started.13 The risk of symptomatic intracranial hemorrhage after thrombolysis is higher in patients with more severe strokes and with increased age.14 However, a post hoc subgroup analysis of the NINDS rt-PA Stroke Study found no significant differences in the benefit from rt-PA therapy across these and other subgroups,15 but the numbers of patients in each subgroup were small. Similar concerns have been raised about the efficacy and safety of rt-PA in patients with early ischemic changes on CT. Other post hoc analyses of data from the NINDS rt-PA Stroke Study showed that in the first 3 hours after the onset of symptoms, the appearance of ischemic changes on CT was not an independent predictor of an increased risk of symptomatic intracranial hemorВ rhage or other adverse outcomes after treatment with rt-PA.16 Several observational studies have suggested that intravenous thrombolysis with rt-PA can be used in the community setting with efficacy and safety similar to that found in the randomized trials.17,18 Other Treatments Aspirin In two large randomized trials, the use of aspirin (160 or 300 mg per day), initiated within 48 hours after the onset of stroke and continued for 2 weeks or until discharge, led to reduced rates of death or dependency at discharge or at 6 months,19,20 probably by means of reducing the risk of recurrent ischemic stroke. In both trials, the routine use of aspirin was recommended as secondary prevention after the first few weeks. Although the benefit was small (77 patients would need to be treated to prevent a poor outcome in 1 patient), aspirin is inexpensive, has a good safety profile, and appears to be effective across the range of patients with ischemic stroke.21 Because the effect of aspirin in combination with rt-PA is uncertain, it seems wise to withhold aspirin for 24 hours in n engl j med 357;6  www.nejm.org  august 9, 2007 08-09-03 clinical pr actice patients treated with the use of intravenous thrombolysis. The use of dipyridamole or clopidogrel in the acute phase of ischemic stroke has not been tested in randomized trials. A meta-analysis of six randomized trials involving 21,966 patients found no evidence that the use of anticoagulants (unfractionated heparin, lowmolecular-weight heparins, heparinoids, thrombin inhibitors, or oral anticoagulants) in the acute phase of stroke improves functional outcomes.22 According to this analysis, nine fewer cases of recurrent ischemic stroke would be expected per 1000 patients treated, but so would nine more cases of symptomatic intracranial hemorrhage.22 A meta-analysis of seven trials similarly failed to show improvement in functional outcome with the use of anticoagulant therapy in patients with acute cardioembolic stroke.23 ment in 93 patients 60 years of age or younger with space-occupying infarction in the territory of the middle cerebral artery, surgical treatment in the first 48 hours after the onset of stroke reduced both the case fatality rate (22%, vs. 71% in the medical-management group) and the rate of moderately severe or severe disability or death (57% vs. 79%).29 Surgery appeared to be less beneficial for patients with aphasia (vs. those without aphasia), patients older than 50 years of age (vs. those 50 years of age or younger), and patients in whom surgery was performed on the second day after the onset of stroke (vs. the first day after onset); however, the numbers of patients in these subgroups were small. Data from randomized and other trials indicate that patients who receive care in a stroke unit are more likely to survive, regain independence, and return home than are those who do not receive such organized care.30 Prevention and Management of Complications Strategies to Reduce Risk of Recurrent Stroke or Other Cardiovascular Events Nutrition is often compromised in patients admitted to the hospital with stroke. However, in randomized trials, neither the routine use of oral nutritional supplements24 nor early tube feeding25 to prevent or treat undernutrition in hospitalized patients with stroke resulted in improved longterm functional outcome. Patients with acute stroke are at increased risk for deep venous thrombosis and pulmonary embolism, and the risk increases with increasing age and stroke severity.26 Although the use of anticoagulants does not improve overall functional outcomes, the use of subcutaneously administered low-dose unfractionated heparin or low-molecularweight heparin has been recommended in patients at high risk for deep venous thrombosis, such as patients who are immobile (e.g., due to paralysis of a leg).8,27 In patients with large supratentorial infarcts, space-occupying brain edema may lead to transtentorial or uncal herniation, usually between the second and fifth days after the onset of stroke.5 Case series of such patients in intensive care units have reported early case fatality rates of up to 78%.5 No medical therapy has proved effective.28 In a pooled analysis of three randomized trials comparing surgical treatment (hemicraniectomy and duraplasty, the insertion of a dural patch to enlarge the intradural space) with medical treat- In patients presenting with stroke, attention to secondary prevention of stroke and other cardiovascular complications is routinely warranted. Although space limitations preclude a detailed discussion of recommended strategies, they include the use of low-dose aspirin and dipyridamole in patients with ischemic stroke of arterial origin31; oral anticoagulation in patients with cardiac embolism; treatment of hypertension; statin therapy for the lowering of lipid levels; glucose control in patients with diabetes; smoking cessation; and carotid endarterectomy in patients with substantial ipsilateral carotid stenosis. These issues have been discussed in detail elsewhere.32,33 Anticoagulant Therapy A r e a s of Uncer ta in t y Even in high-income countries such as the United States, only a small minority of patients with acute ischemic stroke receive intravenous rt-PA.34 Its use is currently restricted to a 3-hour time window after the onset of symptoms, on the basis of results of the NINDS rt-PA Stroke Study,11 but a pooled analysis of six randomized trials has suggested a potential benefit within up to 6 hours after the onset of stroke.13 Trials assessing treatment in this extended time frame among broad populations of patients with ischemic stroke are under way. n engl j med 357;6  www.nejm.org  august 9, 2007 575 The n e w e ng l a n d j o u r na l Preliminary data have suggested that the identification of patients who would benefit from thrombolysis beyond a 3-hour interval might be improved by quantification of the ischemic penumbra with the use of diffusion–perfusion MRI or perfusion CT techniques (Fig. 4).35-37 This suggestion requires further study. Although the intent of intravenous thrombolysis is to recanalize occluded arteries, none of the pivotal clinical trials tested whether recanalization actually occurred. Other studies have shown that complete recanalization of an occluded middle cerebral artery 2 hours after the start of thrombolysis was achieved in only up to one third of patients.38,39 In one controlled trial, continuous 2-MHz transcranial Doppler ultrasonography applied for 2 hours augmented the rate of rt-PA– induced arterial recanalization.38 Limited data suggest that the addition of intravenous galactose–based microbubbles to this treatment strategy may further increase rates of recanalization.39 Because it is still uncertain whether additional measures to improve perfusion also improve functional outcome, these techniques cannot be recommended for use outside clinical trials. As compared with intravenous thrombolysis, intraarterial thrombolysis may increase the likelihood of recanalization, but the two strategies have not been directly compared in a sufficiently large randomized trial. In a small randomized trial, the administration of both intraarterial recombinant prourokinase and intravenous heparin, as compared with intravenous heparin alone, within 6 hours after the onset of stroke resulted in a higher rate of recanalization of the middle cerebral artery (66% vs. 18%) and a higher rate 14.9 A 20 B 10.2 15 5.6 10 1.0 5 3.7 0 C Combo AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. 576 JOB: 35706 ISSUE: m e dic i n e of a favorable functional outcome (no disability to slight disability) at 3 months (40% vs. 25%, P = 0.04).40 However, the procedures required to deliver the thrombolytic agent to the site of vascular occlusion involve more time than does intraВ venous therapy. Thrombolytic “bridging therapy,” in which intravenous thrombolysis is followed by intraarterial thrombolysis,41 could permit more rapid treatment and improved rates of recanalization but is resource intensive, limiting widespread application. Mechanical thrombectomy in patients with acute intracranial occlusion of the intracranial carotid artery has resulted in a high rate of recanalization in case series,42 but controlled trials are lacking. Other Treatments High blood pressure,43 a high serum glucose level,44 and a high body temperature45 in the first hours to days after ischemic stroke have all been associated with poor long-term outcomes. The effects of the early lowering of blood pressure and maintenance of normothermia and normoglycemia are currently being tested in large randomized trials.43,46,47 Data from randomized trials are needed to guide the management of blood pressure in the context of acute stroke. Given concerns about adВ verse effects of the short-term lowering of blood pressure on cerebral perfusion, current guidelines based on consensus opinion recommend withholding antihypertensive therapy during the acute phase of stroke unless the diastolic blood pressure exceeds 120 mm Hg or the systolic blood pressure exceeds 220 mm Hg in patients who are not candidates for rt-PA.8 Blood-pressure monitoring is recommended before, during, and after rt-PA therapy, and intravenous antihypertensive therapy is recommended to maintain the systolic blood pressure below 180 mm Hg and the diastolic blood pressure below 105 mm Hg. Neuroprotection Figure 4. Perfusion CT Scans Obtained 1 Hour 45 Minutes after the Onset of Ischemia in the Territory of the Right Middle Cerebral Artery. RETAKE 1st AUTHOR Van De mean Worp transit time ICM prolongation A large area shows of the (in seconds) 2nd F FIGURE 4 a_c a reduction in cerebral blood (Panel A), and aREG smaller area shows volume 3rd (in milliliters perCASE 100 g)TITLE (Panel B). These two maps suggest a large penumbra Revised EMail Linepenumbra 4-C shown in green and and a small infarct core (Panel C, with the SIZE Enon ARTIST: mleahy H/T H/T the suggested infarct core in red). 22p3 FILL of Hundreds of neuroprotective strategies have been shown to improve outcome in animal models of focal cerebral ischemia,48 but thus far only rt-PA and aspirin have been shown to be clearly efficacious in patients. Although early data suggested a possible benefit of the free-radical–trapping agent NXY-059 in acute ischemic stroke,49 a large multicenter trial reported on by Shuaib et al. in this issue of the Journal showed no improvement in n engl j med 357;6  www.nejm.org  august 9, 2007 08-09-07 clinical pr actice functional outcomes of patients who were treated with this agent within 6 hours after the onset of symptoms.50 Hypothermia has been shown to reduce infarct volume and improve neurologic outcomes in animal models of focal cerebral ischemia51; it has also improved functional outcomes in randomized clinical trials involving patients with global cerebral ischemia after cardiac arrest,52,53 but the improvement was not consistent among those with traumatic brain injury.54 Large clinical trials testing the effect of hypothermia in paВ tients with acute ischemic stroke are warranted. Guidel ine s from Profe s siona l S o cie t ie s Table 1. Main Contraindications to Intravenous Thrombolysis in Patients with Acute Ischemic Stroke.* Onset of symptoms >3 hr before start of treatment Intracranial hemorrhage on CT or MRI Head trauma or stroke in previous 3 mo Myocardial infarction in previous 3 mo Gastrointestinal or urinary tract hemorrhage in previous 21 days Major surgery in previous 14 days History of intracranial hemorrhage Systolic blood pressure ≥185 mm Hg or diastolic blood pressure ≥110 mm Hg Evidence of active bleeding or acute trauma on examination Use of oral anticoagulants and an INR ≥1.7 Use of heparin in previous 48 hr and a currently prolonged aPTT Platelet count <100,000 per cubic millimeter Blood glucose level <50 mg/dl (2.7 mmol/liter) Seizure with postictal residual neurologic impairments 8 from Adams et al., which provides a more complete overview of inPractice guidelines have been issued by the Stroke *Adapted dications and contraindications. INR denotes international normalized ratio, Council of the American Heart Association and and aPTT activated partial-thromboplastin time. the American Stroke Association8 and by the European Stroke Initiative.55 The recommendations in this article are generally consistent with those tient presented within 3 hours after the onset of guidelines. symptoms, we would recommend therapy with intravenous rt-PA. We would start aspirin after 24 hours (300 mg daily for the first 2 weeks) and C onclusions would then administer lower-dose aspirin and dia nd R ec om mendat ions pyridamole for secondary prevention. Aggressive The patient described in the vignette had a sudden management of other cardiovascular risk factors left-sided hemiparesis, strongly suggestive of a — including encouraging the patient to stop smokВ right hemisphere stroke. CT or MRI of the brain ing, treating his hypertension, and initiating statin should be performed promptly; MRI is more sen- therapy — is also warranted. sitive for early ischemic changes, but either methDr. van der Worp reports receiving lecture fees from GlaxoВ od can fully rule out hemorrhage. In the absence SmithKline, Pfizer, and Servier; and Dr. van Gijn, consulting and of bleeding or other contraindications to throm- lecture fees from Sanofi-Aventis. No other potential conflict of bolysis (e.g., spontaneous, complete clearing of interest relevant to this article was reported. We thank Audrey Tiehuis, M.D., for providing the scans shown the deficits or an increase in blood pressure to in Figures 2 and 4 and L. Jaap Kappelle, M.D., for his valuable 185/110 mm Hg or more) (Table 1), since the pa- comments on an early version of the manuscript. References 1. Lopez AD, Mathers CD, Ezzati M, JamiВ son DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet 2006;367:1747-57. 2. Feigin VL, Lawes CM, Bennett DA, Anderson CS. Stroke epidemiology: a review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol 2003;2: 43-53. 3. Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: an inВ tegrated view. Trends Neurosci 1999;22: 391-7. 4. Norrving B. Long-term prognosis after lacunar infarction. Lancet Neurol 2003; 2:238-45. 5. Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, von Kummer R. вЂ�Malignant’ middle cerebral artery infarction: clinical course and prognostic signs. Arch Neurol 1996;53:309-15. 6. Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke 1989;20:864-70. 7. Hankey GJ, Warlow CP. Symptomatic carotid ischaemic events: safest and most cost effective way of selecting patients for angiography, before carotid endarterectomy. BMJ 1990;300:1485-91. 8. Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/ American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007;386:1655-711. [Erratum, Stroke 2007;38(6):e38.] 9. Chalela JA, Kidwell CS, Nentwich LM, n engl j med 357;6  www.nejm.org  august 9, 2007 577 The n e w e ng l a n d j o u r na l et al. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet 2007;369:293-8. 10. Muir KW, Buchan A, von Kummer R, Rother J, Baron JC. Imaging of acute stroke. Lancet Neurol 2006;5:755-68. 11. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-7. 12. Wardlaw JM, Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischaeВ mic stroke. Cochrane Database Syst Rev 2003;3:CD000213. 13. Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004;363:768-74. 14. Khatri P, Wechsler LR, Broderick JP. Intracranial hemorrhage associated with revascularization therapies. Stroke 2007; 38:431-40. 15. NINDS t-PA Stroke Study Group. Generalized efficacy of t-PA for acute stroke: subgroup analysis of the NINDS t-PA Stroke Trial. Stroke 1997;28:2119-25. 16. Patel SC, Levine SR, Tilley BC, et al. Lack of clinical significance of early ischeВ mic changes on computed tomography in acute stroke. JAMA 2001;286:2830-8. 17. Graham GD. Tissue plasminogen activator for acute ischemic stroke in clinical practice: a meta-analysis of safety data. Stroke 2003;34:2847-50. 18. Wahlgren N, Ahmed N, DГЎvalos A, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet 2007;369:275-82. [Erratum, Lancet 2007;369:826.] 19. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute ischaemic stroke. Lancet 1997;349:1569-81. 20. CAST (Chinese Acute Stroke Trial) Collaborative Group. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaeВ mic stroke. Lancet 1997;349:1641-9. 21. Chen ZM, Sandercock P, Pan HC, et al. Indications for early aspirin use in acute ischemic stroke: a combined analysis of 40 000 randomized patients from the Chinese Acute Stroke Trial and the International Stroke Trial. Stroke 2000;31:1240-9. 22. Gubitz G, Sandercock P, Counsell C. Anticoagulants for acute ischaemic stroke. Cochrane Database Syst Rev 2004; 3:CD000024. 23. Paciaroni M, Agnelli G, Micheli S, Caso V. Efficacy and safety of anticoagulant treatment in acute cardioembolic 578 of m e dic i n e stroke: a meta-analysis of randomized controlled trials. Stroke 2007;38:423-30. 24. Dennis MS, Lewis SC, Warlow C. Routine oral nutritional supplementation for stroke patients in hospital (FOOD): a multiВ centre randomised controlled trial. Lancet 2005;365:755-63. 25. Idem. Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): a multicentre randomised controlled trial. Lancet 2005;365:764-72. 26. Kelly J, Rudd A, Lewis R, Hunt BJ. Venous thromboembolism after acute stroke. Stroke 2001;32:262-7. 27. Francis CW. Prophylaxis for thromboembolism in hospitalized medical patients. N Engl J Med 2007;356:1438-44. 28. Hofmeijer J, van der Worp HB, Kappelle LJ. Treatment of space-occupying hemispheric infarction. Crit Care Med 2003;31:617-25. 29. Vahedi K, Hofmeijer J, Juettler E, et al. Early decompressive surgery in malignant infarction of the middle cerebral artery: a pooled analysis of three randomised controlled trials. Lancet Neurol 2007;6:215-22. 30. Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst Rev 2002; 1:CD000197. 31. Halkes PH, van Gijn J, Kappelle LJ, Koudstaal PJ, Algra A. Aspirin plus dipyridВ amole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet 2006; 367:1665-73. [Erratum, Lancet 2007;369: 274.] 32. Johnston SC. Transient ischemic attack. N Engl J Med 2002;347:1687-92. 33. Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Stroke 2006;37:577-617. 34. Douglas VC, Tong DC, Gillum LA, et al. Do the Brain Attack Coalition’s criteria for stroke centers improve care for ischeВ mic stroke? Neurology 2005;64:422-7. 35. Kidwell CS, Alger JR, Saver JL. Beyond mismatch: evolving paradigms in imaging the ischemic penumbra with multimodal magnetic resonance imaging. Stroke 2003; 34:2729-35. 36. Wintermark M, Flanders AE, Velthuis B, et al. Perfusion-CT assessment of infarct core and penumbra: receiver operating characteristic curve analysis in 130 patients suspected of acute hemispheric stroke. Stroke 2006;37:979-85. 37. Albers GW, Thijs VN, Wechsler L, et al. Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol 2006; 60:508-17. 38. Alexandrov AV, Molina CA, Grotta JC, et al. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med 2004;351:2170-8. 39. Molina CA, Ribo M, Rubiera M, et al. Microbubble administration accelerates clot lysis during continuous 2-MHz ultrasound monitoring in stroke patients treatВ ed with intravenous tissue plasminogen activator. Stroke 2006;37:425-9. 40. Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke — the PROACT II Study: a randomized controlled trial. JAMA 1999; 282:2003-11. 41. The IMS Study Investigators. Combined intravenous and intra-arterial recanalization for acute ischemic stroke: the Interventional Management of Stroke Study. Stroke 2004;35:904-11. 42. Flint AC, Duckwiler GR, Budzik RF, Liebeskind DS, Smith WS. Mechanical thrombectomy of intracranial internal carotid occlusion: pooled results of the MERCI and Multi MERCI Part I trials. Stroke 2007;38:1274-80. 43. Willmot M, Leonardi-Bee J, Bath PM. High blood pressure in acute stroke and subsequent outcome: a systematic review. Hypertension 2004;43:18-24. 44. Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke 2001;32:2426-32. 45. Reith J, JГёrgensen S, Pedersen PM, et al. Body temperature in acute stroke: relation to stroke severity, infarct size, mortality, and outcome. Lancet 1996;347:422-5. 46. van Breda EJ, van der Worp HB, van Gemert HM, et al. PAIS: Paracetamol (Acetaminophen) In Stroke; protocol for a randomized, double blind clinical trial. BMC Cardiovasc Disord 2005;5:24. 47. Gray CS, Hildreth AJ, Alberti GK, O’Connell JE. Poststroke hyperglycemia: natural history and immediate management. Stroke 2004;35:122-6. [Erratum, Stroke 2004;35:1229.] 48. O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH, Howells DW. 1,026 Experimental treatments in acute stroke. Ann Neurol 2006;59:46777. 49. Lees KR, Zivin JA, Ashwood T, et al. NXY-059 for acute ischemic stroke. N Engl J Med 2006;354:588-600. 50. Shuaib A, Lees KR, Lyden P, et al. NXY-059 for the treatment of acute ischemic stroke. N Engl J Med 2007;357:56271. 51. van der Worp HB, Sena ES, Donnan GA, Howells DW, Macleod MR. Hypothermia in animal models of acute ischaemic stroke: a systematic review and meta-analyВ sis. Brain (in press). n engl j med 357;6  www.nejm.org  august 9, 2007 clinical pr actice 52. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of outof-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002;346:55763. 53. Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypother- mia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002; 346:549-56. [Erratum, N Engl J Med 2002; 346:1756.] 54. McIntyre LA, Fergusson DA, HГ©bert PC, Moher D, Hutchison JS. Prolonged therapeutic hypothermia after traumatic brain injury in adults: a systematic review. JAMA 2003;289:2992-9. 55. Hack W, Kaste M, Bogousslavsky J, et al. European Stroke Initiative recommendations for stroke management — update 2003. Cerebrovasc Dis 2003;16:311-37. Copyright В© 2007 Massachusetts Medical Society. n engl j med 357;6  www.nejm.org  august 9, 2007 579 The n e w e ng l a n d j o u r na l of m e dic i n e review article current concepts Drug-Induced Immune Thrombocytopenia Richard H. Aster, M.D., and Daniel W. Bougie, Ph.D. From the Department of Medicine, Medical College of Wisconsin (R.H.A.), and the Blood Research Institute, BloodCenter of Wisconsin (R.H.A., D.W.B.) — both in Milwaukee. Address reprint requests to Dr. Aster at the Blood Research Institute, BloodCenter of Wisconsin, 8727 Watertown Plank Rd., Milwaukee, WI 53226-3548, or at richard.aster@bcw.edu. N Engl J Med 2007;357:580-7. Copyright В© 2007 Massachusetts Medical Society. D rug-induced thrombocytopenia can be caused by dozens, perhaps hundreds, of medications. Because thrombocytopenia can have many other causes, the diagnosis of drug-induced thrombocytopenia can easily be overlooked. On occasion, outpatients with drug-induced thrombocytopenia are treated for autoimmune thrombocytopenia and can have two or three recurrences before the drug causing the disorder is identified.1 In acutely ill, hospitalized patients, drug-induced thrombocytopenia can be overlooked because thrombocytopenia is attributed to sepsis, the effect of coronary-artery bypass surgery, or some other underlying condition. Although drug-induced thrombocytopenia is uncommon, it can have devastating, even fatal consequences that can usually be prevented simply by discontinuing the causative drug. It is therefore important that clinicians have a general understanding of this condition and the drugs that can cause it. In this review, we focus on conditions in which exposure to a drug leads to the destruction of circulating platelets, often accompanied by bleeding symptoms. We do not consider thrombocytopenia resulting from dose-dependent hematosuppression, which often occurs after treatment with chemotherapeutic and immunosuppressive agents such as cisplatin and cyclophosphamide.2 Although heparin-induced thrombocytopenia is the most common drug-related cause of a drop in the platelet count, we do not discuss this condition because of its complexity and because thrombosis, rather than thrombocytopenia, is the major threat to an affected patient. Because heparin is often given together with certain drugs that are likely to cause drug-induced thrombocytopenia (platelet inhibitors and vancomycin), it is important to distinguish between heparin-induced thrombocytopenia and druginduced thrombocytopenia. Heparin-induced thrombocytopenia was recently reviewed in the Journal.3 Drug-induced platelet destruction is usually caused by drug-induced antibodies, but this can be difficult to prove. In this review, we include many conditions for which an immune cause has not yet been fully documented. Although platelets are the preferred targets of drug-induced antibodies, drugs can also cause immune hemolytic anemia4 and neutropenia5 through similar mechanisms. Pr e sen tat ion Acute thrombocytopenia after exposure to quinine was recognized as a clinical entity about 140 years ago.6 Subsequently, many other medications were implicated in the development of this condition. Quinine, which is rarely used now as an antimalarial drug but is often prescribed for nocturnal muscle cramps, may still be the most common trigger. People of any age and either sex can be affected. The course of drug-induced thrombocytopenia in a representative patient is shown in Figure 1. Typically, a patient will have taken the sensitizing drug for about 1 week or intermittently over a longer period before presenting with petechial 580 n engl j med 357;6  www.nejm.org  august 9, 2007 current concepts Incidence The incidence of drug-induced thrombocytopenia is not well defined, in part because reporting is voluntary and is not critically reviewed. On the basis of several epidemiologic studies in the United States and Europe, the estimated minimum incidence is about 10 cases per million population per year but the number could be higher in selectВ ed groups, such as hospitalized patients and elderly people.10 A case–control study of patients in Massachusetts, Rhode Island, and Philadelphia showed that during each week of exposure, trimethoprim–sulfamethoxazole and quinine–quinВ idine caused thrombocytopenia in 38 and 26 of every 1 million users, respectively.11 Since these drugs carry relatively high risks of drug-induced thrombocytopenia, the rate at which most drugs cause the condition is probably lower. However, a few drugs (including abciximab and gold salts) cause immune thrombocytopenia in about 1% of patients. 3.0 2.5 Platelets (Г—10в€’5/mm3) hemorrhages and ecchymoses that are indicative of thrombocytopenia. Occasionally, symptoms deВ velop within 1 or 2 days after what is apparently the first exposure to a drug, particularly in patients given platelet inhibitors such as abciximab who may have preexisting, perhaps naturally occurring, antibodies.7 Systemic symptoms such as lightheadedness, chills, fever, nausea, and vomiting often precede bleeding symptoms. Severely affected patients have florid purpura and bleeding from the nose, gums, and gastrointestinal or urinary tract (“wet purpura”). In such cases, thrombocytopenia is invariably severe (<20,000 platelets per cubic millimeter). If the causative medication is stopped, symptoms usually resolve within 1 or 2 days, and the platelet count returns to normal in less than a week. For reasons that are poorly understood, patients with drug-induced thrombocytopenia ocВ casionally present with disseminated intravascular coagulation8 or renal failure and other findings indicative of the hemolytic–uremic syndrome or thrombotic thrombocytopenic purpura.9 2.0 Platelet transfusion 1.5 Petechiae and oral and urinary bleeding 1.0 0.5 0.0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Days Figure 1. Course of Immune Thrombocytopenia in a Patient Treated with Sulfamethoxazole. Trimethoprim–sulfamethoxazole was prescribed for treatment of a urinary tract infection in a 29-year-old woman. On day 7 of treatment, petechiae RETAKE 1st AUTHOR: Aster ICM and ecchymoses, buccal hemorrhage, and gross urinary bleeding developed, 2nd FIGURE: 1 of 2 REG F 3rd 4000 per and the antibiotic treatment was stopped. Her platelet count was CASE cubic millimeter. A platelet transfusion given on day 9 Revised had little effect on Line 4-C EMail the platelet count. Sustained occurred during theSIZE next few days. ARTIST: recovery ts H/T H/T 22p3 Enon A strong sulfamethoxazole-dependent, platelet-reactive antibody was detectCombo ed in a blood sample obtained on day 9 and was still present after 3 months AUTHOR, PLEASE NOTE: and after 5 years. Figure No trimethoprim-dependent antibodies were detected. has been redrawn and type has been reset. Please check carefully. JOB: 356xx ISSUE: 08-02-07 have been implicated.2,12,13 Many of the drugs that are common triggers for this disorder also cause sensitivity reactions involving the skin and other organs.14 George and colleagues critically analyzed reports of drug-induced thrombocytopenia published through 200513,15 and identified 85 medications for which a cause-and-effect relationship was considered to be “definite” (58 agents) or “probable” (27 agents) on the basis of clinical criteria (Table 2).13 (A compendium of implicated drugs and case reports updated through August 2004 is available at http://moon.ouhsc.edu/jgeorge/ DITP.html.) In the analysis by George et al., no weight was given to laboratory demonstration of drug-dependent antibodies. As improved techniques are developed, serologic testing may become increasingly useful for identifying the specific cause of thrombocytopenia in individual cases — albeit after the fact. C aus at i v e Agen t s Rare but convincing examples of drug-induced Many of the drugs shown in multiple studies to thrombocytopenia induced by herbal remedies16,17 be capable of causing drug-induced thrombocy- and foods18 have been described, and there are topenia are listed in Table 1, but at least 100 others numerous reports of acute, severe thrombocyton engl j med 357;6  www.nejm.org  august 9, 2007 581 The n e w e ng l a n d j o u r na l of m e dic i n e Table 1. Drugs Commonly Implicated as Triggers of Drug-Induced Thrombocytopenia.* Drug Category Drugs Implicated in Five or More Reports Heparins Unfractionated heparin, low-molecular-weight heparin Other Drugs Cinchona alkaloids Quinine, quinidine Platelet inhibitors Abciximab, eptifibatide, tirofiban Antirheumatic agents Gold salts Antimicrobial agents Linezolid, rifampin, sulfonamides, vancomycin Sedatives and anticonvulsant agents Carbamazepine, phenytoin, valproic acid Diazepam Histamine-receptor antagonists Cimetidine Ranitidine Analgesic agents Acetaminophen, diclofenac, naproxen Ibuprofen Diuretic agents Chlorothiazide Hydrochlorothiazide Chemotherapeutic and immunoВ suppressant agents Fludarabine, oxaliplatin Cyclosporine, rituximab D-penicillamine *For a more extensive list, see Aster,2 Warkentin,12 and George et al.13 and the University of Oklahoma Web site (http:// moon.ouhsc.edu/jgeorge/DITP.html). Table 2. Criteria and Level of Evidence for Establishing a Causative Relationship in Drug-Induced Thrombocytopenic Purpura.* Criterion and Level of Evidence Description Criterion 1 Therapy with the candidate drug preceded thrombocytopenia, and recovery from thrombocytopenia was complete and sustained after discontinuation of therapy. 2 The candidate drug was the only drug used before the onset of thrombocytopenia, or other drugs were continued or reintroduced after discontinuation of therapy with the candidate drug, with a sustained normal platelet count. 3 Other causes of thrombocytopenia were ruled out. 4 Re-exposure to the candidate drug resulted in recurrent thrombocytopenia. Level of evidence I Definite — criteria 1, 2, 3, and 4 are met. II Probable — criteria 1, 2, and 3 are met. III Possible — criterion 1 is met. IV Unlikely — criterion 1 is not met. *The information is adapted from George et al.13 penia after injection of iodinated contrast medium for radiographic studies.12,13 Whether immune mechanisms are involved is unknown. Severe thrombocytopenia and other signs and symptoms of thrombotic thrombocytopenic purpura develop in approximately 1 of every 2500 patients treated with the platelet inhibitor ticlopidine and a much smaller fraction of those given the closely related drug clopidogrel, usually after 1 to 2 weeks of treatment.19 The responsible mechanisms have not yet been defined. Acute, 582 severe, usually self-limited thrombocytopenia has been described in patients treated with recently developed monoclonal antibodies such as infliximab (anti–tumor necrosis factor-О± antibody), efalizumab (anti-CD11a antibody), and rituximab (anti-CD20 antibody).2 No causative mechanism has yet been identified. Certain drugs, such as the antiepileptic agent valproate,20 the cardiac agent amrinone,21 and the antibiotic linezolid,22 induce low-grade thrombocytopenia in up to 30% of patients receiving long- n engl j med 357;6  www.nejm.org  august 9, 2007 current concepts term treatment; the mechanisms of action may be nonimmune but are poorly understood. The decrease in platelets is rarely severe enough to require treatment. Although chemotherapeutic and immunosuppressive agents typically cause thrombocytopenia by suppressing hematopoiesis, they can also cause immune thrombocytopenia.23 Drug-induced thrombocytopenia should be suspected, therefore, in patients treated with such drugs if there is an acute drop in the platelet level after exposure. Immune thrombocytopenia caused by vancomycin is probably more common than is generally recognized, and it is easily overlooked in seriousВ ly ill patients because the low platelet count can be attributed to other causes.24 In rare cases, the quinine in tonic water or an aperitif causes immune thrombocytopenia (“cocktail purpura”).25 Patho gene sis Drug-induced thrombocytopenia, like other idiosyncratic drug-sensitivity reactions, affects only a small fraction of patients taking medications that can trigger the disorder. No predisposing genetic or environmental factors have been identified, and no suitable animal models are available. Mechanisms by which drugs are thought to cause immune thrombocytopenia are summarized in Table 3. Thrombocytopenia Induced by Quinine and Other Drugs The hallmark of thrombocytopenia induced by quinine and many other drugs is a remarkable antibody that binds tightly to normal platelets only in the presence of the sensitizing drug. The epitopes targeted by these antibodies usually reside on glycoprotein IIb/IIIa or Ib/V/IX complexes, the major platelet receptors for fibrinogen and von Willebrand factor, respectively.26,27 Small molecules, like drugs, are thought to be immunogenic only when linked covalently to a large carrier molecule, usually a protein. Antibodies induced by drug–protein adducts are largely specific for the drug (or the small molecule, called the hapten), although some antibodies recognize the drug and its carrier molecule.28 Accordingly, early investigators assumed that drug-dependent antibodies found in patients with drug-induced thrombocytopenia were hapten-specific (or drugspecific). This may be true of antibodies that cause hemolytic anemia in patients treated with massive doses of penicillin29 and perhaps some of those that cause thrombocytopenia in patients given penicillin-like drugs.30 However, serologic studies in patients with drug-induced thrombocytopenia caused by other drugs failed to support this concept.31 An alternative hypothesis was that the drug reacts directly with the antibody to produce immune complexes that somehow target Table 3. Mechanisms Underlying Drug-Induced Immune Thrombocytopenia.* Classification Mechanism Incidence Examples of Drugs Hapten-dependent Hapten links covalently to membrane protein Very rare antibody and induces drug-specific immune response Penicillin, possibly some cephalosporin antibiotics Quinine-type drug Drug induces antibody that binds to membrane 26 cases per 1 million users of В uinine per week, probably q protein in presence of soluble drug Вfewer cases with other drugs Quinine, sulfonamide antibiotics, nonsteroidal antiinflammatory drugs Fiban-type drug Drug reacts with glycoprotein IIb/IIIa to induce 0.2–0.5% a conformational change (neoepitope) recognized by antibody (not yet confirmed) Tirofiban, eptifibatide Drug-specific antibody Antibody recognizes murine component of Вchimeric Fab fragment specific for platelet membrane glycoprotein IIIa Abciximab Autoantibody Drug induces antibody that reacts with autolo- 1.0% with gold, very rare with progous platelets in absence of drug cainamide and other drugs Immune complex Drug binds to platelet factor 4, producing im- 3–6% among patients treated with Heparins mune complex for which antibody is specific; unfractionated heparin for 7 days, immune complex activates platelets through rare with low-molecular-weight Fc receptors heparin 0.5–1.0% after first exposure, 10–14% after second exposure Gold salts, procainamide *The information is adapted from Aster.2 n engl j med 357;6  www.nejm.org  august 9, 2007 583 The n e w e ng l a n d j o u r na l platelets and cause their destruction.31 However, these hypothetical drug–antibody complexes were never demonstrated experimentally, and it was later found that drug-dependent antibodies, like other antibodies, react with platelets through their Fab domains rather than through their Fc domains, as would be expected of immune complexes.32,33 Other possibilities considered were that the drug reacts with the target protein to produce a compound epitope (part drug, part proВ tein) for which the antibody is specific34,35 and that the drug induces a conformational change in the protein, creating a new target epitope elsewhere in the molecule.2,36 A recently proposed model aimed at reconciling several of these hypotheses37 suggests that drug-dependent antibodies are derived from a pool of naturally occurring antibodies with weak affinity for self antigens,38 residing in this case on certain platelet membrane glycoproteins. According to this model, the interaction between these low-affinity antibodies and their target antigens is too weak to affect blood cells under normal circumstances. However, certain drugs affect both antibody and antigen in such a way that the strength of the interaction is greatly increased (Fig. 2). When a B cell expressing such an antibody is induced to proliferate and undergo affinity maturation in a patient taking the medication, the resulting antibody can destroy the targeted blood cell if the drug is present.37 This model suggests that whether the drug binds first to the antibody or to the targeted membrane protein depends simply on its relative affinity for one component or the other. Thrombocytopenia Induced by Platelet Inhibitors Acute thrombocytopenia, usually mild but occasionally life-threatening, is a common complication of treatment with the platelet inhibitors tirofiban and eptifibatide, which are widely used to prevent restenosis after coronary angioplasty.7 These ligand-mimetic drugs (“fibans”) inhibit thrombosis by binding to a specific site on the platelet О±IIb/ОІ3 integrin (glycoprotein IIb/IIIa) and competitively inhibiting platelet–fibrinogen interaction.7 Antibodies causing thrombocytopenia in patients given these agents probably recognize structural changes (neoepitopes) induced in the О±IIb/ОІ3 integrin when a fiban binds to it, but this theory has not been formally proved. Curiously, 584 of m e dic i n e these antibodies can occur naturally, creating the possibility that thrombocytopenia will arise within a few hours after the patient’s first exposure to the drug.7 Thrombocytopenia Induced by Abciximab Abciximab is a widely used chimeric (human– mouse) Fab fragment that is specific for ОІ3 integrin (glycoprotein IIIa). Like the fibans, it blocks platelet–fibrinogen interaction. Abciximab itself does not cause thrombocytopenia because it lacks the Fc domain required for recognition of antibody-coated platelets by phagocytes. However, in about 1% of patients given abciximab for the first time, and in more than 10% of those treated a second time, acute thrombocytopenia develops within a few hours of starting an infusion.39 In some patients the onset of thrombocytopenia is delayed until 5 to 8 days after the initial 24- to 48-hour period of exposure to the drug.40 AbcixiВ mab-induced thrombocytopenia is often mild, but fatalities have been recorded.41,42 Acute thrombocytopenia after first exposure to abciximab appears to be caused by preexisting antibodies specific for murine structural elements in the abciximab molecule.40,42 Antibodies that cause delayed thrombocytopenia are newly induced but recognize the same target; they cause thrombocytopenia because abciximab-coated platelets are still present in the circulation 10 to 14 days after treatment.40 Thrombocytopenia Due to Drug-Induced Autoantibodies In rare cases, drugs induce true autoantibodies that are capable of destroying platelets in the absence of the sensitizing agent.43 About 1% of patients treated with gold salts for rheumatoid arthritis have this complication.44 Autoantibodies induced by gold may be unique in having specificity for platelet membrane glycoprotein V.45 Other drugs that are probably capable of inducing autoimmune thrombocytopenia include procainamide, sulfonamide antibiotics, and interferons alfa and beta.2,12,13,43 Acute, sometimes severe, but usualВ ly transient thrombocytopenia can occur several weeks after the vaccination of children or adults for various infectious diseases, but it is rare.46,47 This condition resembles acute idiopathic thrombocytopena, which sometimes develops in children after a viral infection, but its cause has not been established. n engl j med 357;6  www.nejm.org  august 9, 2007 current concepts H Drug-dependent antibody CDR Drug Drug-dependent antibody CDR H + H + + + + + Platelet antigen Platelet antigen Low-affinity fit High-affinity fit Figure 2. Model for the Binding of a Drug-Dependent Antibody to an Epitope on a Platelet Glycoprotein. COLOR FIGURE Antibodies capable of causing drug-dependent thrombocytopenia react weakly with an epitope on a target glycoprotein. The binding affinity Draft 5 06/15/07 (K A) for this interaction is too low to allow a sufficient number of antibody molecules to bind in the absence of the drug (“low-affinity Author Aster fit”). The drug contains structural elements that are complementary to a negatively charged site on the glycoprotein and a hydrophobic Fig # 2 site (H) on the complementarity-determining region (CDR) of the antibody. The drug interacts with these sites toTitle improve the fit between Drug-dependent antibody binding the two proteins, increasing the K A to a value that permits binding to occur at levels of antibody, antigen, and ME drug achieved in the cirВ Campion DE culation after ingestion of the drug (“high-affinity fit”). Adapted from Bougie et al.37 KMK Artist AUTHOR PLEASE NOTE: Figure has been redrawn and type has been reset Please check carefully Platelet-specific autoimmunity induced by drugs is clinically similar to acute idiopathic autoimmune thrombocytopenia.43 The possibility that drug-induced autoimmune thrombocytopenia is not uncommon remains speculative. Di agnosis Drug-induced thrombocytopenia should be suspected in any patient who presents with acute thrombocytopenia of unknown cause. In considering this diagnosis, the clinician should keep in mind that 5 to 7 days of exposure is usually needed to produce sensitization in a patient given a drug for the first time. As previously noted, platelet inhibitors are exceptions to this general rule. In adults, the presence of severe thrombocytopenia (<20,000 platelets per cubic millimeter) increases the likelihood that a patient has druginduced thrombocytopenia, and it should be strongly suspected in any patient with a history of acute, transient thrombocytopenia. Because patients sometimes do not report exposure to drugs later found to be the responsible agents,1 a detailed, careful history of drug exposure is essential. Patients should be asked specifically about quinine, quinidine, sulfonamides, herbal remedies, folk medicines, common nonprescription drugs such as acetaminophen, and recent vaccinations. 08/02/07 Thrombocytopenia caused by undisclosed drug use has been described.48 In patients with sensitivity to quinine, quinidine, sulfonamides, and many other drugs, it is often possible to identify antibodies that react with normal platelets in the presence of the drug but not in its absence.23,42,49 However, testing is technically demanding and not widely available (except for heparin) and is therefore not useful in the immediate care of a patient. Testing can be helpful in documenting the cause of thrombocytopenia after the fact and, more generally, in determining which drugs can cause drug-induced thrombocytopenia. Unfortunately, in patients with a history that is typical of drug-induced thrombocytopenia, antibody tests may be negative.2,36 One important reason for this is that a drug metabolite produced in vivo can be the sensitizing agent.34,50 The range of drug metabolites capable of inducing drug-induced thrombocytopenia is not well defined, but this type of sensitivity may be more common than has been thought.34,50 If there is a strong suspicion that thrombocytopenia was drug-induced and documentation of drug sensitivity is critical for diagnosis or management, a diagnostic challenge can be considered. Just 1 or 2 mg of a drug can cause a substan- n engl j med 357;6  www.nejm.org  august 9, 2007 Issue date 585 The n e w e ng l a n d j o u r na l tial drop in platelet levels,51 and a conventional dose can cause severe thrombocytopenia and bleeding.52 Therefore, it is important to start with a few milligrams of the drug and to monitor platelet counts closely for 24 hours. Antibodies sometimes become undetectable after a few months, in which case the drug may initially have no effect on the platelet count. T r e atmen t a nd Pro gnosis Many patients with drug-induced thrombocytopenia have only petechial hemorrhages and occasional ecchymoses and require no specific treatment other than discontinuation of the sensitizing medication. When there is uncertainty about the causative drug, all medications should be discontinued, and pharmacologic equivalents with differВ ent chemical structures substituted as necessary. Patients who have severe thrombocytopenia and “wet purpura” should be aggressively treated with References 1. Reddy JC, Shuman MA, Aster RH. Quinine/quinidine-induced thrombocytopenia: a great imitator. Arch Intern Med 2004;164:218-20. 2. Aster R. Drug-induced thrombocytopenia. In: Michelson AD, ed. Platelets. New York: Academic Press, 2007:887-902. 3. Arepally GM, Ortel TL. HeparinВinduced thrombocytopenia. N Engl J Med 2006;355:809-17. 4. Arndt PA, Garratty G. The changing spectrum of drug-induced immune hemolytic anemia. Semin Hematol 2005;42: 137-44. 5. Stroncek DF. Drug-induced immune neutropenia. Transfus Med Rev 1993;7:26874. 6. Vipan W. Quinine as a cause of purpura. Lancet 1865;2:37. 7. Aster RH. Immune thrombocytopenia caused by glycoprotein IIb/IIIa inhibitors. Chest 2005;127:Suppl 2:53S-59S. 8. Knower MT, Bowton DL, Owen J, Dunagan DP. Quinine-induced disseminated intravascular coagulation: case report and review of the literature. Intensive Care Med 2003;29:1007-11. 9. Kojouri K, Vesely SK, George JN. Quinine-associated thrombotic thrombocytopenic purpura–hemolytic uremic syndrome: frequency, clinical features, and long-term outcomes. Ann Intern Med 2001;135:104751. 10. van den Bemt PM, Meyboom RH, Egberts AC. Drug-induced immune thrombocytopenia. Drug Saf 2004;27:1243-52. 11. Kaufman DW, Kelly JP, Johannes CB, 586 of m e dic i n e platelet transfusions because of the risk of fatal intracranial or intrapulmonary hemorrhage.2,53,54 Corticosteroids are often given, but there is no evidence that they are helpful if the thrombocytopenia is drug-induced. Intravenous immune globulin55 and plasma exchange56 have been used in acutely ill patients, but the benefit of these treatments is uncertain.2 Once established, drug sensitivity probably perВ sists indefinitely. Therefore, patients should be advised to avoid permanently the medication thought to be the cause of thrombocytopenia. Fortunately, drug-induced antibodies tend to be specific for the sensitizing drug,57 and patients usually tolerate pharmacologic equivalents, even those with quite similar structures. Supported by grants from the National Heart, Lung, and Blood Institute (HL-13629 and HL-44612) and the Northland affiliate of the American Heart Association (0235419Z). No potential conflict of interest relevant to this article was reported. et al. Acute thrombocytopenic purpura in relation to the use of drugs. Blood 1993; 82:2714-8. 12. Warkentin TE. Thrombocytopenia due to platelet destruction and hypersplenism. In: Hoffman R, Benz EJ Jr, Shattil SJ, et al., eds. Hematology: basic principles and pracВ tice. 4th ed. Philadelphia: Elsevier, 2005: 2305-25. 13. George JN, Raskob GE, Shah SR, et al. Drug-induced thrombocytopenia: a systematic review of published case reports. Ann Intern Med 1998;129:886-90. 14. Roujeau JC, Kelly JP, Naldi L, et al. Medication use and the risk of Stevens– Johnson syndrome or toxic epidermal necrolysis. N Engl J Med 1995;333:16007. 15. Li X, Hunt L, Vesely SK. Drug-induced thrombocytopenia: an updated systematic review. Ann Intern Med 2005;142:474-5. 16. Arnold J, Ouwehand WH, Smith GA, Cohen H. A young woman with petechiae. Lancet 1998;352:618. 17. Azuno Y, Yaga K, Sasayama T, Kimoto K. Thrombocytopenia induced by Jui, a traditional Chinese herbal medicine. Lancet 1999;354:304-5. 18. Lavy R. Thrombocytopenic purpura due to lupinus termis bean. J Allergy Clin Immunol 1964;35:386-9. 19. Bennett CL, Connors JM, Carwile JM, et al. Thrombotic thrombocytopenic purpura associated with clopidogrel. N Engl J Med 2000;342:1773-7. 20. Trannel TJ, Ahmed I, Goebert D. Occurrence of thrombocytopenia in psychi- atric patients taking valproate. Am J Psychiatry 2001;158:128-30. 21. Ross MP, Allen-Webb EM, Pappas JB, McGough EC. Amrinone-associated thromВ bocytopenia: pharmacokinetic analysis. Clin Pharmacol Ther 1993;53:661-7. 22. Attassi K, Hershberger E, Alam R, Zervos MJ. Thrombocytopenia associated with linezolid therapy. Clin Infect Dis 2002;34:695-8. 23. Curtis BR, Kaliszewski J, Marques MB, et al. Immune-mediated thrombocytopenia resulting from sensitivity to oxaliplatin. Am J Hematol 2006;81:193-8. 24. Von Drygalski A, Curtis BR, Bougie DW, et al. Vancomycin-induced immune thrombocytopenia. N Engl J Med 2007; 356:904-10. 25. Belkin GA. Cocktail purpura: an unusual case of quinine sensitivity. Ann Intern Med 1967;66:583-6. 26. Visentin GP, Newman PJ, Aster RH. Characteristics of quinine- and quinidineinduced antibodies specific for platelet glycoproteins IIb and IIIa. Blood 1991;77: 2668-76. 27. Asvadi P, Ahmadi Z, Chong BH. Druginduced thrombocytopenia: localization of the binding site of GPIX-specific quininedependent antibodies. Blood 2003;102: 1670-7. 28. Parker CW. Hapten immunology and allergic reactions in humans. Arthritis Rheum 1981;24:1024-36. 29. Garratty G. Immune cytopenia associated with antibiotics. Transfus Med Rev 1993;7:255-67. n engl j med 357;6  www.nejm.org  august 9, 2007 current concepts 30. Salamon DJ, Nusbacher J, Stroupe T, Wilson JH, Hanrahan JB. Red cell and platelet-bound IgG penicillin antibodies in a patient with thrombocytopenia. Transfusion 1984;24:395-8. 31. Shulman NR. A mechanism of cell destruction in individuals sensitized to foreign antigens and its implications in auto-immunity: combined Clinical Staff Conference at the National Institutes of Health. Ann Intern Med 1964;60:506-21. 32. Christie DJ, Mullen PC, Aster RH. Fab-mediated binding of drug-dependent antibodies to platelets in quinidine- and quinine-induced thrombocytopenia. J Clin Invest 1985;75:310-4. 33. Smith ME, Reid DM, Jones CE, Jordan JV, Kautz CA, Shulman NR. Binding of quinine- and quinidine-dependent drug antibodies to platelets is mediated by the Fab domain of the immunoglobulin G and is not Fc dependent. J Clin Invest 1987;79: 912-7. 34. Mueller-Eckhardt C, Salama A. Druginduced immune cytopenias: a unifying pathogenetic concept with special emphasis on the role of drug metabolites. Transfus Med Rev 1990;4:69-77. 35. Shulman NR, Reid DM. Mechanisms of drug-induced immunologically mediated cytopenias. Transfus Med Rev 1993;7: 215-29. 36. Aster RH. Drug-induced immune cytopenias. Toxicology 2005;209:149-53. 37. Bougie DW, Wilker PR, Aster RH. Patients with quinine-induced immune thrombocytopenia have both “drug-depenВ dent” and “drug-specific” antibodies. Blood 2006;108:922-7. 38. Pillai S. Two lymphoid roads diverge — but does antigen bade B cells to take the road less traveled? Immunity 2005;23: 242-4. 39. Tcheng JE, Kereiakes DJ, Lincoff AM, et al. Abciximab readministration: results of the ReoPro Readministration Registry. Circulation 2001;104:870-5. 40. Curtis BR, Divgi A, Garritty M, Aster RH. Delayed thrombocytopenia after treatment with abciximab: a distinct clinical entity associated with the immune response to the drug. J Thromb Haemost 2004;2:985-92. 41. McCorry RB, Johnston P. Fatal delayed thrombocytopenia following abciximab therapy. J Invasive Cardiol 2006;18: E173-E174. 42. Curtis BR, Swyers J, Divgi A, McFarland JG, Aster RH. Thrombocytopenia after second exposure to abciximab is caused by antibodies that recognize abciximab-coated platelets. Blood 2002;99: 2054-9. 43. Aster RH. Can drugs cause autoimmune thrombocytopenic purpura? Semin Hematol 2000;37:229-38. 44. von dem Borne AE, Pegels JG, van der Stadt RJ, van der Plas-van Dalen CM, Helmerhorst FM. Thrombocytopenia associated with gold therapy: a drug-induced autoimmune disease? Br J Haematol 1986; 63:509-16. 45. Garner SF, Campbell K, Metcalfe P, et al. Glycoprotein V: the predominant target antigen in gold-induced autoimmune thrombocytopenia. Blood 2002;100: 344-6. 46. Neau D, Bonnet F, Michaud M, et al. Immune thrombocytopenic purpura after recombinant hepatitis B vaccine: retrospective study of seven cases. Scand J Infect Dis 1998;30:115-8. 47. Nieminen U, Peltola H, Syrjala MT, Makipernaa A, Kekomaki R. Acute thrombocytopenic purpura following measles, mumps and rubella vaccination: a report on 23 patients. Acta Paediatr 1993;82:26770. 48. Reid DM, Shulman NR. Drug purpura due to surreptitious quinidine intake. Ann Intern Med 1988;108:206-8. 49. Bougie DW, Wilker PR, Wuitschick ED, et al. Acute thrombocytopenia after treatment with tirofiban or eptifibatide is assoВ ciated with antibodies specific for ligandoccupied GPIIb/IIIa. Blood 2002;100: 2071-6. 50. Bougie D, Aster R. Immune thrombocytopenia resulting from sensitivity to metabolites of naproxen and acetaminophen. Blood 2001;97:3846-50. 51. Shulman NR. Immunoreactions involvВ ing platelets. IV. Studies on the pathogenesis of thrombocytopenia in drug purpura using test doses of quinidine in sensitized individuals; their implications in idiopathic thrombocytopenic purpura. J Exp Med 1958;107:711-29. 52. Schmitt SK, Tomford JW. Quinineinduced pancytopenia and coagulopathy. Ann Intern Med 1994;120:90-1. 53. Freiman JP. Fatal quinine-induced thrombocytopenia. Ann Intern Med 1990; 112:308-9. 54. Fireman Z, Yust I, Abramov AL. Lethal occult pulmonary hemorrhage in druginduced thrombocytopenia. Chest 1981; 79:358-9. 55. Ray JB, Brereton WF, Nullet FR. Intravenous immune globulin for the treatment of presumed quinidine-induced thrombocytopenia. DICP 1990;24:693-5. 56. Pourrat O. Treatment of drug-related diseases by plasma exchanges. Ann Med Interne (Paris) 1994;145:357-60. 57. Christie DJ, Weber RW, Mullen PC, Cook JM, Aster RH. Structural features of the quinidine and quinine molecules necessary for binding of drug-induced antibodies to human platelets. J Lab Clin Med 1984;104:730-40. Copyright В© 2007 Massachusetts Medical Society. images in clinical medicine The Journal welcomes consideration of new submissions for Images in Clinical Medicine. Instructions for authors and procedures for submissions can be found on the Journal’s Web site at www.nejm.org. At the discretion of the editor, images that are accepted for publication may appear in the print version of the Journal, the electronic version, or both. n engl j med 357;6  www.nejm.org  august 9, 2007 587 The n e w e ng l a n d j o u r na l of m e dic i n e images in clinical medicine Intravesical Foreign Body A B C D Nicola Mondaini, M.D. Riccardo Bartoletti, M.D. University of Florence Florence, Italy mondatre@hotmail.com A  n 82-year-old woman presented with abdominal colic. she had a 20-year history of type 2 diabetes and a 2-year history of recurrent urinary RETAKE 1st Mondaini ICM tractAUTHOR infections despite many courses of antimicrobial therapy. She lived in a 2nd REG F FIGURE 1a-d 3rd long-term care facility. An abdominal radiograph showed a large stone in her bladder, CASE TITLE with EMail a foreign body in theLine center4-C of theRevised stone (Panel A). On cystotomy (Panel B), an SIZE Enon bladder ARTIST:stone mleahy measuring infected 6 by 2 by 0.5 cm was removed (Panel C), and a pen H/T H/T 39p6 FILL Combo cap was found at the center (Panel D). The patient was discharged 2 days later and AUTHOR, PLEASE NOTE: had a complete recovery. hashas had noreset. further urinary tract infections. The patient Figure has been redrawnShe and type been did not know howPlease thecheck cap carefully. made its way into her bladder. A foreign body should be considered in a patient with persistent urinary tract problems, especially if the patient JOB: 35706 ISSUE: 8-09-07 is frail. Copyright В© 2007 Massachusetts Medical Society. 588 n engl j med 357;6  www.nejm.org  august 9, 2007 The n e w e ng l a n d j o u r na l of m e dic i n e case records of the massachusetts general hospital Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate Editor Jo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate Editor Sally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor Case 24-2007: A 20-Year-Old Pregnant Woman with Altered Mental Status Andrew J. Cole, M.D., John W. Henson, M.D., Michael H.A. Roehrl, M.D., Ph.D., and Matthew P. Frosch, M.D., Ph.D. Pr e sen tat ion of C a se A 20-year-old pregnant woman was admitted to this hospital at 26 weeks of gestation because of dizziness, confusion, and difficulty walking. Ten weeks before admission, the patient had a positive result on a home pregnancy test and presented to a neighborhood health center for prenatal screening. Tests for sickle cell trait, syphilis, and human immunodeficiency virus (HIV) and hepatitis B and C virus antibodies were negative. Serologic tests for varicella–zoster virus and rubella IgG were positive. Two weeks later, an endocervical specimen was positive for Chlamydia trachomatis infection and negative for gonorrhea. The patient missed follow-up appointments, and treatment with azithromycin was initiated 4 weeks later. Six weeks before admission, she moved into a shelter for pregnant women. Staff members described her as happy, with a childlike affect, a poor memory, confusion, and odd movements of her head. During the next 2 weeks, nausea and vomiting occurred daily and were controlled with metoclopramide. Four days before admission, dizziness and weakness on the left side developed; she began to fall to her left and vomited several times. The next day, she went to the emergency department of another hospital. On evaluation, the patient was oriented to location but not to date, day, or month, and she provided inconsistent information about her medical history. The uterus was gravid, and the remainder of the physical examination was normal. An electrocardiogram revealed sinus tachycardia and counterclockwise rotation with T waves in the right precordial leads. Urinalysis showed a protein level of 30 mg per deciliter and a glucose level of 100 mg per deciliter (5.6 mmol per liter). Tricyclic metabolites were present on toxicology screening of a urine specimen. Computed tomographic (CT) scanning of the head revealed a slight, diffuse prominence of the ventricular system. There was no intracranial mass or other focal brain lesion. On the second hospital day, the patient was alert, calm, cooperative, and oriented to person, location, and current events but was not aware of details of her life. There were no tremors or extrapyramidal signs. Ultrasonographic examination revealed normal fetal anatomy and growth, corresponding to a gestation of 25 weeks 6 days. On the third day, the weakness, nausea, and vomiting had resolved, n engl j med 357;6  www.nejm.org  august 9, 2007 From the Neurology Service (A.J.C., J.W.H., M.P.F.) and the Departments of RadiolВ ogy (J.W.H.) and Pathology (M.H.A.R., M.P.F.), Massachusetts General Hospital; and the Departments of Neurology (A.J.C., J.W.H.) and Pathology (M.H.A.R., M.P.F.), Harvard Medical School. N Engl J Med 2007;357:589-600. Copyright В© 2007 Massachusetts Medical Society. 589 The n e w e ng l a n d j o u r na l and the patient was thought to have returned to her baseline mental status. She was discharged to the shelter with a recommendation to schedule a follow-up neurologic evaluation. At the shelter, she was dizzy, had difficulty walking, and fell into a chair. That evening, she was brought to the emergency department of this hospital. In the emergency department, the patient reported feeling “woozy” and nauseated. She noted a mild headache of gradual onset, extending bandВ like across the brow. The history as given by the patient was inconsistent; the history was then provided by staff members of the shelter, and many details were lacking. The patient was a native of Cape Verde who had immigrated to this country 3 years previously. She had had measles at 4 months of age and varicella infection in childВ hood. At 7 years of age, she injured her head in a fall but was said to have recovered fully. ImmuВ nizations included polio vaccine and diphtheria, pertussis, and tetanus vaccine series; measles vaccine (at 11 months of age); measles, mumps, and rubella vaccine combination; and hepatitis B vaccine (between 2 and 3 years before admission, on enrollment in high school). The patient had attended school through the 10th grade and was unemployed. During the 3 years before admission, she had lived with relatives, friends, and a boyfriend, as well as in shelters. She was single, and she no longer maintained a social relationship with the father of the fetus. Her parents and seven siblings were alive but not in contact with her at the time of admission. No family medical history was available. She had no known allergies and did not use alcohol, illicit drugs, or tobacco. On examination in the emergency department, the patient was alert but somewhat uncooperative, with involuntary head movements. Her mental status was not formally assessed, but her level of cognitive function was said by a friend to be at baseline. The blood pressure was 107/81 mm Hg, the pulse 84 beats per minute, and the temperature 36.3В°C; the respirations were 18 per minute, and the oxygen saturation was 100% while the paВ tient was breathing ambient air. Acneiform lesions were present on her face. The abdomen was soft, gravid, and not tender; the fetus appeared to be healthy. The 1st cranial nerve was not tested, and the 2nd through 12th nerves were intact. Strength was intact, and the gait was unsteady. The remainВ der of the examination was normal. 590 of m e dic i n e Results of laboratory tests are shown in Table 1. After premedication with lorazepam at a dose of 1 mg to control involuntary movements, magnetВ ic resonance imaging (MRI) of the brain was performed without administration of contrast material. On T2-weighted, fluid-attenuated inverВ sion recovery (FLAIR) images, hyperintense signal was seen in the left hippocampus and parahippoВ campal gyrus as well as in the posterior limb of the left internal capsule. There was no evidence of restricted diffusion. Examination by a neurology consultant showed that the patient was oriented to person and place, with a childlike affect. Her speech was fluent, and naming was intact. She could read a short sentence and do simple addition. She was lefthanded, could write her name but not a sentence, and followed simple and complex commands. Her attention was variable, and testing of her memory showed recollection of zero of three items at 5 minutes on repeated examination. There was mild asymmetry of the face with flattening of the right nasolabial fold. Smell and taste were not tested. The function of the other cranial nerves was intact. There were choreiform movements of the head and neck, poor performance of rapid alternating movements, and apraxВ ia. Hypertonia and hyperreflexia with clonus were noted in the right leg. The gait was wide-based, with postural instability and leaning toward the left. She was unable to stand on one foot. She was admitted to the neurology service. On the second hospital day, a lumbar puncture was performed. Results of cerebrospinal fluid analysis are shown in Table 2; other test results are listed in Table 1. An enzyme-linked imВ munosorbent assay for serum antibodies against HIV was negative. An electroencephalogram showed diffuse theta slowing and frontal intermittent rhythmic delta activity, which was more prominent in the right hemisphere than in the left. There was no epileptiform activity (Fig. 1). Repeated MRI of the brain after the administration of gadolinium showed no changes and no evidence of abnormal enhancement. Acyclovir was administered intravenously. The next day, a serum Lyme antibody test, a test of a throat swab for Mycoplasma pneumoniae nucleic acid, and cultures of blood and urine were negative; results of other tests are listed in Table 1. On the fifth day, the patient’s condition appeared to be improved. She was oriented and remembered details of her past; dysmetria and truncal n engl j med 357;6  www.nejm.org  august 9, 2007 case records of the massachuset ts gener al hospital ataxia were reduced. Results on a repeated elecВ troencephalogram were unchanged. The next day, a repeated lumbar puncture was performed (Table 2). Between the 7th and 18th hospital days, the patient’s motor function gradually worsened, right-sided neglect developed, she became unable to feed herself, her responsiveness and ability to follow commands decreased, and she became incontinent. She began lying in a fetal position, moaning and crying out unintelligible sounds. A skin test for tuberculosis, a test of a nasopharyngeal specimen for respiratory viral antigens, and a viral culture of a stool specimen were negative. Nucleic acid testing for HIV RNA and tests for antinuclear antibodies were negative. Levels of free and total thyroxine were normal, and the thyroglobulin level was elevated (54.7 ng per milliВ liter; normal range, 4 to 40). On the 12th day, the acyclovir was discontinued, and ceftriaxone, at a dose of 2 g, was administered intravenously. A repeated electroencephalographic study showed increased attenuation of background activity and less abundant frontal intermittent rhythmic delta activity. MRI on the 13th day showed new hyperintense signal in the pons and middle cerebellar peduncles with associated restricted diffusion of water on T2-weighted FLAIR images. Restricted diffusion was also noted in the posterior limb of the left internal capsule. There was atrophy in the left medial temporal lobe, with resolution of the abnormal hyperintense signal on FLAIR images. On the 14th day, a third lumbar puncture was performed. On the 18th hospital day, a test result was received. Differ en t i a l Di agnosis Dr. Andrew J. Cole: I was involved in this patient’s care from the time of her admission and am therefore aware of the diagnosis. I will discuss the case as it unfolded in order to illustrate the diagnostic process and therapeutic decision making that took place. The patient lived semi-independently until she became pregnant 27 weeks before admission. Her level of function at that time was unknown, and because of the lack of information, it was not possible to determine either her level of function before her illness or the tempo of her disease. Neurologic differential diagnosis relies primarily on the physical examination for localization of lesions and on the history, especially the nature of onset and pace of progression, to identify the disease process. This patient’s neurologic examination showed abnormal cognitive function indicating dysfunction of the cortical and subcortical gray matter, abnormal motor function indicating dysfunction of the pyramidal motor system, and choreiform movements indicating dysfunction of the extrapyramidal motor systems. This examination also showed a clumsy gait and difficulty performing rapid alternating movements, indicating dysfunction of the cerebellum or its connections. With the limited information about the pace of her disease, we needed to consider inherited, congenital, and acquired diseases that could be acute, subacute, or chronic, with static, episodic, or proВgressive tempos. We had to base our differential diagnosis on the neurologic examination, initial laboratory testing, and electroencephalographic and MRI studies. Cerebrospinal Fluid Examination The results of the cerebrospinal fluid analysis in this patient showed a lymphocytic pleocytosis with few red cells, a mildly elevated protein level, and a normal glucose level. These findings are characteristic of aseptic meningitis. We were thus concerned about viruses, rickettsia, spirochetes, partially treated bacterial infection, a parameninВ geal focus of infection, certain autoimmune illnesses such as systemic lupus erythematosus or BehГ§et’s disease, vasculitides, carcinoma, a reaction to the toxic effects of certain medications such as nonsteroidal antiinflammatory drugs, and chemical meningitis related to the rupture of a cyst. Although they were nonspecific, the cerebrospinal fluid findings provided support for the possibility of acute or subacute infection or inflammatory illness. The presence of an inflammatory response made chronic degenerative diseasВ es such as Huntington’s disease, Wilson’s disease, and systems abiotrophies such as multisystem atrophy unlikely. Electroencephalographic Studies The initial electroencephalogram was markedly abnormal, but the findings were nonspecific (Fig. 1). The slow and attenuated posterior dominant rhythm suggests cortical gray-matter disease, whereas the intermittent frontal rhythmic delta activity suggests subcortical gray-matter disease. The monomorphic slow waves also suggest that initially the subcortical white matter n engl j med 357;6  www.nejm.org  august 9, 2007 591 The n e w e ng l a n d j o u r na l of m e dic i n e Table 1. Results of Laboratory Tests.* Reference Range for Adults†Variable On Admission Hematocrit (%) 36.0–46.0 (in women) 37.4 Hemoglobin (g/dl) 12.0–16.0 (in women) 13.2 White-cell count (per mm3) 4500–13,000 8,100 On Hospital Day 2 35.2 12.1 7,600 Differential count (%) Neutrophils 40–62 72 Lymphocytes 27–40 21 Monocytes 4–11 6 Eosinophils 0–8 1 Basophils 0–3 0 Platelet count (per mm3) 150,000–350,000 Mean corpuscular volume (Ојm3) 236,000 80–100 Erythrocyte sedimentation rate (mm/hr) Glucose (mg/dl) 192,000 89 1–25 26 70–110 78 73 Sodium (mmol/liter) 135–145 135 137 Potassium (mmol/liter) 3.4–4.8 Chloride (mmol/liter) 100–108 Carbon dioxide (mmol/liter) 23.0–31.9 26.0 25.2 8–25 8 4 0.6–1.5 0.5 0.6 0.0–1.0 0.1 0–0.4 0.0 Total 6.0–8.3 7.7 Albumin 3.3–5.0 3.5 Globulin 2.6–4.1 4.2 Phosphorus (mg/dl) 2.6–4.5 3.0 Magnesium (mmol/liter) 0.7–1.0 0.75 Calcium (mg/dl) 8.5–10.5 9.2 Urea nitrogen (mg/dl) Creatinine (mg/dl) 3.5 106 3.4 104 Bilirubin (mg/dl) Total Direct Protein (g/dl) Creatine kinase (U/liter) 40–150 (in women) Alkaline phosphatase (U/liter) 62 30–100 96 Aspartate aminotransferase (U/liter) 9–32 18 Alanine aminotransferase (U/liter) 7–30 15 Lipase (U/dl) 1.3–6.0 Amylase (U/liter) 3–100 7.5 79 Rapid plasma reagin Nonreactive Human chorionic gonadotropin, quantitative (IU/liter) <6 (in nonpregnant women); 6–15 (borderline) Toxicology screen 32,907 Negative Partial-thromboplastin time lupus anticoagulant Anticardiolipin IgG antibodies (GPL units) 592 7.4 None 0–15 n engl j med 357;6  www.nejm.org  august 9, 2007 7.9 case records of the massachuset ts gener al hospital Table 1. (Continued.) Reference Range for Adults†Variable Anticardiolipin IgM antibodies (MPL units) On Admission 0–15 On Hospital Day 2 10.6 Ceruloplasmin (mg/dl) 27–50 84 Iron (Вµg/dl) 30–160 61 228–428 464 Iron-binding capacity (Вµg/dl) Vitamin B12 (pg/ml) >250 Ferritin (ng/ml) Transferrin (mg/dl) Antistreptolysin O (IU/ml) 10–200 9 188–341 361 <200 0.40–5.00 Thyrotropin (ВµU/ml) 430 208 0.2 Serum protein electrophoresis (mg/dl) IgA 69–309 109 IgG 614–1295 1490 IgM 53–334 93 Herpes simplex virus type 1 antibody IgG Positive (>6.00) Herpes simplex virus type 2 antibody IgG Negative *To convert the values for glucose to millimoles per liter, multiply by 0.05551. To convert the values for urea nitrogen to millimoles per liter, multiply by 0.357. To convert the values for creatinine to micromoles per liter, multiply by 88.4. To convert the values for total and direct bilirubin to micromoles per liter, multiply by 17.1. To convert the values for phosphorus to millimoles per liter, multiply by 0.3229. To convert the values for magnesium to milliequivalents per Вliter, multiply by 2. To convert the values for calcium to millimoles per liter, multiply by 0.250. To convert the values for iron and iron-binding capacity to micromoles per liter, multiply by 0.1791. To convert the values for vitamin B12 to picomoles per liter, multiply by 0.7378. †Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Massachusetts General Hospital are for adults who are not pregnant and do not have medical Вconditions that could affect the results. The ranges therefore may not be appropriate for all patients. was relatively spared. Dr. Henson, may we review the radiologic studies? Dr. John W. Henson: Axial T2-weighted FLAIR images from the MRI studies of the brain on the day of admission, performed without the administration of gadolinium, revealed a region of hyperintense signal in the left medial temporal lobe (Fig. 2A) and subtle increased signal in the posterior limb of the left internal capsule corresponding to the location of the corticospinal tract. These foci did not show restricted diffusion or abnormal enhancement on a gadoliniumenhanced study performed the next day. The appearance of the pons was unremarkable, and no other clinically significant findings were noted. Magnetic resonance venography of the head was normal. By day 13, there had been marked changes. There was a region of abnormal signal in the pons (Fig. 2B), with areas of restricted diffusion on the diffusion-weighted image and apparent- diffusion-coefficient maps. The hyperintensity of the left medial temporal lobe had resolved, and there was volume loss in the region of the hippoВ campal formation. There was restricted diffusion in the left corticospinal tract (Fig. 2C); no abnormal enhancement was detected. These findings were interpreted as resulting from a subacute enВ cephalitis caused by an infection or an autoimmune disorder. Dr. Cole: In summary, this patient has a disturbance of cognitive function, pyramidal tract and cerebellar dysfunction, and a choreiform-movement disorder, and both laboratory tests and electroencephalographic and imaging studies suggest an infectious or autoimmune encephalitis. Disorders of Movement Chorea is a hyperkinetic movement disorder that may result from a number of neurologic diseases; it may appear or worsen during pregnancy, a condition known as chorea gravidarum. Most patients n engl j med 357;6  www.nejm.org  august 9, 2007 593 The n e w e ng l a n d j o u r na l of m e dic i n e Table 2. Results of Cerebrospinal Fluid Tests. Test* Normal Range Opening pressure (mm H20) Hospital Day 2 Hospital Day 6 Hospital Day 14 Pink, slightly turbid Slightly pink, clear 17 Appearance Colorless Colorless, slightly turbid Red-cell count (per mm3) Tube 1 None 650 2250 2360 Tube 4 None 28 2438 1100 Tube 1 0–5 40 100 36 Tube 4 0–5 37 46 10 Tube 1 None 0 6 7 Tube 4 None 0 6 4 Tube 1 None 82 80 61 Tube 4 None 88 82 76 Tube 1 None 11 0 18 Tube 4 None 3 0 8 Tube 1 None 7 7 9 Tube 4 None 9 White-cell count (per mm3) Differential count (%) Neutrophils Lymphocytes Reactive lymphocytes Monocytes Other hematic cells (%) 4 Large mononuclear cells with abundant cytoplasm and nucleoli 9 Large mononuclear cells with basophilic cytoplasm and prominent nucleoli Tube 1 None 7 5 Tube 4 None 6 3 Tube 1 None 0 Tube 4 None 2 Unidentified cells (%) Protein (mg/dl)   5–55 66 100 76 Glucose (mg/dl) 50–75 53 73 65 Nonreactive Nonreactive Venereal Disease Research Laboratory test IgG (mg/dl) Albumin (mg/dl) Oligoclonal bands on agarose electrophoresis 0.0–8.0 38.9 11.0–50.9 16.4 None seen in 80 × concentrate Several seen in 63Г— concentrate Gram’s stain No organisms Acid-fast bacilli stain No organisms No organisms Varicella–zoster virus (PCR) None detected None detected Enterovirus RNA (PCR) None detected Cytomegalovirus DNA None detected None detected Epstein–Barr virus DNA None detected None detected 594 No organisms n engl j med 357;6  www.nejm.org  august 9, 2007 No organisms case records of the massachuset ts gener al hospital Table 2. (Continued.) Test Normal Range Hospital Day 2 Human herpes virus type 6 DNA (PCR) Herpes simplex virus (PCR) Hospital Day 6 Hospital Day 14 None detected None detected None detected None detected None detected Mycoplasma pneumoniae (PCR) Encephalitis antibodies Eastern equine encephalitis None detected West Nile virus IgM None detected Cultures Routine No growth Fungal No growth Adenoviral No growth No growth No growth No growth Enteroviral No growth Mycobacterial No growth *PCR denotes polymerase chain reaction. with this condition present during the second trimester with an isolated movement disorder that resolves after delivery. The most common causes are acute rheumatic fever (Sydenham’s chorea) and the antiphospholipid-antibody syndrome. We also considered other illnesses associated with chorea, including systemic lupus erythematosus, HuntingВ ton’s chorea, and Wilson’s disease, although the latter two illnesses were ruled out by the cerebrospinal fluid and other findings. Sydenham’s chorea is a late complication of infection with group A streptococcus; the onset occurs months after acute infection. Most cases occur in childhood, but up to 30% of patients may have recurrent chorea months or years after the initial episode.1 This patient had only a minimally elevated antistreptolysin-antibody titer, with no other evidence of recent streptococcal infection or cardiac disease. The antiphospholipid-antibody syndrome2 may be primary or secondary to systemic lupus erythematosus, and it may beВcome manifest during pregnancy. This patient had no symptoms or signs of systemic lupus, but lupus confined to the central nervous system is well recognized and may worsen during the course of pregnancy. Antiphospholipid-antibody testing and all laboratory studies for lupus were negative. Acute Viral Encephalitis Herpes simplex encephalitis was initially considered as one of the acute infectious encephalitides because of the abnormality detected in the left hippocampus on MRI. Unlike the arboviral encephalitides and West Nile virus encephalitis, which occur in the summer and fall, when mosquitoes are abundant, herpes simplex encephalitis occurs sporadically throughout the year. The negative results on cerebrospinal fluid testing for herpes simplex virus nucleic acid and the lack of response to acyclovir made this diagnosis unlikely. Other common causes of viral encephalitis, including enteroviral and echoviral infections, as well as infection with coxsackievirus, typically proВ Figure 1. Electroencephalogram Obtained on the Second Hospital Day. The electroencephalogram is markedly abnormal, showing modest slowing dominant1st AUTHOR Cole of the posterior RETAKE ICM background rhythm1 of with bursts of frontal intermittent 2nd REG F FIGURE 4 3rd rhythmic activity (arrows), sometimes maximal CASE delta TITLE Revised on the relatively symmetric bilatEMailright and other timesLine 4-C erally. There are no mst epileptiform features and no periodSIZE Enon ARTIST: H/T H/T 16p6 ic discharges. FILL Combo AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. n engl j med 357;6  www.nejm.org  JOB:august 357069, 2007 ISSUE: 7-9-07 595 The n e w e ng l a n d j o u r na l of m e dic i n e Figure 2. Brain Imaging Studies. An axial T2 -weighted FLAIR image (Panel A) obtained on the day of admission showed a region of abnormal, hyperintense signal in the left hippocampus (arrow) and in the posterior limb of the left internal capsule (not shown). On the 13th hospital day, there was a new region of Вhyperintense signal on T2-weighted FLAIR images in the pons and middle cerebellar peduncles (Panel B, arrow) and restricted diffusion in the middle cerebellar peduncle and posterior limb of the internal capsule as shown on the diffusion-weighted images (Panel C, arrow). A Subacute Encephalitides Paraneoplastic Encephalitis Paraneoplastic limbic encephalitis may precede the appearance of a tumor by months or even years. Psychiatric symptoms, memory failure, confusion and drowsiness, disordered respiration, ataxia, and cranial-nerve palsies have been reported. There may be a modest increase in protein in the cerebrospinal fluid, but few cells are detected. This patient’s clinical and cerebrospinal fluid findings were not consistent with paraneoplastic encephalitis. B Postinfectious Encephalitis C duce prominent signs of meningeal irritation, with photophobia, meningismus, nausea, and headAUTHOR Cole signs of focalRETAKE ache,ICMbut only minimal cerebral1stdysREG F which FIGURE may 2a-c ofbe 4 fleeting and are not2nd function, pro3rd CASE TITLE Revised gressive. Serologic tests in this patient ruled out EMail Line 4-C theseEnon agents. SIZE ARTIST: mst H/T H/T 596 16p6 Combo FILL Several infections may be associated with postinfectious encephalitis syndromes, including measles, mumps, and rubella; influenza; Epstein–Barr virus; and varicella–zoster virus. Acute disseminated encephalomyelitis may occur after a variety of viral infections and after the administration of rabies and smallpox vaccines.3 It usually begins with nonspecific symptoms such as fever, headache, stiff neck, vomiting, and anorexia. Neurologic examination may show optic neuritis, ataxia, and focal weakness; seizures and decreased consciousness may develop. This patient did not have a recent history of immunizations or a viral infection or evidence of optic neuritis, and the imaging findings were not typical of acute disseminatВ ed encephalomyelitis. The cerebrospinal fluid findings were an important clue to the diagnosis in this case. Although the protein level in the initial cerebrospinal fluid specimen was modestly elevated, the IgG component was markedly elevated. Dr. Roehrl, would you discuss the analysis and implications of this finding? Dr. Michael H.A. Roehrl: Cerebrospinal fluid levels of total protein, albumin, and IgG obtained on the second hospital day are shown in Table 2. AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. n engl j med 357;6  www.nejm.org  august 9, 2007 Please check carefully. JOB: 35706 ISSUE: 8-9-07 case records of the massachuset ts gener al hospital Agarose-gel electrophoresis of cerebrospinal fluid revealed oligoclonal bands in the gamma region (Fig. 3A). The cerebrospinal fluid to serum mass concentration quotients for albumin and IgG conВcentrations were QAlb = 4.7Г—10 в€’3 and QIgG =  26.1Г—10в€’3, corresponding to an IgG index of 5.6 (normal value, <0.85).4 On the basis of an analysis developed by Reiber,5‑7 this patient’s results (Fig. 3B) indicated markedly increased intrathecal IgG synthesis (intrathecal proВduction fraction, 87.7%) without evidence of clinВically significant blood–brain barrier dysfunction. The mass concentration ratio of IgG to total protein in the cerebrospinal fluid was 58.9%. Dr. Cole: The diseases that can elicit an intrathecal response of this magnitude are syphilis, chronic rubella panencephalitis, and subacute sclerosing panencephalitis.8-11 This patient did not have syphilis, as shown by negative results on serologic testing and a symptom complex that was inconsistent with the disease. Postrubella enВ cephalitis12,13 may affect patients with history of remote or congenital rubella infection and pres- A P A О±1 О±2 ОІ Оі Normal cerebrospinal fluid Patient’s cerebrospinal fluid Lo w (Г—10в€’3) M H ea igh n 80 % 100 60 % 40 % 20 Q Q % B Q 50 3 20 10 QIgG Figure 3. Results of Cerebrospinal Fluid Electrophoresis. Panel A shows the results of agarose-gel electrophoresis of a specimen of the patient’s cerebrospinal fluid collectВ ed on the second hospital day (concentrated to 1/63 of the original volume) and cerebrospinal fluid from a normal control (concentrated to 1/80 of the original volume). P, A, О±1, О±2, ОІ, and Оі denote the electrophoretic preВ albumin, albumin, alpha-1, alpha-2, beta, and gamma regions, respectively. The arrow shows the position of several strong bands in the gamma region, indicating the presence of multiple oligoclonal immunoglobulins. There is also a relative decrease of the level of albumin in the patient’s cerebrospinal fluid. Panel B shows a double-logarithmic graph designed according to the method proposed by Reiber (also called a Reibergram), in which cerebrospinal fluid to serum mass concentration quotients for albumin (QAlb) and IgG (Q IgG) are plotted along the abscissa and ordinate, respectively. Upper limits (Q High) and lower limits (QLow) of normal values are shown as solid lines, with the dotted line indicating mean normal values (QMean). The isopercentiles (dashed lines) correspond to various relative amounts of intrathecal IgG production (20 to 80%). The vertical dashed line denotes the age-adjusted upper limit of QAlb, separating normal function (left) and abnormal function (right) of the blood–brain barrier. The patient (red dot) had markedly increased intrathecal IgG synthesis (intrathecal production fraction, 87.7%) without evidence of significant dysfunction of the blood–brain barrier (zone 4). Zone 1 denotes normal function, zone 2 denotes pure blood–brain barrier dysfunction, and zone 3 denotes a combination of increased intrathecal IgG synthesis and blood–brain barrier dysfunction. 2 5 4 2 1 1 0.5 (Г—10в€’3) 2 5 10 20 50 100 QAIb ents with progressive dementia, ataxia, chorea, RETAKE 1st AUTHOR: Cole ICM degeneration, and seizures. Examination retinal 2nd FIGURE: 3 of 4 REG F of the cerebroВspinal fluid shows pleocytosis and 3rd CASE Revised a moderately elevated protein level, with up to Line 4-C EMail SIZE ts 50% of theARTIST: cerebrospinal fluid protein composed H/T H/T 16p6 Enon of immunoglobulins. TheCombo diagnosis is confirmed AUTHOR, PLEASE NOTE: by a high antirubella-antibody titer in the cereFigure has been redrawn and type has been reset. brospinal fluid. Please check carefully. JOB: 35706Sclerosing Panencephalitis ISSUE: Subacute 08-09-07 Measles causes three distinct diseases of the central nervous system: postinfectious encephalomyelitis, subacute measles encephalitis, and subВacute sclerosing panencephalitis.14 Subacute sclerosing panencephalitis is typically seen 7 to 10 years after infection with measles, and patients present most commonly with declining performance in school, behavioral changes, headache, adВventitious movements, and sometimes seizures.15 Characteristic findings include myoclonic jerks that are often periodic and are associated with periodic lateralized or bilateral epileptiform discharges on an electroencephalogram. Although most cases occur in childhood or adolescence, cases beginning as late as the fifth decade of life have been described.16,17 The incidence of subacute scleros- n engl j med 357;6  www.nejm.org  august 9, 2007 597 The n e w e ng l a n d j o u r na l ing panencephalitis has decreased with widespread vaccination against measles; howВever, it persists in places where measles vaccination is uncommon.18 The incidence of this condition is increased as much as 10 times in patients in whom measles develops before the age of 2 years; this patient had measles at 4 months of age. The illness may present during pregnancy, possibly as a result of altered immune status.8,19 In summary, this patient presented with a subacute progressive neurologic disease characterized by widespread dysfunction of the central nervous system, inflammatory features in the cerebrospinal fluid, and an extremely high level of cerebrospinal fluid IgG. My colleagues and I favored the diagnosis of subacute sclerosing panencephalitis, a delayed consequence of her infection with measles at 4 months of age. This condition may have been exacerbated by her pregnancy. Specimens of serum and cerebrospinal fluid from the 14th hospital day were sent for testing of levels of antibodies against measles. Dr. Roehrl: The measles-specific cerebrospinal fluid to serum IgG antibody index was elevated at 31.8 (normal value, <1.4)7 (Table 3). Measles-specific IgM antibodies were not detectВed in the serum. This profile indicates a chronic immune response to measles infection in the cerebrospinal fluid compartment. A comparison with mumps titers shows the specificity of the immunologic process. The results confirm the diagnosis of subacute sclerosing panencephalitis in the patient. The disease was a late consequence of persistent infection with measles virus. Dis cus sion of M a nage men t Dr. Cole: Cell-mediated immunity stimulated by T-helper cell type 1 (Th1) inducing cytokines is crucial for the clearance of measles virus in the weeks after infection, whereas cytokines that induce type 2 helper T (Th2) cells are implicated in antibody production. Several reports have suggested that treatment with intrathecal interferon alfa-2 (a cytokine that promotes Th1 activity), with or without treatment with the antiviral immunomodulatory agent inosine pranobex, may slow or even arrest the progression of subacute sclerosing panencephalitis.20-25 However, no definitive data are available to show the efficacy of this treatment approach. When we made the diagnosis in this patient, 598 of m e dic i n e Table 3. Results of Blood and Cerebrospinal Fluid Tests for Measles and Mumps Antibodies on Hospital Day 14. Test Result Blood Cerebrospinal Fluid Measles IgM Negative 1:512 IgG >1:800,000 1:81,920 IgM Negative Negative IgG 1:512 1:32 Mumps she was at 28 weeks of gestation, and her condition was deteriorating rapidly. We believed that an attempt at treatment was in the best interest of the patient and her fetus. We treated her with interferon and inosine pranobex for 8 weeks, without any clear clinical benefit. After the delivery of a healthy baby by elective cesarean section at 34 weeks’ gestation, a decision was made to discontinue treatment, with the consent of the patient’s mother. The patient died 6 weeks later. DR . A NDR E W J. C OL E’S DI AGNOSIS Subacute sclerosing panencephalitis. Pathol o gic a l Dis cus sion Dr. Matthew P. Frosch: The autopsy revealed inflammatory infiltrates containing macrophages, plasma cells, and lymphocytes around vessels, with neuronal destruction and reactive gliosis that were most prominent in the brain stem (Fig. 4A). No viral inclusions of the type usually seen in acute measles encephalitis (and occasionally present in subacute sclerosing panencephalitis) were seen in the nuclei or cytoplasm of any cell types (neurons, glia, or vascular endothelial cells). Unlike other measles-associated diseases, subacute sclerosing panencephalitis is caused by the persistence of defective viruses that do not form complete viral particles but may infect adjacent cells by direct contact.26,27 In the cerebral cortex, neuronal populations were preserved, but there was marked gliosis with reactive astrocytes (Fig. 4B). The brain stem was softened by the pathologic process, but the hemispheric white matter was firmer than normal; this was most evident when the brain was cut in the fresh state. This firmness corresponds to the sclerosis in the name, subacute n engl j med 357;6  www.nejm.org  august 9, 2007 case records of the massachuset ts gener al hospital nonspecific, but together with the serologic studies, they are consistent with a diagnosis of subA acute sclerosing panencephalitis. Fixed and frozen specimens of brain tissue were sent to Dr. William Bellini at the Centers for Disease Control and Prevention for immunohistochemical and molecular diagnostic studies.14,28‑30 Immunohistochemical analysis for measles virus nucleoprotein antigen was negative. Molecular diagnostic studies performed to detect portions of the measles genome were negative in repeated attempts at amplification of regions of the measles nucleoprotein gene. Weak signals were B detected in a real-time reverse-transcriptase– polymerase-chain-reaction assay, but there were insufficient amounts of amplified DNA product to perform a sequence analysis. As a result, it was not possible to definitively establish the presence of measles virus in this case. Dr. Nancy Lee Harris (Pathology): Dr. Cort, who prepares the case histories for these exercises, was able to obtain some additional history, which was not available to the patient’s caregivers. Dr. Alice M. Cort (Internal Medicine): Two years before admission, the patient was seen in the C emergency department of another hospital because of an episode of loss of consciousness that was associated with rolling of the eyes and arching of the back. On examination, there were intermittent involuntary movements of the head and neck and jerking movements of the arms. Deeptendon reflexes were brisk and symmetric. CT scanning of the head and an electroencephalogram were normal. Further testing showed an early pregnancy, which was electively terminated. During the next 20 months, the patient was lost to medical follow-up, and it is not known whether Figure 4. Findings in the Brain at Autopsy. the abnormal movements stopped. A marked inflammatory infiltrate around the vessels and Dr. Harris: Dr. Cole, is it possible that subacute neuronal destruction are most prominent in this section RETAKE plasma 1st AUTHOR Cole contains macrophages, ICM brain sclerosing panencephalitis began during this paof the stem, which 2nd REGand F lymphocytes; FIGURE 4a-c ofthere 4 cells, is prominent perivascular tient’s previous pregnancy, stabilized, and then 3rd CASE by TITLE cuffing lymphocytes (Panel A, hematoxylinRevised and eosin). worsened with the second pregnancy? EMail Linepopulations 4-C are preserved, In the cerebral cortex, neuronal SIZE Dr. Cole: Subacute sclerosing panencephalitis Enon ARTIST: mst H/T (Panel H/T but a marked gliosis is present B, immunohisto16p6 FILL Combo is almost always a chronically progressive disease, chemical analysis for glial fibrillary acidic protein). Marked AUTHOR, PLEASEinNOTE: although plateaus in the clinical course have been microglial activation is present the subcortical white Figure has been redrawn and type has been reset. matter with rod-shaped CD68-positive described. The duration of the disease can be Please check carefully. cells (Panel C, arrows; hematoxylin and eosin) (inset, immunohistoyears, however, and in retrospect, her symptoms chemical JOB: staining 35706 for CD68). ISSUE: 8-9-07 2 years earlier may have been an earlier manifestation of the same disease. The effect of the pasclerosing panencephalitis. The subcortical white tient’s treatment on the appearance of the brain matter also showed reactive gliosis and extensive at autopsy and on the ability to detect viral antimicroglial activation (Fig. 4C). These findings are gens or DNA is not known. n engl j med 357;6  www.nejm.org  august 9, 2007 599 case records of the massachuset ts gener al hospital A nat omic a l Di agnosis Subacute sclerosing panencephalitis secondary to measles virus infection. Dr. Cole reports receiving consulting fees from GlaxoSmithKline, Abbott Laboratories, and Supernus Pharmaceuticals and lecture fees from GlaxoSmithKline, Abbott Laboratories, and Ortho-McNeil; References 1. al-Eissa A. Sydenham’s chorea: a new look at an old disease. Br J Clin Pract 1993; 47:14-6. 2. Levine JS, Branch DW, Rauch J. The antiphospholipid syndrome. N Engl J Med 2002;346:752-63. 3. Menge T, Hemmer B, Nessler S, et al. Acute disseminated encephalomyelitis: an update. Arch Neurol 2005;62:1673-80. 4. Thompson EJ, Riches PG, Kohn J. AntiВ body synthesis within the central nervous system: comparisons of CSF IgG indices and electrophoresis. J Clin Pathol 1983;36: 312-5. 5. Reiber H. The discrimination between different blood-CSF barrier dysfunctions and inflammatory reactions of the CNS by a recent evaluation graph for the protein profile of cerebrospinal fluid. J Neurol 1980;224:89-99. 6. Idem. Flow rate of cerebrospinal fluid (CSF) — a concept common to normal blood-CSF barrier function and to dysfunction in neurological diseases. J Neurol Sci 1994;122:189-203. 7. Reiber H, Peter JB. Cerebrospinal fluid analysis: disease-related data patterns and evaluation programs. J Neurol Sci 2001;184:101-22. 8. Case Records of the Massachusetts General Hospital (Case 15-1998). N Engl J Med 1998;338:1448-56. 9. Fishman RA. Cerebrospinal fluid in diseases of the nervous system. 2nd ed. Philadelphia: W.B. Saunders, 1992. 10. Norrby E, Vandvik B. Relationship between measles virus-specific antibody activities and oligoclonal IgG in the central nervous system of patients with subacute sclerosing panencephalitis and multiple sclerosis. Med Microbiol Immunol 1975; 162:63-72. 11. Wolinsky JS. Progressive rubella panencephalitis. In: Vinken PJ, Bruyn GW, Klawans HL, McKendall RR, eds. Viral disease. Amsterdam: Elsevier, 1989:405-16. Dr. Henson, consulting fees from GlaxoSmithKline; and Dr. Frosch, consulting fees from Biogen Idec and Bristol-Myers Squibb. No other potential conflict of interest relevant to this article was reported. We thank Dr. Mandakolathur R. Murali, director of the Clinical Immunology Laboratory, Department of Pathology, Massachusetts General Hospital, for the analysis of the immunologic findings in the cerebrospinal fluid. 12. Townsend JJ, Baringer JR, Wolinsky JS, et al. Progressive rubella panencephalitis: late onset after congenital rubella. N Engl J Med 1975;292:990-3. 13. Weil ML, Itabashi H, Cremer NE, OshiВ ro L, Lennette EH, Carnay L. Chronic progressive panencephalitis due to rubella virus simulating subacute sclerosing panencephalitis. N Engl J Med 1975;292:994-8. 14. Honarmand S, Glaser CA, Chow E, et al. Subacute sclerosing panencephalitis in the differential diagnosis of encephalitis. Neurology 2004;63:1489-93. 15. Swoveland PT, Johnson KP. Subacute sclerosing panencephalitis and other paramyxovirus infections. In: Vinken PJ, Bruyn GW, Klawans HL, McKendall RR, eds. Viral disease. Amsterdam: Elsevier, 1989:417. 16. Gagnon A, Bouchard RW. Fulminating adult-onset subacute sclerosing panencephalitis in a 49-year-old man. Arch Neurol 2003;60:1160-1. 17. Prashanth LK, Taly AB, Ravi V, Sinha S, Arunodaya GR. Adult onset subacute sclerosing panencephalitis: clinical profile of 39 patients from a tertiary care centre. J NeuВ rol Neurosurg Psychiatry 2006;77:630-3. 18. Bellini WJ, Rota JS, Lowe LE, et al. Subacute sclerosing panencephalitis: more cases of this fatal disease are prevented by measles immunization than was previously recognized. J Infect Dis 2005;192:1686-93. 19. Wirguin I, Steiner I, Kidron D, et al. Fulminant subacute sclerosing panencephВ alitis in association with pregnancy. Arch Neurol 1988;45:1324-5. 20. Gokcil Z, Odabasi Z, Demirkaya S, Eroglu E, Vural O. Alpha-interferon and isoprinosine in adult-onset subacute sclerosing panencephalitis. J Neurol Sci 1999; 162:62-4. 21. Anlar B, Yalaz K, Oktem F, KГ¶se G. Long-term follow-up of patients with subacute sclerosing panencephalitis treated with intraventricular alpha-interferon. Neurology 1997;48:526-8. 22. Gascon G, Yamani S, Crowell J, et al. Combined oral isoprinosine-intraventricular alpha-interferon therapy for subacute sclerosing panencephalitis. Brain Dev 1993; 15:346-55. 23. Yalaz K, Anlar B, Oktem F, et al. Intraventricular interferon and oral inosiplex in the treatment of subacute sclerosing panencephalitis. Neurology 1992;42:488-91. 24. Steiner I, Wirguin I, Morag A, AbramВ sky O. Intraventricular interferon treatment for subacute sclerosing panencephalitis. J Child Neurol 1989;4:20-4. 25. Panitch HS, Gomez-Plascencia J, Norris FH, Cantell K, Smith RA. Subacute sclerosing panencephalitis: remission after treatment with intraventricular interferon. Neurology 1986;36:562-6. 26. Ueda S, Okuno Y, Hamamoto Y, Oya H. Subacute sclerosing panencephalitis (SSPE): isolation of a defective variant of measles virus from brain obtained at autopsy. Biken J 1975;18:113-22. 27. Hirano A, Ayata M, Wang AH, Wong TC. Functional analysis of matrix proteins expressed from cloned genes of measles virus variants that cause subacute sclerosing panencephalitis reveals a common defect in nucleocapsid binding. J Virol 1993; 67:1848-53. 28. Zaki SR, Bellini WJ. Measles. In: Connor DH, Chandler FW, Schwartz DA, Manz HJ, Lack EE, eds. Pathology of infectious diseases. Stamford, CT: Appleton & Lange, 1997:233-44. 29. Bellini WJ, Rota JS, Lowe LE, et al. Subacute sclerosing panencephalitis: more cases of this fatal disease are prevented by measles immunization than previously recognized. J Infect Dis 2005;192:1686-93. 30. Hummel KB, Lowe L, Bellini WJ, Rota PA. Development of quantitative genespecific real-time RT-PCR assays for the deВ tection of measles virus in clinical specimens. J Virol Methods 2006;132:166-73. Copyright В© 2007 Massachusetts Medical Society. Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neuroВ logic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record. The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail Pathphotoslides@partners.org. 600 n engl j med 357;6  www.nejm.org  august 9, 2007 The n e w e ng l a n d j o u r na l of m e dic i n e edi t or i a l s Safer Drugs for the American People Gregory D. Curfman, M.D., Stephen Morrissey, Ph.D., and Jeffrey M. Drazen, M.D. By wide margins, both the House and the Senate have now passed bills that aim to ensure the safety of the drug supply in the United States.1,2 Given the serious safety problems that have arisen with drugs taken by millions of Americans, this legislation is long overdue. It is now up to both houses of Congress to resolve the differences between the two versions and agree on a strong final bill to send to the President. This year, Congress had to consider reauthorization of the Prescription Drug User Fee Act (PDUFA), which it must do every 5 years. Under PDUFA, the major funding for the review of new drugs by the Food and Drug Administration (FDA) comes from user fees paid by pharmaceutical companies. This mechanism has been controversial because, although it was designed to accelerate the drug-approval process and can make new drugs available to patients without delay, it has directed no money to the postmarketing assessment of drug safety. In addition, some believe that user fees pose a conflict of interest for the FDA. Nonetheless, to ensure that the FDA has adequate financial resources, both the House and the Senate versions of the bill not only maintain these user fees but increase them (with some of the money now directed to safety assessment). In reauthorizing PDUFA, Congress has wisely taken the opportunity to strengthen the FDA’s authority over drug safety, and both versions of the bill give the FDA new tools to accomplish this objective. At a minimum, we believe that the final bill should contain the following essential components. The FDA must have the authority to mandate adequately powered postmarketing clinical trials of the safety of approved drugs and to require specific timetables for their completion and reporting of results. 602 The FDA must also have the authority to conduct an annual review of drug safety for the first 3 years after a drug’s approval and again at 7 years. To assist patients in reporting adverse effects of the drugs they are taking, drug advertisements and labels must include a toll-free telephone number and a Web address. There must be substantial penalties for drug advertising that overstates efficacy or understates adverse effects. The FDA must be able to mandate changes to drug labels as new information about safety and efficacy becomes available. In order to provide safety surveillance, every new drug should have a pharmacovigilance plan at the time of its approval. Sophisticated pharmacoepidemiologic surveillance systems must be created to allow the FDA to monitor reports of adverse drug effects in large databases. Clinical trials of drugs must be registered in a public database. In the wake of the landmark report on drug safety issued by the Institute of Medicine almost a year ago,3 Congress is now poised to pass the most important drug-safety legislation in a century. Although we remain concerned about the user-fee approach to funding of the FDA, we believe that the bills initiated by Congressmen Henry Waxman and Edward Markey and by Senators Edward Kennedy and Michael Enzi are important steps in the right direction. Congress should now speedily agree on a substantive drugsafety bill and give the FDA the tools it needs to do its work. The crisis of confidence in the nation’s drug supply must be resolved. This article (10.1056/NEJMe078154) was published at www. nejm.org on July 18, 2007. 1. H.R. 2900, 110th Cong. (2007). n engl j med 357;6  www.nejm.org  august 9, 2007 editorials 2. S. 1082, 110th Cong., 1st Sess. (2007). 3. Committee on the Assessment of the US Drug Safety System, Baciu A, Stratton K, Burke SP, eds. The future of drug safety: promoting and protecting the health of the public. Washington, DC: National Academies Press, 2006. (Available at http://www. iom.edu/CMS/3793/26341/37329.aspx.) Copyright В© 2007 Massachusetts Medical Society. Prophylactic Treatment for Prevention of Joint Disease in Hemophilia — Cost versus Benefit Goris Roosendaal, M.D., Ph.D., and Floris Lafeber, Ph.D. Patients with severe hemophilia number only around 400,000 worldwide, but their lifespan has increased because of improved treatment, and with that the prevalence of the disease is increasing. Despite the relatively small number of patients with severe hemophilia, the disease has an important socioeconomic effect because of its distinctive feature: a level of clotting factor (factor VIII or factor IX) so low that without replacement therapy, frequent hemorrhages occur, most often in the ankle, knee, and elbow joints. These joint hemorrhages culminate in a severe arthropathy, with signs of inflammation (as in rheumatoid arthritis) as well as degenerative damage (as in osteoarthritis).1,2 As a result of these hemorrhages, patients with hemophilic arthropathy can become disabled at a relatively young age. Joint bleeding in hemophilia can be prevented by the administration of a concentrated clotting factor derived from plasma (cryoprecipitate) or a recombinant clotting protein. Since these products are expensive, the beneficial results they have to offer should be balanced by a consideration of their cost. In this issue of the Journal, Manco-Johnson and colleagues report the results of a randomized study that assessed the clinical benefit of a very costly product, recombinant factor VIII, for the prophylactic treatment of young boys (up to the age of 6 years) with severe hemophilia.3 Prophylaxis, a scheduled intravenous injection of clotting factor in anticipation of bleeding, was compared with on-demand, or episodic, treatment, the administration of clotting factor whenever signs of joint bleeding appeared. The benefit of prophylaxis as compared with episodic treatment was clear. After a mean follow-up of 49 months, 93% of the patients in the prophylaxis group showed no joint damage on magnetic resonance imaging as compared with 55% in the episodic- therapy group. The number of infused units of factor VIII per participant was approximately 350,000 in the prophylaxis group (with 0.63 joint hemorrhage per year) and approximately 113,000 in the episodic-therapy group (with 4.89 joint hemorrhages per year). Several previous retrospective or uncontrolled studies have suggested the superiority of prophylaxis,4,5 but the study by Manco-Johnson et al. is a controlled randomized trial comparing the effects of prophylaxis with episodic treatment in hemophilia. The study puts a harsh light on cost–benefit issues in the management of hemophilia: the estimated annual cost for prophylactic treatment of one patient with recombinant factor VIII was $300,000. Manco-Johnson and her colleagues comment that “the high cost of recombinant factor VIII is a barrier to widespread acceptance of prophylaxis.” With the current challenges entailed in reducing health care costs, this is a reality we must deal with, a challenge to further optimize the balance between cost and benefit. In the balance of cost with the efficacy of treatment in hemophilia, it is important to consider that inadequately treated patients make great demands on the health care system. Such patients often need expensive additional treatment, such as joint replacement. Yet the kind of cost-effectiveness studies that have been performed for many other chronic diseases have never been performed for hemophilia. The dilemma in managing hemophilia is not whether to use prophylaxis or episodic treatment but how to manage prophylaxis such that the optimal, most cost-effective treatment is provided. The crux of the problem is this: How many joint hemorrhages can be tolerated before disabling arthropathy occurs, and how can clottingfactor replacement therapy be managed such that optimal prevention of joint bleeding is achieved? n engl j med 357;6  www.nejm.org  august 9, 2007 603 The n e w e ng l a n d j o u r na l The study by Manco-Johnson and colleagues provides little help in answering these questions. The authors conclude that “Prophylaxis was efficacious in decreasing bleeding and joint damage after up to five hemarthroses.” At the population level, their conclusion is correct, but what does it mean for the individual patient? Could it be that patients who had no joint hemorrhages before the start of prophylaxis were at a lower risk for a subsequent joint hemorrhage than patients who started prophylaxis after having one or more joint hemorrhages? In the prophylaxis group, 18 patients had had at least one joint hemorrhage before treatment and 14 patients had no previous hemorrhage. This difference provides a unique opportunity to evaluate these subgroups for the development of joint damage despite prophylaxis. The outcome of such an analysis might be anticipated, considering the patients’ long experience with hemophilia. Nilsson and colleagues6 have noted progressive deterioration in joints that are damaged before the start of prophylaxis, whether or not there is further bleeding into those joints. Petrini and colleagues7 and Fischer et al.8 found that the early institution of prophylaxis — before the age of 3 years or before the third joint hemorrhage — resulted in radiologic and orthopedic scores that were significantly better than those associated with later commencement of prophylaxis (after the age of 5 years). Progression of arthropathy continued in children in both groups who had experienced more than five joint hemorrhages before the start of prophylaxis, whether it was instituted early or late in childhood. Kreuz and colleagues9 also found a worsening of joint scores despite ongoing prophylaxis in patients who had a median of six joint hemorrhages before starting prophylaxis. These results fit well with the lack of correlation between the number of hemorrhages and the severity (progression rate) of arthropathy in the study by Manco-Johnson et al. It may be that the first episode of bleeding or early episodes initiate a self-perpetuating arthropathy and that subsequent episodes of bleeding only accelerate the degenerative process. Even a small number of joint hemorrhages can cause irreversible joint alterations, leading to an arthropathy that can be slowed by prophylaxis but not prevented. In this regard, it is notable that culturing full-thickness articular cartilage explants in 604 of m e dic i n e the presence of blood, even for a short period of time, has devastating effects on chondrocyte activity and cartilage integrity.10,11 For all these reasons, it seems that prophylaxis will be most effective if it can prevent joints from reaching the point of no return. But determining when to start prophylaxis is difficult because severe hemophilia varies considerably in terms of the number and frequency of joint hemorrhages.12 Starting prophylaxis at a very early age could be cost-effective because young patients, with their low body weight, require only small amounts of clotting factor. Moreover, the preservation of joint structure with early initiation of prophylaxis is thought to result in fewer episodes of bleeding later in life, less disability in adults, and therefore lower health care costs. It seems reasonable, in light of all these considerations, to begin prophylaxis after the occurrence of one joint hemorrhage rather than at a fixed age.13 Subsequent prophylaxis can be tailored to the individual patient, on the basis of that patient’s clinical course, to achieve optimum costeffectiveness.14 The study by Manco-Johnson and colleagues provides renewed and detailed evidence that prophylaxis in severe hemophilia with recombinant factor VIII has clinical benefit despite its huge costs. However, we must await prospective studies that demonstrate the most balanced approach, weighing possible adverse events and cost against benefits. No potential conflict of interest relevant to this article was reported. From the Department of Hematology and Van Creveld Clinic and the Department of Rheumatology and Clinical Immunology, University Medical Center Utrecht, Utrecht, the Netherlands. 1. Roosendaal G, van Rinsum AC, Vianen ME, van den Berg HM, Lafeber FP, Bijlsma JW. Haemophilic arthropathy resembles degenerative rather than inflammatory joint disease. Histopathology 1999;34:144-53. 2. Wen FQ, Jabber AA, Chen YX, Kazarian T, Patel DA, Valentino LA. c-myc Proto-oncogene expression in hemophilic synovitis: in vitro studies of the effects of iron and ceramide. Blood 2002;100:912-6. 3. Manco-Johnson MJ, Abshire TC, Shapiro AD, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med 2007;357:535-44. 4. Liesner RJ, Khair K, Hann IM. The impact of prophyactic treatment on children with severe haemophilia. Br J Haematol 1996;92:973-8. 5. Aledort LM, Haschmeyer RH, Pettersson H. A longitudinal study of orthopaedic outcomes for severe factor-VIII-deficient haemophiliacs. J Intern Med 1994;236:391-9. 6. Nilsson IM, Berntorp E, LГ¶fqvist T, Pettersson H. Twentyfive years’ experience of prophylactic treatment in severe haemophilia A and B. J Intern Med 1992;232:25-32. n engl j med 357;6  www.nejm.org  august 9, 2007 editorials 7. Petrini P, Lindvall N, Egberg N, BlombГ¤ck M. Prophylaxis with factor concentrates in preventing hemophilic arthropathy. Am J Pediatr Hematol Oncol 1991;13:280-7. 8. Fischer K, van der Bom JG, Mauser-Bunschoten EP, et al. The effects of postponing prophylactic treatment on long-term outcome in patients with severe hemophilia. Blood 2002;99:2337-41. 9. Kreuz W, Escuriola-Ettingshausen C, Funk M, Schmidt H, Kornhuber B. When should prophylactic treatment in patients with haemophilia A and B start? The German experience. Haemophilia 1998;4:413-7. 10. Jansen NW, Roosendaal G, Bijlsma JW, Degroot J, Lafeber FP. Exposure of human cartilage tissue to low concentrations of blood for a short period of time leads to prolonged cartilage damage: an in vitro study. Arthritis Rheum 2007;56:199-207. 11. Hooiveld M, Roosendaal G, Vianen M, van den Berg M, Bijlsma J, Lafeber F. Blood-induced joint damage: longterm effects in vitro and in vivo. J Rheumatol 2003;30:339-44. 12. van Dijk K, van der Bom JG, Lenting PJ, et al. Factor VIII half-life and clinical phenotype of severe hemophilia A. Haematologica 2005;90:494-8. 13. Roosendaal G, Lafeber FP. Pathogenesis of haemophilic arthropathy. Haemophilia 2006;12:Suppl 3:117-21. 14. Astermark J, Petrini P, Tengborn L, Schulman S, Ljung R, Berntorp E. Primary prophylaxis in severe haemophilia should be started at an early age but can be individualized. Br J Haematol 1999;105:1109-13. Copyright В© 2007 Massachusetts Medical Society. Rituximab and Pemphigus — A Therapeutic Advance Luis A. Diaz, M.D. Pemphigus vulgaris and pemphigus foliaceus are rare autoimmune blistering diseases of obscure causes. The scientific bases for the therapy of these disorders have evolved in the past 60 years. Landmark studies demonstrated that intraepidermal blisters were subcorneal in pemphigus foliaceus1 and suprabasilar in pemphigus vulgaris2,3 and suggested that an ongoing process of epidermal-cell detachment (acantholysis) led to blister formation. Armed with this limited information, dermatologists in the 1950s began to use systemic steroids to treat these diseases. Before the use of corticosteroids, the diagnosis of pemphigus carried a poor prognosis; it was believed that if a patient survived for more than a year, the diagnosis of pemphigus was probably incorrect. The autoimmune nature of these diseases was substantiated in the 1960s, when Beutner and Jordon4 discovered that pemphigus vulgaris and pemphigus foliaceus antiepidermal autoantibodies were present in patients with these disorders. In the 1980s my colleagues and I showed by passive transfer experiments that pemphigus vulgaris and pemphigus foliaceus autoantibodies faithfully reproduced the disease in the epidermis of neonatal mice.5,6 Stanley and coworkers7,8 showed that the epidermal antigens recognized by pemphigus vulgaris and pemphigus foliaceus autoantibodies were desmoglein 3 and desmoglein 1, respectively, both members of the cadherin superfamily of adhesion molecules. The molecular mechanisms of the epidermal acantholysis triggered by pemphigus vulgaris and pemphigus foliaceus autoantibodies remain unknown, but they are the subject of intense investigation in several laboratories.9 The autoimmune nature of pemphigus was used as a rationale for the introduction of immunosuppressive drugs and plasmapheresis, both aimed at eliminating pathogenic autoantibodies from the patient. The combined use of systemic steroid and immunosuppressive agents such as azathioprine, cyclophosphamide, methotrexate, mycophenolate mofetil, and cyclosporine has become the standard of therapy for pemphigus vulgaris and pemphigus foliaceus with good results. However, the morbidity associated with the longterm use of these drugs remains problematic for the patients, especially those with diabetes, hypertension, or other medical conditions. Since the introduction of systemic steroids in the 1950s and immunosuppressive agents in the 1960s, the prognosis for patients with the disease has been gradually improving. Recent reports estimate an overall 5% mortality rate due to complications from therapy for patients with pemphigus vulgaris.10 During the past 10 years we have witnessed the arrival of new and exciting therapies for pemphigus. Infusions of intravenous immune globulins and B-cell–targeted humanized monoclonal antibodies are two examples. Rituximab is an anti-CD20 chimeric monoclonal antibody approved by the Food and Drug Administration for the treatment of B-cell non-Hodgkin’s lymphoma and rheumatoid arthritis that is refractory to anti– tumor necrosis factor О±. These therapies are especially useful in cases of pemphigus that are not responsive to conventional therapy with corticosteroids and immunosuppressive drugs. In this n engl j med 357;6  www.nejm.org  august 9, 2007 605 The n e w e ng l a n d j o u r na l issue of the Journal, Joly and colleagues11 report a prospective open trial of rituximab in patients with pemphigus vulgaris or pemphigus foliaceus who had not had a response to prednisone at a dose of 1.5 mg per kilogram of body weight per day, who had active disease despite systemic doses of prednisone greater than 20 mg per day, or in whom systemic corticosteroids were contraindicated. Treatment with adjuvant intravenous immune globulins and immunosuppressive therapy was described as having failed in some of these patients. Eighteen of 21 patients who were treated with four weekly infusions of rituximab had a complete clinical remission by 3 months. In 8 of the 18 patients, this remission was maintained without corticosteroid or immunosuppressive therapy after a median follow-up of almost 3 years. One patient died of septicemia, and pyelonephritis developed in another. In addition to the clinical response, Joly and colleagues also followed the progression of certain immunologic markers. Three weeks after the onset of therapy, peripheral-blood B cells decreased by a dramatic 99% and remained undetectable for 6 months in two patients. B cells reappeared after 6 months. No changes were detected in T cells or in the titers of antibodies against pneumococcal capsule polysaccharide, tetanus toxoid, or total IgG values. There was a significant decrease of anti–desmoglein 1 and anti– desmoglein 3 autoantibodies 3 months after the onset of therapy. These autoantibodies reappeared in the serum of patients during relapses. Of note, in five patients with pemphigus vulgaris who were in complete clinical remission, the titers of autoantibodies remained elevated. These studies point toward the relevance of certain “pathogenic” epitopes on the ectodomain of desmoglein 1 and desmoglein 3, as previously reported.12 One of the conclusions of Joly and colleagues is that pemphigus vulgaris and pemphigus foliaceus are life-threatening skin diseases that are mediated by antigen-specific activated B cells and their products — that is, anti–desmoglein 3 and anti–desmoglein 1 autoantibodies. These autoantibodies are IgG4 restricted and pathogenic in most patients; their effect may depend on the epidermal-cell epitopes they bind. Since the clinical remission induced by rituximab in patients with pemphigus vulgaris and pemphigus foliaceus was associated with a decrease in the titers of anti– desmoglein 3 and anti–desmoglein 1 autoanti606 of m e dic i n e bodies without changes in the titers of antipneumococcal and antitetanus antibodies, it may be assumed that these antibodies eliminate desmoglein 1–specific and desmoglein 3–specific B-cell precursors. It has been proposed that long-lived plasma cells produce antigen-specific autoantibodies that show stable titers in the serum of patients, whereas short-lived plasma cells and plasmablasts produce antigen-specific autoantibodies in titers that fluctuate with disease activity.13 Long-lived and short-lived plasma cells do not express the CD20 antigen; consequently, by eliminating a large population of B cells with rituximab therapy, it may be possible to eliminate a substantial number of desmoglein 1 and desmoglein 3 B-cell precursors of short-lived plasma cells. It is clear that further studies are needed to disclose the molecular and cellular mechanisms of action of rituximab. In summary, the article by Joly et al. supports previous reports that describe the beneficial effects of rituximab in the treatment of pemphigus without the need for infusions of intravenous immune globulins; however, its use must be restricted to a limited number of patients with pemphigus vulgaris or pemphigus foliaceus that is not responsive to conventional therapy (e.g., systemic corticosteroids and immunosuppressive agents) or to patients in whom these drugs may be harmful. Caution should be exercised in the use of rituximab because of the risk of serious short-term complications such as viral and bacterial infections and the potential for as yet unknown long-term complications. Finally, this study demonstrates the value of a multicenter approach to accomplish relevant clinical research in orphan diseases such as pemphigus. A U.S. national registry for pemphigus and standardized tools to assess the disease activity of pemphigus are necessary to accelerate research progress. Dr. Diaz reports being named as coinventor on a patent held by the University of North Carolina for the inhibition of the phosphorylation of HSP27 (heat-shock protein 27) for the treatment of blistering disorders. No other potential conflict of interest relevant to this article was reported. From the Department of Dermatology, University of North Carolina at Chapel Hill, Chapel Hill. 1. Vieira JP. Contribuição ao estudo do pemphigo no estado de SГЈo Paulo. SГЈo Paulo: Empresa GrГЎfica da Revista dos Tribunais, 1937. 2. Civatte A. Diagnostic histopathologique de la dermatite polymorphe douloureuse ou maladie de Duhring-Brocq. Ann Dermatol Syphiligr 1943;3:1-30. 3. Lever WF. Pemphigus. Medicine (Baltimore) 1953;32:1-123. n engl j med 357;6  www.nejm.org  august 9, 2007 editorials 4. Beutner EH, Jordon RE. Demonstration of skin antibodies in sera of patients with pemphigus vulgaris by indirect immunofluorescent staining. Proc Soc Exp Biol Med 1964;117:505-10. 5. Anhalt GJ, Labib RS, Voorhees JJ, Beals TF, Diaz LA. Induction of pemphigus in neonatal mice by passive transfer of IgG from patients with the disease. N Engl J Med 1982;306:1189-96. 6. Roscoe JT, Diaz L, Sampaio SA, et al. Brazilian pemphigus foliaceus autoantibodies are pathogenic to BALB/c mice by passive transfer. J Invest Dermatol 1985;85:538-41. 7. Eyre RW, Stanley JR. Human autoantibodies against a desmosomal protein complex with a calcium-sensitive epitope are characteristic of pemphigus foliaceus patients. J Exp Med 1987; 165:1719-24. 8. Amagai M, Klaus-Kovtun V, Stanley J. Autoantibodies against a novel epithelial cadherin in pemphigus vulgaris, a disease of cell adhesion. Cell 1991;67:869-77. 9. Li N, Rubenstein DS, Liu Z, Diaz LA. Pemphigus foliaceus, pemphigus vulgaris, paraneoplastic pemphigus, bullous pemphigoid herpes gestationis and cicatricial pemphigoid. In: Runge MS, Patterson WC, eds. Principles of molecular medicine. 2nd ed. Totowa, NJ: Humana Press, 2006:959-69. 10. Herbst A, Bystryn J-C. Patterns of remission in pemphigus vulgaris. J Am Acad Dermatol 2000;42:422-7. 11. Joly P, Mouquet H, Roujeau J-C, et al. A single cycle of rituximab for the treatment of severe pemphigus. N Engl J Med 2007; 357:545-52. 12. Li N, Aoki V, Hans-Filho G, Rivitti EA, Diaz LA. The role of intramolecular epitope spreading in the pathogenesis of endemic pemphigus foliaceus (fogo selvagem). J Exp Med 2003;197: 1501-10. 13. Radbruch A, Muehlinghaus G, Luger EO, et al. Competence and competition: the challenge of becoming a long-lived plasma cell. Nat Rev Immunol 2006;6:741-50. Copyright В© 2007 Massachusetts Medical Society. view current job postings at the nejm careercenter Visit our online CareerCenter for physicians at www.nejmjobs.org to see the expanded features and services available. Physicians can conduct a quick search of the public database by specialty and view hundreds of current openings that are updated daily online at the CareerCenter. n engl j med 357;6  www.nejm.org  august 9, 2007 607 The n e w e ng l a n d j o u r na l of m e dic i n e s ounding boa r d The Tension between Needing to Improve Care and Knowing How to Do It Andrew D. Auerbach, M.D., M.P.H., C. Seth Landefeld, M.D., and Kaveh G. Shojania, M.D. The past 7 years have seen unprecedented interest in patient safety and the quality of health care.1-3 As physicians whose careers are focused on improving quality and safety, we have welcomed this change. However, we have also witnessed recent initiatives that emphasize dissemination of innovative but unproven strategies, an approach that runs counter to the principle of following the evidence4 in selecting interventions that meet quality and safety goals, as well as the idea that interventions should be tailored to local needs and resources.5 These principles have been used as safeguards in helping us pursue practices that have clear benefits for patients and that can be implemented with local resources. This approach also reflects the recognition of how little we know about ways to improve care in a large number of settings.4,6,7 Our consideration of the rationale for rapid dissemination of novel quality and safety strategies has led us to identify a number of weaknesses inherent in approaches that consistently favor action over evidence. In this article, we outline the arguments in favor of rapid dissemination and the counterpoints to each of the arguments (Table 1). We conclude by proposing a framework for evaluating interventions to improve the safety and effectiveness of health care. Ar gument 1: We C annot Wait The most common argument in favor of prioritizing action over evidence is that the need to address quality and safety problems is urgent. Often, this need is summed up by the question, “How many times does outcome X need to occur before we implement intervention Y?” This question seems particularly compelling because hundreds of thousands of patients (possibly millions) experience harm as a result of underuse, overuse, or misuse of medical therapies.8 However, similar claims about the scale of mor608 bidity and mortality could be made for heart disease, cancer, AIDS, depression, and many other disorders. Medical error may be the eighth leading cause of death in the United States,2 but by proceeding largely on the basis of urgency rather than evidence, we exempt the eighth cause of death from standards applied to the top seven. In addition, the question of how many instances of X outcome need to occur before we implement Y intervention assumes that we can define Y and X accurately, as well as connect Y to a decreased risk of X. Donabedian pointed out that Y can be either a structural element of health care (e.g., staffing ratios) or a process (e.g., administration of a drug) and emphasized the importance of establishing a connection between Y and the outcome of interest, X.9 Unfortunately, connections between structural or process-based interventions and outcomes are usually presumptive,7,10 and defining problems and solutions with respect to patient safety is generally difficult.10,11 For example, mandates to reduce residents’ work hours reflect the view that tired residents cause errors that harm patients. However, evidence linking patient harm directly to care provided by a fatigued resident is indirect,12,13 and although reductions in work hours do not appear to have harmed patients, evidence that reforms have met their goal of improving safety is tentative at best.14-18 Furthermore, to be cost-effective, a reduction in work hours would have to result in greater improvement in safety than that reported for any other intervention.19 Regardless of whether an 80-hour workweek ultimately improves patient safety, an intervention with a number of potential effects was introduced without a full understanding of its risks and benefits and without a plan to evaluate its effectiveness after implementation. Promising initiatives and bold efforts at improvement can consume tremendous resources yet confer only a small benefit15,20,21 or a benefit that n engl j med 357;6  www.nejm.org  august 9, 2007 sounding Board Table 1. Arguments for and against Rapid Dissemination of Quality-Improvement Interventions. Argument Why Proceeding Quickly Is Critical Why Evaluation Is Critical We cannot wait — the need to improve the quality of care is urgent. Thousands of patients are injured or killed each year by medical errors. The need to improve the treatment of many diseases is equally urgent, yet we demand rigorous evidence that a therapy works before recommending it widely. Any effort to improve quality is better than the current state of affairs. On balance, the harms of quality improvement are likely to be far less than those of the status quo. Knowledge of the harms and opportunity costs of quality improvement is important for an understanding of the net benefit to patients and health care systems, which is often small. Emulating successful organizations Emulation and collaboration provide can speed effective improvement. an efficient means of disseminating potentially effective solutions. Emulation and collaboration can incorrectly promote or even overlook interventions that have not worked. The effectiveness of some qualityimprovement strategies is obvious. Even though many quality-improvement practices have a simple rationale, they may be less effective than expected and can be difficult to implement fully. Insistence on evidence may lead us to underuse interventions that are obviously effective. Innovation can be catalyzed by dis- Preliminary data provide an imporsemination of strategies that tant opportunity to speed innovahave promise but are unproven. tion and improve care rapidly. Flawed, biased, or incomplete data may lead to adoption of interventions that are ineffective or harmful. The framework of evidence-based medicine does not apply to quality improvement. The nature of quality improvement exempts it from the usual strategies of assessment. Given the complexity of quality and safety problems, the complexity of their causes, and how little we understand them, we should use rigorous study designs to evaluate them. Developing evidence in quality improvement is too costly. The resources and expertise required to evaluate quality and safety interventions rigorously make trials impractical, particularly when the field is moving so quickly. As compared with the large opportunity costs incurred by wide implementation of ineffective quality and safety strategies, investments in better evaluation would be small. is at best unclear.22 How many such examples of efforts to intensify the treatment of diabetes, must we have before we decide to choose our ef- adverse consequences of many other efforts at forts more wisely? improvement of care have been less predictable, including errors introduced by computerized entry of physicians’ orders,25,26 bar coding,27 and Ar gument 2 : Any Effor t to Impr ove Is Be t ter than infection-control isolation protocols.28 Side efthe Current S tate of Affair s fects may seem inherently less likely with quality-improvement interventions than with drugs Multiple problems in our flawed health care sys- and devices. However, most quality-improvement tem lead to the view that any attempt at improve- interventions involve changes in the organizament is better than the status quo. Although tion of complex systems, and the law of uninunderstandable, this view ignores the possibil- tended consequences — long recognized as a side ity that quality-improvement efforts can cause effect of complex change — tends to apply to harm.23 Unfortunately, few studies have assessed such interventions.29-31 this possibility. For example, only 12 of 66 reports on trials of strategies to improve care for Ar gument 3: Emul ating patients with diabetes included rates of hypoglySucce ssful Or g aniz ations C an Speed Impr ovement cemia.24 However, in 7 of those 12 studies, hypoglycemia was more frequent in the intervention group than in the control group. Although A recommendation to emulate successful organihypoglycemia is an easily anticipated consequence zations reflects the reasoning that adopting fea- n engl j med 357;6  www.nejm.org  august 9, 2007 609 The n e w e ng l a n d j o u r na l tures of these organizations — the institutional culture, leadership styles, or specific improvement practices — will result in similar successes. Unfortunately, this reasoning ignores the possibility that many unsuccessful organizations also share these features, so that the truly critical determinants of success are not being targeted. For instance, continuous quality improvement and quality-improvement collaboratives are often recommended on the basis of their adoption by successful organizations. However, systematic evaluations of these approaches have shown that they result in only modest improvements at best.20,21,23,32 These disappointing findings probably reflect the overemphasis on success that is inherent in benchmarking and the collaborative approach, which tend to neglect an examination of unsuccessful organizations that share features of successful ones.33 Successful organizations may also have a vested interest in promoting their services or preferred quality-improvement strategies, further distorting the usefulness of emulating such organizations. Even when direct financial conflicts of interest do not exist, any organization that has undertaken a major campaign to improve the quality of care has little incentive to invest resources in a rigorous evaluation of the effects of its efforts. If anecdotal reports or superficial analyses are positive, the organization will understandably focus on advertising these measures of success rather than pursuing more rigorous evaluation. Ar gument 4 : The Effec tivene ss of Some Qualit y- Impr ovement S tr ategie s Is O bvious Some solutions appear to be so obviously beneficial that requiring evidence seems like asking for randomized trials of parachutes.34 However, anyone who has undertaken a quality-improvement project understands that identifying an apparent solution to a problem is only a first step. Even with pilot testing and evaluative steps, implementing solutions in practice can present numerous challenges. Hand washing is an example of a well-defined, effective solution to a problem (nosocomial infections), but strategies that consistently result in increased hand washing remain unestablished.35 Unfortunately, many initiatives fall into the hand610 of m e dic i n e washing category — that is, the case for improvement is obvious, but effective strategies for translating solutions into practice remain elusive.8 Changes in complex systems can have unanticipated consequences (as we note with respect to Argument 2), such as new problems25,26,30,31,36 or simply the failure to achieve the desired goal. Until we advance the basic sciences in quality improvement (e.g., organizational theory and ergonomics),4,7,23,32 we cannot assume that even the most apparently straightforward solutions can be seamlessly implemented. Without an understanding of not only what to do but also how to help people actually do it, many apparently obvious quality-improvement interventions have more in common with calls for world peace than with parachutes — the goal is not in question, but the path for achieving it is. Ar gument 5: Pr omising B u t Unpr oven S tr ategie s C an C ataly ze Innovation Many quality-improvement interventions have such strong face validity that their dissemination seems to be justified on the basis of early or preliminary evidence. This strategy will certainly speed dissemination, but it also carries substantial risks. Early trials of medical emergency teams suggested a large potential benefit37-40 — to the point that some observers regarded further study as unethical.41 However, a large, randomized trial subsequently showed that medical emergency teams had no effect on patient outcomes.42 The validity of the earlier positive studies has also been questioned,43 but only after many hospitals introduced medical emergency teams (and have had no reason to switch from advertising the adoption of an innovation to questioning its usefulness in the first place — Argument 3). There are many examples of drugs or devices that showed substantial promise on the basis of early findings, which were then modified or refuted by later-phase research. These often represent therapies for disorders that affect millions of people (as we note with respect to Argument 1). Yet we rarely sanction the widespread distribution of new drugs on the basis of preliminary data alone. It is therefore not clear why we favor approaches to quality improvement that foster change over appropriate evaluation. n engl j med 357;6  www.nejm.org  august 9, 2007 sounding Board It is worth emphasizing that when studies show no benefit of an intervention with strong face validity, as has occurred with rapid-response teams42 and more recently with teamwork training,44 one should not necessarily conclude that the intervention has no value. The finding may simply mean that the intervention had no effect in the form and setting that were studied. The crucial point is that without the randomized trial, we would have no way of knowing that implementation of the intervention in its current form confers no advantage over usual care (or confers a much smaller advantage than that suggested by preliminary studies) and that refinement is necessary. tion and control groups. In clinical medicine, important confounders are often well known and easily planned for, so that observational studies can adjust for these factors, thereby producing results that often agree with the results of randomized trials.48,49 However, outcomes of quality-improvement interventions depend on many factors, related to patients, providers, and organizations, that remain poorly understood. Thus, the complexity of health care and the dearth of evidence with respect to how components of the system interact to influence outcomes provide a strong rationale for conducting randomized trials to evaluate quality and safety interventions whenever feasible. Argument 6: The Framework of Evidence-based Medicine Does Not Apply to Qualit y Improvement Ar gument 7 : De veloping E vidence in Qualit y Impr ovement Is To o Cos tly A recent commentary argued that we would not require randomized trials to determine whether we have solved problems or learned skills in our daily lives.45 By extension, according to this argument, evidence-based medicine may not apply to the processes that underlie many quality-improvement initiatives. Although it is true that we often do not need trials to test our acquisition of knowledge or skills, we do need them when choosing between alternative methods of acquisition — particularly when training is costly or the skill is of high value. Rigorous evaluation does not always require randomized trials. Alternative designs (e.g., before-and-after studies that include concurrent control groups and time-series designs involving multiple preintervention and postintervention measurements) can sometimes provide robust results,32,46 as can research that combines quantitative and qualitative approaches.47 But anecdotal reports and simple before-and-after studies, although sometimes adequate to justify local quality-improvement efforts, are probably never sufficient to support widespread initiatives because of the risks of expending tremendous resources without obtaining a true benefit and possibly introducing new problems. Randomized, controlled trials, although not always necessary,46 remain highly relevant to quality improvement. The value of such trials lies in the random assignment of subjects with unknown characteristics that affect outcomes to interven- Many people have argued that with limited resources available for quality-improvement efforts, the costs of evaluation are untenable. However, one could also argue that we should not spend scarce resources on quality improvement unless we know it is effective. More important, there are tremendous opportunity costs. An institution that invests millions of dollars or expends hundreds of personnel hours in implementing an ineffective system almost certainly could have made other investments that would have benefited its patients. Moreover, if the investment at one hospital is multiplied by thousands of hospitals across the country, then surely spending several million dollars for evaluation is cost-effective, given the billions of dollars at stake with widespread implementation. In this sense, it is the absence of evidence — with respect to efficacy, possible harms, and strategies for implementation — that is too costly, not the efforts to generate such evidence. Conclusions The urge to favor action over evidence in efforts to improve the quality and safety of health care is understandable. However, we have seen in recent years that progress in quality improvement occurs just as it does in the rest of biomedicine: interventions that appear to be promising on the basis of preliminary studies often prove to have no benefit, and those that are beneficial typi- n engl j med 357;6  www.nejm.org  august 9, 2007 611 The n e w e ng l a n d j o u r na l of m e dic i n e cally result in modest improvements, not monu- to harms, squander scarce resources, or delude mental breakthroughs. And quality-improvement us about the effectiveness of our efforts. interventions, like clinical therapies, can have unSupported by a Patient Safety Research and Training Grant toward effects and both direct and indirect costs. from the Agency for Healthcare Research and Quality (K08 These commonalities compel us to argue that in- HS11416-02, to Dr. Auerbach), an Academic Leadership Award from the National Institute on Aging (K07 AG00912, to Dr. terventions to improve the quality and safety of Landefeld), and funding from the Government of Canada Rehealth care should meet the same standards that search Program (to Dr. Shojania). No potential conflict of interest relevant to this article was reare applied to the adoption of all medical techported. nologies. We thank Erin Hartman, M.S., Ralph Gonzales, M.D., M.S.P.H., In the rest of biomedicine, innovation begins and Chaim Bell, M.D., M.P.H., for their helpful comments on with basic-science experimentation and proceeds an early version of the manuscript. through evaluative trials in successive phases. From the University of California, San Francisco, Department The basic sciences in quality improvement differ of Medicine, San Francisco (A.D.A., C.S.L.); San Francisco Vetfrom those in the rest of biomedicine, but the erans Affairs Medical Center, San Francisco (C.S.L.); and Ottawa Health Research Institute, Ottawa (K.G.S.). framework for evaluating candidate interventions is largely the same. Clinicians often make deci- 1. Institute of Medicine. Crossing the quality chasm: a new sions about treatment in individual patients on health system for the 21st century. Washington, DC: National Academy Press, 2001. the basis of limited evidence or even just intu- 2. Kohn LT, Corrigan JM, Donaldson MS, eds. To err is human: ition. Similarly, individual hospitals may pursue building a safer health system. Washington, DC: National Acadpromising quality-improvement strategies on the emy Press, 2000. 3. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The basis of scant evidence, including anecdotal re- 100,000 Lives Campaign: setting a goal and a deadline for imports or face validity. However, clinical practices proving health care quality. JAMA 2006;295:324-7. based on such limited evidence would never be- 4. Brennan TA, Gawande A, Thomas E, Studdert D. Accidental deaths, saved lives, and improved quality. N Engl J Med 2005; come broad standards of care, much less require- 353:1405-9. ments for accreditation or reimbursement. Simi- 5. Nelson EC, Batalden PB, Ryer JC, eds. The clinical improvelarly, recommending or mandating the widespread ment action guide. Oakbrook Terrace, IL: Joint Commission on Accreditation of Healthcare, 1998. adoption of interventions to improve quality or 6. Forster AJ, Shojania KG, van Walraven C. Improving patient safety requires rigorous testing to determine safety: moving beyond the “hype” of medical errors. CMAJ whether, how, and where the intervention is ef- 2005;173:893-4. 7. Shojania KG, Duncan BW, McDonald KM, Wachter RM. Safe fective — just as in the rest of medicine. Clarifi- but sound: patient safety meets evidence-based medicine. JAMA cation of this picture is critical because a num- 2002;288:508-13. ber of widely promulgated interventions are likely 8. Chassin MR, Galvin RW. The urgent need to improve health care quality: Institute of Medicine National Roundtable on to be wholly ineffective, even if they do not harm Health Care Quality. JAMA 1998;280:1000-5. patients. Even worse, in the current environment, 9. Donabedian A. Evaluating the quality of medical care. Milwe will not know what these interventions are. bank Mem Fund Q 1966;44:Suppl:166-206. 10. Pronovost PJ, Miller MR, Wachter RM. Tracking progress in The movement to improve quality and safety patient safety: an elusive target. JAMA 2006;296:696-9. has achieved substantial momentum in recent 11. Hofer TP, Kerr EA, Hayward RA. What is an error? Eff Clin years and has begun to address the many errors Pract 2000;3:261-9. 12. Gaba DM, Howard SK. Patient safety: fatigue among cliniof omission and commission that harm patients cians and the safety of patients. N Engl J Med 2002;347:1249-55. each day. Moreover, the visible moral leadership 13. Weinger MB, Ancoli-Israel S. Sleep deprivation and clinical associated with these efforts3 has played a crucial performance. JAMA 2002;287:955-7. 14. Fletcher KE, Davis SQ, Underwood W, Mangrulkar RS, Mcrole in maintaining public trust. Although the Mahon LF Jr, Saint S. Systematic review: effects of resident work scope of the problems may seem to favor action hours on patient safety. Ann Intern Med 2004;141:851-7. over knowledge, quality improvement is on com- 15. Laine C, Goldman L, Soukup JR, Hayes JG. The impact of a regulation restricting medical house staff working hours on the mon ground with the rest of biomedicine. The quality of patient care. JAMA 1993;269:374-8. temptation is to circumvent traditional models 16. Shetty KD, Bhattacharya J. Changes in hospital mortality asof evidence when it comes to quality improve- sociated with residency work-hour regulations. Ann Intern Med 2007;147:73-80. ment, but this temptation has always existed in 17. Horwitz LI, Kosiborod M, Lin Z, Krumholz HM. Changes in medicine for those seeking cures to conditions outcomes for internal medicine inpatients after work-hour reguwith high morbidity. Just as in the rest of medi- lations. Ann Intern Med 2007;147:97-103. 18. Goldman L, Fiebach N. Hippocrates affirmed? Limiting cine, we must pursue the solutions to quality and residents’ work hours does no harm to patients. Ann Intern Med safety problems in a way that does not blind us 2007;147:143-4. 612 n engl j med 357;6  www.nejm.org  august 9, 2007 sounding Board 19. Nuckols TK, Escarce JJ. Residency work-hours reform: a cost analysis including preventable adverse events. J Gen Intern Med 2005;20:873-8. 20. Landon BE, Hicks LS, O’Malley AJ, et al. Improving the management of chronic disease at community health centers. N Engl J Med 2007;356:921-34. 21. Landon BE, Wilson IB, McInnes K, et al. Effects of a quality improvement collaborative on the outcome of care of patients with HIV infection: the EQHIV study. Ann Intern Med 2004; 140:887-96. 22. Wachter RM, Pronovost PJ. The 100,000 Lives Campaign: a scientific and policy review. Jt Comm J Qual Patient Saf 2006; 32:621-7. 23. Mittman BS. Creating the evidence base for quality improvement collaboratives. Ann Intern Med 2004;140:897-901. 24. Shojania KG, Ranji SR, McDonald KM, et al. Effects of quality improvement strategies for type 2 diabetes on glycemic control: a meta-regression analysis. JAMA 2006;296:427-40. 25. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA 2005;293:1197-203. 26. Han YY, Carcillo JA, Venkataraman ST, et al. Unexpected increased mortality after implementation of a commercially sold computerized physician order entry system. Pediatrics 2005;116: 1506-12. [Erratum, Pediatrics 2006;117:594.] 27. Patterson ES, Cook RI, Render ML. Improving patient safety by identifying side effects from introducing bar coding in medication administration. J Am Med Inform Assoc 2002;9:540-53. 28. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA 2003;290:1899-905. 29. Merton RK. The unanticipated consequences of purposive social action. Am Sociol Rev 1936;1:894-904. 30. Perrow C. Normal accidents: living with high-risk technologies. New York: Basic Books, 1984. 31. Reason J. Managing the risks of organizational accidents. Burlington, VT: Ashgate Publishing, 1997. 32. Shojania KG, Grimshaw JM. Evidence-based quality improvement: the state of the science. Health Aff (Millwood) 2005; 24:138-50. 33. Denrell J. Selection bias and the perils of benchmarking. Harvard Business Review. April 2005:114-9, 134. 34. Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials. BMJ 2003;327:1459-61. 35. Gawande A. On washing hands. N Engl J Med 2004;350: 1283-6. 36. Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharma- cist counseling in preventing adverse drug events after hospitalization. Arch Intern Med 2006;166:565-71. 37. Bristow PJ, Hillman KM, Chey T, et al. Rates of in-hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team. Med J Aust 2000;173:236-40. 38. Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ 2002;324:387-90. 39. Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Care Med 2004;32:91621. 40. DeVita MA, Braithwaite RS, Mahidhara R, Stuart S, Foraida M, Simmons RL. Use of medical emergency team responses to reduce hospital cardiopulmonary arrests. Qual Saf Health Care 2004;13:251-4. 41. Kerridge RK, Saul WP. The medical emergency team, evidence-based medicine and ethics. Med J Aust 2003;179:313-5. 42. Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091-7. [Erratum, Lancet 2005; 366:1164.] 43. Winters BD, Pham J, Pronovost PJ. Rapid response teams — walk, don’t run. JAMA 2006;296:1645-7. 44. Nielsen PE, Goldman MB, Mann S, et al. Effects of teamwork training on adverse outcomes and process of care in labor and delivery: a randomized controlled trial. Obstet Gynecol 2007;109:48-55. 45. Berwick DM. Broadening the view of evidence-based medicine. Qual Saf Health Care 2005;14:315-6. 46. Glasziou P, Chalmers I, Rawlins M, McCulloch P. When are randomised trials unnecessary? Picking signal from noise. BMJ 2007;334:349-51. 47. Bradley EH, Herrin J, Wang Y, et al. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med 2006;355:2308-20. 48. Benson K, Hartz AJ. A comparison of observational studies and randomized, controlled trials. N Engl J Med 2000;342:187886. 49. Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med 2000;342:1887-92. Copyright В© 2007 Massachusetts Medical Society. n engl j med 357;6  www.nejm.org  august 9, 2007 613 The n e w e ng l a n d j o u r na l of m e dic i n e c or r e sp ondence Adjunctive Antidepressant Treatment for Bipolar Depression To the Editor: Sachs et al. (April 26 issue)1 report that adding an adjunctive antidepressant drug offers no benefit over continued mood-stabilizer monotherapy in the treatment of bipolar depression. This finding contradicts some previous studies and the experience of many clinicians. In his thoughtful accompanying editorial, Belmaker2 identifies possible reasons for this discrepancy, including diagnostic heterogeneity and changes in the manifestation of bipolar disorder during the past 20 years. These observations are perhaps too circumspect. The past two decades have seen a marked increase in the diagnosis of bipolar disorder by North American psychiatrists.3 This trend has many origins: a reaction to past underdiagnosis, a belief that this disorder is more treatable and less stigmatizing than some alternative diagnoses, and an insufficiently critical application of the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), as well as a genuine conviction on the part of some authorities that this is indeed a widely prevalent condition.4 More recently, direct-to-consumer advertising by pharmaceutical companies has exacthis week’s letters 614 614 Adjunctive Treatment for Bipolar Depression 616 Glucose Regulation in Young Adults with Very Low Birth Weight 617 Use of Physicians’ Services for Medicare Beneficiaries 619 Video on Orotracheal Intubation 621 A Man with Swelling of Both Eyes and an Ear 622 Pregnancy in Congenital ВErythropoietic Porphyria erbated the trend. To the extent that the diagnostic boundaries of bipolar disorder are allowed to expand, the benefits of specific pharmacologic treatments are likely to decline. Lawrence H. Price, M.D. Audrey R. Tyrka, M.D., Ph.D. Butler Hospital Providence, RI 02906 lawrence_price_md@brown.edu Dr. Price reports receiving lecture fees from AstraZeneca. No other potential conflict of interest relevant to this letter was reported. 1. Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression. N Engl J Med 2007;356:1711-22. 2. Belmaker RH. Treatment of bipolar depression. N Engl J Med 2007;356:1771-3. 3. Patten SB. Does almost everybody suffer from a bipolar disorder? Can J Psychiatry 2006;51:6-8. 4. Akiskal HS. Validating вЂ�hard’ and вЂ�soft’ phenotypes within the bipolar spectrum: continuity or discontinuity? J Affect Disord 2003;73:1-5. To the Editor: Sachs et al. do not consider the heterogeneity of bipolar depression, concluding that adding antidepressants to mood stabilizers for patients with this condition is not effective. This finding, which contradicts the results of previous studies,1 could lead to possible deleterious consequences for patients. As suggested in the editorial by Belmaker, the low recruitment rate (366 of 2689 patients with at least one major depressive episode) may reflect a selection bias. There is considerable clinical heterogeneity in bipolar depression.2 It is possible to distinguish two types of bipolar depression, one characterized by a global inhibition and the other by activation features.3 Inhibited depressions appear to share common mechanisms with unipolar depression,4 and failing to treat such conditions with antidepressant drugs may increase the risk of suicide. Activated depressions are closer to mixed states and may be worsened by antidepressants. This differential response to treatment may n engl j med 357;6  www.nejm.org  august 9, 2007 correspondence account for the lack of efficacy of antidepressants reported in the study by Sachs et al., which did not assess heterogeneity. Chantal Henry, M.D., Ph.D. University Bordeaux 2 33076 Bordeaux, France chenry@ch-perrens.fr Jacques Demotes-Mainard, M.D., Ph.D. INSERM-ECRIN 75013 Paris, France Marion Leboyer, M.D., Ph.D. INSERM UnitГ© 841 94000 CrГ©teil, France 1. Gijsman HJ, Geddes JR, Rendell JM, Nolen WA, Goodwin GM. Antidepressants for bipolar depression: a systematic review of randomized, controlled trials. Am J Psychiatry 2004;161: 1537-47. 2. Benazzi F. Bipolar disorder — focus on bipolar II disorder and mixed depression. Lancet 2007;369:935-45. 3. Henry C, M’BaГЇlara K, Poinsot R, et al. Evidence for two types of bipolar depression using a dimensional approach. Psychother Psychosom (in press). 4. Oquendo MA, Hastings RS, Huang Y-Y, et al. Brain serotonin transporter binding in depressed patients with bipolar disorder using positron emission tomography. Arch Gen Psychiatry 2007; 64:201-8. To the Editor: The trial by Sachs and colleagues is the latest in a string of studies showing that the addition of antidepressants to mood stabilizers in depressed bipolar patients is of minimal benefit.1,2 However, antidepressants given in the absence of a mood stabilizer — either alone (in type II illness)3,4 or added to a second-generation antipsychotic drug5 — are effective in treating bipolar depression. The major difference in the design of these studies is the absence or presence of mood stabilizers. When mood stabilizers (lithium or valproate, carbamazepine, or lamotrigine) are used, antidepressants are of minimal benefit. This finding has traditionally been interpreted as showing that mood stabilizers have an intrinsic antidepressant effect, which cannot be augmented by the antidepressant agent. An alternative interpretation that would reconcile the discrepant data is that mood stabilizers may actually interfere with or block the effect of antidepressant drugs. This distinction is important, since it would alter the approach to treating depression in patients with bipolar disorder. Studies that specifically examine this question need to be performed. Rif S. El-Mallakh, M.D. University of Louisville School of Medicine Louisville, KY 40202 rselma01@louisville.edu 1. Nemeroff CB, Evans DL, Gyulai L, et al. Double-blind, pla- cebo-controlled comparison of imipramine and paroxetine in the treatment of bipolar depression. Am J Psychiatry 2001;158: 906-12. 2. Post RM, Leverich GS, Nolen WA, et al. A re-evaluation of the role of antidepressants in the treatment of bipolar depression: data from the Stanley Foundation Bipolar Network. Bipolar Disord 2003;5:396-406. 3. Amsterdam J. Efficacy and safety of venlafaxine in treatment of bipolar II major depressive episode. J Clin Psychopharmacol 1998;18:414-7. 4. Amsterdam JD, Garcia-EspaГ±a F, Fawcett J, et al. Efficacy and safety of fluoxetine in treating bipolar II major depressive episode. J Clin Psychopharmacol 1998;18:435-40. 5. Tohen M, Vieta E, Calabrese J, et al. Efficacy of olanzapine and olanzapine-fluoxetine combination in the treatment of bipolar I depression. Arch Gen Psychiatry 2003;60:1079-88. [Erratum, Arch Gen Psychiatry 2004;61:176.] The authors reply: Price and Tyrka comment on several trends related to the diagnosis of bipolar disorder, which raise concerns we share. However, as we detailed in our article, the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) rigorously applied DSM-IV criteria both in the selection of subjects at initial entry into the program and for inclusion in the randomized study of acute depression. We do not believe our results necessarily contradict those of previous studies. Instead, we suggest that our conclusions differ from those of previous studies largely because in our study, durable recovery was the primary outcome variable. As we stated, the results of our cross-sectional, last-observation-carriedforward analyses, as typically applied in most previous studies of short-term treatment, revealed a proportion of subjects treated with antidepressants who had rates of successful outcome similar to those reported in previous studies. However, mood stabilizers alone provided an equivalent benefit in the depressed subjects with bipolar disorder whom we studied. Dr. Henry and colleagues raise the issue of heterogeneity and suggest a differential response on the basis of two principal subtypes of depression in bipolar disorder: global inhibition and activation. Although their proposed typology is potentially interesting, the existence of such heterogeneity is unlikely to account for the absence of difference between study groups in our randomized study. Notably, no increase in suicidality was observed in subjects treated without standard antidepressants. STEP-BD does plan to examine symptom profiles obtained at baseline as predictors of treatment outcome. Dr. El-Mallakh makes a scientific point that cannot be adequately resolved currently. Treating n engl j med 357;6  www.nejm.org  august 9, 2007 615 The n e w e ng l a n d j o u r na l acute bipolar depression for short periods with antidepressants alone could result in higher response rates than the use of antidepressants in combination with mood stabilizers. However, a blinded maintenance study1 reported lower response rates when patients with bipolar disorder who were receiving placebo under double-blind conditions became depressed and received adjunctive antidepressants, as compared with the response rates observed when the antidepressants were added to mood stabilizers in a blinded fashion. To our knowledge, no published study has had design features that directly address Dr. ElMallakh’s supposition, which requires that patients be randomly assigned to receive antidepressants in combination with a mood stabilizer or as monotherapy. Since evidence-based treatment guidelines consistently recommend the concurrent use of a mood stabilizer, it is likely that ethical concerns, as well as concerns about practical complexities and study costs, account for the lack of such initiatives. Dr. Belmaker’s concern about limited generalizability and low recruitment rates in our study requires some clarification. Unlike most clinical of m e dic i n e trials, STEP-BD enrolled a large number of patients with bipolar disorder who were seeking treatment. However, the relatively low percentage of depressed patients who underwent randomization reflected the large number of patients who were ineligible owing to previous treatment with both bupropion and paroxetine, an unwillingness to accept treatment with approved mood stabilizers, or an unwillingness to taper the dose of a current antidepressant medication. However, we acknowledge that results from our study may not apply to all antidepressants, since our study examined only bupropion and paroxetine. Gary S. Sachs, M.D. Harvard Medical School Boston, MA 02115 Charles Bowden, M.D. University of Texas Health Science Center San Antonio, TX 78229-3900 Michael E. Thase, M.D. University of Pennsylvania Philadelphia, PA 19104 1. Gyulai L, Bowden CL, McElroy SL, et al. Maintenance effi- cacy of divalproex in the prevention of bipolar depression. Neuropsychopharmacology 2003;28:1374-82. Glucose Regulation in Young Adults with Very Low Birth Weight To the Editor: Hovi et al. (May 17 issue)1 report that young adults who had a very low birth weight have higher indexes of glucose intolerance and higher blood pressure than do those who were born at term. Although the authors report that maternal preeclampsia occurred significantly more frequently in the very-low-birth-weight group (35 of 166) than in the term group (13 of 172, P<0.001), they did not adjust their comparisons for this variable. In our tertiary neonatal intensive care unit in an urban area in northern Italy, from 2000 to 2006, glucose intolerance (fasting glucose level, >215 mg per deciliter)2 was recorded in 74 of 469 neonates with a very low birth weight. Hyperglycemia occurred in 22 of 92 (23.9%) of those with a history of maternal preeclampsia,3 as compared with 52 of 377 (13.8%) without maternal preeclampsia (95% confidence interval [CI], 1.12 to 3.44; P = 0.02). Preeclampsia and insulin resistance may be associated in pregnant women,4 putting stress on the fetus and causing the onset of fetal hormonal 616 responses, possibly involving blood pressure and glucose regulation. Since circumstances during the fetal period may have lifelong programming effects on various body functions and susceptibility to disease, our data suggest that preeclampsia — rather than very low birth weight itself — might account for early disturbances in glucose regulation. Paolo Manzoni, M.D. Maria Grazia BaГ№, M.D. Daniele Farina, M.D. Sant’Anna Obstetrics and Neonatology Hospital 10126 Turin, Italy paolomanzoni@hotmail.com 1. Hovi P, Andersson S, Eriksson JG, et al. Glucose regulation in young adults with very low birth weight. N Engl J Med 2007; 356:2053-63. 2. Cowett RM, Farrag HM. Selected principles of perinatalneonatal glucose metabolism. Semin Neonatol 2004;9:37-47. 3. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy. Am J Obstet Gynecol 2000;183:S1-S22. 4. Montoro MN, Kjos SL, Chandler M, Peters RK, Xiang AH, Buchanan TA. Insulin resistance and preeclampsia in gestational diabetes mellitus. Diabetes Care 2005;28:1995-2000. n engl j med 357;6  www.nejm.org  august 9, 2007 correspondence The authors reply: Manzoni et al. raise the important issue of maternal preeclampsia, which is a frequent reason for prematurity. Previous reports suggest that offspring of mothers with preeclampsia have higher-than-normal blood pressure in childhood1 and impaired glucose regulation in adulthood.2 In our study, we decided not to preВ sent results adjusted for preeclampsia because such an adjustment would not have altered the results. We here present numerical data to support this decision. Young adults born to mothers with preeclampsia had glucose and insulin concentrations similar to those of the rest of the subjects. However, their systolic blood pressure was increased by 3.8 mm Hg (95% CI, 0.2 to 7.4). After adjustment for preeclampsia, very low birth weight was associated with an increase in the fasting insulin level of 16.7% (95% CI, 4.2 to 30.6), an increase in the 2-hour glucose level of 6.4% (95% CI, 0.3 to 12.7), and an increase in systolic blood pressure of 4.4 mm Hg (95% CI, 1.7 to 7.1). These estimates are similar to those we reported without adjustment for preeclampsia. Also, when we excluded subjects with a history of maternal preeclampsia, the effects of very low birth weight remained similar and statistically significant. Therefore, we conclude that maternal preeclampsia did not explain the association of very low birth weight with impaired glucose regulation and higher blood pressure. Petteri Hovi, M.D. National Public Health Institute FI-00300 Helsinki, Finland Sture Andersson, M.D., Ph.D. Hospital for Children and Adolescents FI-00029 HUS Helsinki, Finland Eero Kajantie, M.D., Ph.D. National Public Health Institute FI-00300 Helsinki, Finland 1. Tenhola S, Rahiala E, Martikainen A, Halonen P, Voutilainen R. Blood pressure, serum lipids, fasting insulin, and adrenal hormones in 12-year-old children born with maternal preeclampsia. J Clin Endocrinol Metab 2003;88:1217-22. 2. Thomas C, HyppГ¶nen E, Power C. Prenatal exposures and glucose metabolism in adulthood: are effects mediated through birth weight and adiposity? Diabetes Care 2007;30:918-24. Use of Physicians’ Services for Medicare Beneficiaries To the Editor: The Specialty Society Relative Value Update Committee of the American Medical Association (AMA) has two primary concerns regarding the article by Maxwell et al. (May 3 issue).1 First, we are unable to reconcile the data in Table 1 of the article with our recommendations in this time period. For example, our recommendations for “tests” represent a 2% increase, not a 68% increase, as asserted in the article. Second, the authors did not consider major changes from the most recent 5-year review of the resourcebased relative-value scale. A comparison of 1992 and 2007 work relative-value units (RVUs), with the 2005 utilization data used as a common multiplier, reveals that evaluation and management work valuation has increased 45%, while imaging work valuation has decreased 6% since 1992. We question the appropriateness of excluding the most significant change and subsequent redistribution since the inception of the resourcebased relative-value scale — the revaluation of evaluation and management services in 2007. We agree that the scale’s improvements should be ongoing, and we have submitted to the Centers for Medicare and Medicaid Services (CMS) a number of significant recommendations related to the practice-expense payments for consideration in the 2008 Medicare resource-based relative-value scale. William L. Rich, III, M.D. American Medical Association Chicago, IL 60610 1. Maxwell S, Zuckerman S, Berenson RA. Use of physicians’ services under Medicare’s resource-based payments. N Engl J Med 2007;356:1853-61. To the Editor: Maxwell et al. analyzed the effect of the resource-based relative-value scale, reporting that the share of Medicare total RVUs for evaluation and management services did not change between 1992 and 2002. In an accompanying editorial, Newhouse describes concerns about potential underpayment for these services.1 My colleagues and I believe the Berenson– Eggers Type of Service (BETOS) classification used by Maxwell et al. does not provide sufficiently accurate clinical-service-group delineation. For example, the BETOS evaluation and management n engl j med 357;6  www.nejm.org  august 9, 2007 617 The n e w e ng l a n d j o u r na l of m e dic i n e Table 1. Effect of the Resource-Based Relative-Value Scale on Evaluation and Management Services and Major Procedures, 1992–2002. Service Category Average Allowed RVUs per Service 1992 2002 no. Change Average Annual Allowed RVU per Beneficiary Average Allowed Charge per Service Average Annual Allowed Charges per Beneficiary 1992 1992 1992 % 2002 no. Change % 2002 $ Change % 2002 $ Change % Evaluation and management 1.22 1.76 +44 11.10 17.45 +57 39 64 +64 355 632 +78 Major procedures 21.27 16.76 в€’21 6.74 5.11 в€’24 681 607 в€’11 216 185 в€’14 category includes pathology services, and the BETOS major procedures category excludes highvolume surgical procedures such as cataract extractions. We analyzed Medicare data files during the same period, defining evaluation and management services as office, hospital, emergency-department, and nursing-facility services and home visits, plus consultations and critical care. Major procedures were defined as surgery with 90-day global periods. With the use of more refined service assignments, we identified dramatic growth in evaluation and management RVUs and payments, both per service and per beneficiary (Table 1); this growth was not shown by the proportional analysis of Maxwell et al. In addition, we identified large reductions in payments for major procedures that were not noted by Maxwell and colleagues. An analysis of data from recent years is necessary to define the current effect of the resource-based relative-value scale. Thomas R. Russell, M.D. American College of Surgeons Chicago, IL 60611 1. Newhouse JP. Medicare spending on physicians — no easy fix in sight. N Engl J Med 2007;356:1883-4. To the Editor: The article by Maxwell and colleagues is a welcome addition to the literature on Medicare’s resource-based relative-value scale payment system. Using similar methods, we likewise found that the increase in the volume and intensity mix of physician services was the largest source of growth over the first 5 years of this system.1 In addition, we found that, at most, half of the growth in volume and intensity was due to demographic factors such as the aging of the population, selective enrollment of healthier beneficiaries in managed-care plans, and changes in the prevalence of health conditions. Also, increases in service use were surprisingly uniform 618 across conditions, indicating that technological advances and changing standards of care are affecting most categories of patients. This finding poses difficult challenges to policymakers seeking to control Medicare spending. Melinda B. Buntin, Ph.D. Jose J. Escarce, M.D., Ph.D. Dana Goldman, Ph.D. RAND Santa Monica, CA 90407 buntin@rand.org 1. Buntin MJB, EscarcГ© JJ, Goldman D, Kan H, Laugesen MJ, Shekelle P. Increased Medicare expenditures for physicians’ services: what are the causes? Inquiry 2004;41:83-94. The Authors Reply: We agree with Rich that the most recent 5-year review of the resource-based relative-value scale is relevant to our findings. Data from this review were not available to us during our study. We discuss this review in our article, noting the increases in work RVUs of selected evaluation and management services and factors that diluted the effect of those increases in terms of actual payments to physicians.1 Rich reports that on the basis of a comparison of 1992 and 2007 RVUs, with 2005 utilization data used as a common multiplier, tests reviewed by the Specialty Society Relative Value Update Committee of the AMA resulted in an estimated 2% increase in work volume. Since this is lower than our estimate, we reviewed our data and found that the discrepancy arose from four test codes that were incorrectly categorized in the RVU files provided to us. These tests had low 1992 work volumes and high 2002 work volumes, which resulted in an overestimation of growth due to RVU revisions and an underestimation of growth due to service quantity and mix. When we applied the calculation to the corrected data file, we found an increase of 11% in work volume for all tests due to RVU revisions from the 5-year review and annual revision processes. Be- n engl j med 357;6  www.nejm.org  august 9, 2007 correspondence cause tests are less than 3% of work volume, this change had a very limited effect on our other findings. Russell questions the BETOS classification2 and finds different results when the service groupings of the American College of Surgeons are used. BETOS is used by the CMS, the Medicare Payment Advisory Commission, and many health services researchers as the standard classification system for physicians’ services. On the basis of an examination of only surgical procedures with 90-day global periods, Russell reports declines in total RVUs and charges per beneficiary. Our study also showed declines in the total volume for some groups within the major procedures category. Russell found higher increases in work volume when the cognitive services of some specialists were removed from the evaluation and management category. Excluding those services, we also find higher increases in work volume among the remaining services in this BETOS category. The study by Buntin and colleagues provided a valuable early analysis of the sources of growth in expenditures for physicians’ services during the 5 years after implementation of the physician fee schedule.3 They used the Medicare Current Beneficiary Survey, which permitted them to conduct a detailed investigation of beneficiary health status and sociodemographic factors as sources of expenditure growth. Stephanie Maxwell, Ph.D. Stephen Zuckerman, Ph.D. Robert A. Berenson, M.D. Urban Institute Washington, DC 20037 1. Centers for Medicare & Medicaid Services. Medicare pro- gram: five-year review of work relative value units under the physician fee schedule and proposed changes to the practice expense methodology: notice. Fed Regist 2006;71(125):37255. 2. Idem. Berenson-Eggers Type of Service (BETOS). (Accessed July 19, 2007, at http://www.cms.hhs.gov/HCPCSReleaseCodeSets/ 20_BETOS.asp.) 3. Buntin MJB, EscarcГ© JJ, Goldman D, Kan H, Laugesen MJ, Shekelle P. Increased Medicare expenditures for physicians’ services: what are the causes? Inquiry 2004;41:83-94. Video on Orotracheal Intubation To the Editor: In the Video in Clinical Medicine about orotracheal intubation, presented by Kabrhel et al. (April 26 issue),1 the authors state that the “combination of flexion of the neck and extension of the head [the sniffing position] improves the alignment of the axes of the oral cavity, pharynx, and larynx, facilitating optimal visualization of the vocal cords.” This is an anatomical myth that is not supported by clinical evidence.2 In a randomized crossover study of 456 consecutive patients, Adnet et al.3 found no differences in glottic visualization by direct laryngoscopy or in the score on the intubation-difficulty scale between the use of simple head extension and routine sniffing position. Furthermore, in 11% of patients, glottic exposure was lessened with the use of the “three axes alignment.” However, a multivariable analysis showed that reduced neck mobility and obesity were independently related to improvement in the laryngoscopic view with the use of the sniffing position.3 These results are consistent with studies of other populations4 and with anatomical studies involving magnetic resonance imaging.5 In conclusion, routine use of the sniffing position should not be a standard procedure in orotracheal intubation. David A. RincГіn, M.D. Universidad Nacional de Colombia BogotГЎ 11001000, Colombia darinconv@unal.edu.co 1. Kabrhel C, Thomsen TW, Setnik GS, Walls RM. Orotracheal intubation. N Engl J Med 2007;356:e15 (Web only). (Available at http://content.nejm.org/cgi/content/full/356/17/e15.) [Erratum, N Engl J Med 2007;356:2228.] 2. Adnet F, Borron SW, Lapostolle F, Lapandry C. The three axis alignment theory and the “sniffing position”: perpetuation of an anatomic myth? Anesthesiology 1999;91:1964-5. 3. Adnet F, Baillard C, Borron SW, et al. Randomized study comparing the “sniffing position” with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology 2001;95:836-41. 4. Collins JS, Lemmens HJM, Brodsky JB, Brock-Utne JG, Levitan RM. Laryngoscopy and morbid obesity: a comparison of the “sniff” and “ramped” positions. Obes Surg 2004;14:1171-5. 5. Adnet F, Borron SW, Dumas JL, Lapostolle F, Cupa M, Lapandry C. Study of the “sniffing position” by magnetic resonance imaging. Anesthesiology 2001;94:83-6. To the Editor: In their video on orotracheal intubation, Kabrhel et al. suggest that neuromuscular-blocking agents and sedatives will “prevent the patient from vomiting.” Readers should not be comforted that the use of these agents will prevent emesis. Etomidate, the medication mentioned in the video, is known to be emetogenic and has been shown to be associated with emesis n engl j med 357;6  www.nejm.org  august 9, 2007 619 The n e w e ng l a n d j o u r na l of m e dic i n e during intubation.1 In addition, we were disappointed that there was no mention of the difficult-airway algorithm of the American Society of Anesthesiologists, an evidence-based practice guideline on this important topic that has guided airway management for 15 years.2 Sachin Kheterpal, M.D. George A. Mashour, M.D., Ph.D. sure on the cricoid cartilage during emergency intubation (the Sellick maneuver), even though this maneuver is not always used. The usefulness of cricoid pressure in preventing aspiration has never been proved, and there is ample literature on both sides of the issue. What is not in doubt is that abnormally applied cricoid pressure can lead to partial or complete obstruction of the airway, making ventilation and intubation difficult University of Michigan Ann Arbor, MI 48109 or impossible. Also not in doubt is the fact that sachinkh@med.umich.edu very few practitioners know where the cricoid 1. Bozeman WP, Young S. Etomidate as a sole agent for endo- cartilage is and how to hold 30 N of pressure. tracheal intubation in the prehospital air medical setting. Air One other indisputable fact is that aspiration, Med J 2002;21:32-7. 2. Practice guidelines for management of the difficult airway: though potentially fatal, is very rare if intubation an updated report by the American Society of Anesthesiologists is performed correctly. Thus, I would recommend Task Force on Management of the Difficult Airway. Anesthesiolthat the emphasis on the Sellick maneuver be ogy 2003;98:1269-77. [Erratum, Anesthesiology 2004;101:565.] completely removed from this video, since it is more likely to cause harm than good if the perTo the Editor: Kabrhel et al. recommend use of son performing the intubation is inexperienced. a carbon dioxide detector to confirm the place- Nir Hoftman, M.D. ment of the endotracheal tube. Furthermore, they University of California, Los Angeles suggest that the device be used to detect carbon Los Angeles, CA 90049 dioxide consistently within the first six breaths after intubation and during subsequent breaths. The Authors Reply: The concise format of proThey caution that false negative results with re- cedural videos, such as ours, limits what can be gard to tube placement may occur in patients in addressed. Though the sniffing position is the cardiac arrest, in whom carbon dioxide may not most commonly recommended position to facilibe present in the lungs. tate orotracheal intubation and is considered the It would have been relevant to point out the standard of care,1 its usefulness has been debatpossibility of color change in the device due to ed. The crossover study cited by Dr. RincГіn comagents other than exhaled carbon dioxide. Gastric pared the sniffing position with head extension contents, mucus, and drugs such as epinephrine but not with neutral position.1 Considering the can cause false positive results.1,2 It is imperative study design, it is somewhat misleading to focus that clinicians using these devices be aware of only on the 11% of patients in whom neck extenthis limitation. One way to avoid this pitfall is to sion alone provided better glottic exposure withobserve the change in color in the device with out mentioning the 18% of patients in whom the each breath. A false positive result causes a per- sniffing position provided a better view. Studies manent color change in the device; hence, the have demonstrated an improved laryngoscopic color does not vary with ventilation. view with head elevation as compared with neutral position.2 However, we agree that for most Venkatesh Srinivasa, M.D. patients, the benefit of the sniffing position is VA Boston Healthcare System West Roxbury, MA 02132 probably conferred by the head extension it provenkatesh.srinivasa@va.gov vides. As such, we do not find a strong reason to Bhavani Shankar Kodali, M.D. abandon a long-standing practice, and we agree Brigham and Women’s Hospital with Adnet et al.,1 who state that their study is Boston, MA 02115 “less an indictment of the sniffing position than 1. Brackney SM, Nellcor Puritan Bennett. Caution when using reinforcement of the importance of head extencolorimetry to confirm endotracheal intubation. Anesth Analg sion in all patients.” 2007;104:738-9. We agree with Drs. Kheterpal and Mashour 2. Srinivasa V, Kodali BS. Caution when using colorimetry to confirm endotracheal intubation. Anesth Analg 2007;104:738. that the difficult-airway algorithm of the American Society of Anesthesiologists is a very useful To the Editor: The video on orotracheal intuba- guide. However, it is perhaps most applicable to tion places special emphasis on the use of pres- the planning of operating-room cases and is less 620 n engl j med 357;6  www.nejm.org  august 9, 2007 correspondence helpful when intubation is emergent or unavoidable. They are correct in stating that etomidate can cause emesis, but this is not an issue when neuromuscular-blocking agents are also used. Unfortunately, detailed discussions of the American Society of Anesthesiologists algorithm and pharmaceutical adjuncts were beyond the scope of our video. We also agree with Drs. Srinivasa and Kodali that during assessment of end-tidal carbon dioxide levels, the detector should be free of foreign material (e.g., vomit, mucus, or drugs) and that the color should vary during the respiratory cycle. Regarding Dr. Hoftman’s comments: we acknowledge in the text accompanying the video that cricoid pressure can distort the airway and that the benefit of decreased aspiration is theoretical. The maneuver is also frequently performed improperly. Although the evidence is mixed as to whether cricoid pressure improves or degrades intubating conditions, surveys show that it is al- most universally performed,3 so we thought it best to describe the technique. No doubt, future studies will clarify the precise role, if any, for this maneuver. Christopher Kabrhel, M.D. Massachusetts General Hospital Boston, MA 02114 Todd W. Thomsen, M.D. Mount Auburn Hospital Cambridge, MA 02138 Ron Walls, M.D. Brigham and Women’s Hospital Boston, MA 02115 1. Adnet F, Baillard C, Borron SW, et al. Randomized study comparing the “sniffing position” with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology 2001;95:836-41. 2. Levitan RM, Mechem CC, Ochroch EA, Shofer FS, Hollander JE. Head-elevated laryngoscopy position: improving laryngeal exposure during laryngoscopy by increasing head elevation. Ann Emerg Med 2003;41:322-30. 3. Morris J, Cook TM. Rapid sequence induction: a national survey of practice. Anaesthesia 2001;56:1090-7. Case 14-2007: A Man with Pain and Swelling of Both Eyes and the Right Ear To the Editor: In the Case Record of a man with fever and pain and swelling of both eyes and the right ear, presented by Butterton and colleagues (May 10 issue),1 the right ear is described as “tender, with erythema of the external canal involving the preauricular and postauricular soft tissue and pinna.” This is repeated in the discussion. The point that is not emphasized but should be is that, although the external ear was inflamed, the earlobe was spared. This is evident even in the clinical photograph. Sparing of the earlobe is in itself diagnostic of polychondritis.2,3 This clinical feature alone helps in differentiating the case from other conditions such as cellulitis or malignant otitis externa, in which the earlobe is also inflamed.2 The earlobe is spared in polychondritis because it is devoid of cartilage, and only cartilaginous structures are involved. Therefore, while one is evaluating a patient for red ear, it is pertinent to look specifically for inflammation of the earlobe, the absence of involvement of which is diagnostic of polychondritis. However, under certain circumstances, leprosy, leishmaniasis, frostbite, and trauma can be considered in the differential diagnosis of auricular chondritis.2,3 Sandeep Chauhan, M.D. Government Medical College & Hospital Chandigarh 160030, India drsc88@rediffmail.com Vikas Agarwal, M.D., D.M. Sanjay Gandhi Postgraduate Institute of Medical Sciences Lucknow 226014, India Sanjay D’Cruz, M.D., D.M. Government Medical College & Hospital Chandigarh 160030, India 1. Case Records of the Massachusetts General Hospital (Case 14-2007). N Engl J Med 2007;356:1980-8. 2. Piette J-C, Vinceneux P. Relapsing polychondritis. In: Harris ED, Budd RC, Firestein GS, et al., eds. Kelley’s textbook of rheumatology. 7th ed. Philadelphia: Elsevier Saunders, 2005:1541-6. 3. Gilliland BC. Relapsing polychondritis. In: Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s principles of internal medicine. 16th ed. New York: McGraw-Hill, 2005:2015-6. The Discussants Reply: Chauhan et al. highlight the specificity of sparing of the earlobe in the diagnosis of relapsing polychondritis. In this case, the observation that swelling involved only the cartilaginous helix, and not the lobe, was not made until we first saw the patient on the fourth hospital day. Therefore, the text reflects how the n engl j med 357;6  www.nejm.org  august 9, 2007 621 The n e w e ng l a n d j o u r na l case was presented to us, with ambiguity as to which part of the ear was swollen. The sparing of the lobe is described at the end of the case history. We wanted to permit readers to make this observation on their own from Figure 1 of the article and to draw their own conclusions. The swelling of the helix with sparing of the earlobe, in the context of this patient’s history, led us immediately to the diagnosis of relapsing polychondritis and decreased our suspicion of infectious causes. We thus started corticosteroid treatment before the results of the biopsy were of m e dic i n e available and before this case met all the diagnostic criteria listed in Table 3 of the Case Record. However, we emphasize that there is no laboratory, radiographic, or physical finding that is pathognomonic of relapsing polychondritis. Auricular chondritis alone, even with sparing of the lobe, is not absolutely diagnostic of this disease. Deborah S. Collier, M.D. Joan R. Butterton, M.D. Massachusetts General Hospital Boston, MA 02114 Pregnancy in a Patient with Congenital Erythropoietic Porphyria To the Editor: Congenital erythropoietic porphyria, a rare autosomal recessive disorder of heme biosynthesis, results from markedly deficient uroporphyrinogen III synthase activity.1,2 Data regarding pregnancy in patients with this condition are lacking, which may be explained by the rarity of the disease, as well as social restrictions due to associated photosensitivity or disfiguring effects in more severely affected patients. We describe a successful pregnancy in a patient with congenital erythropoietic porphyria. The patient presented at 3 months of age with pink urine and severe photosensitivity; congenital erythropoietic porphyria was diagnosed on the basis of analysis of urinary, fecal, and blood porphyrin. Bone marrow transplantation, an established treatment option,3 was considered at the age of 18 months but was not pursued, owing to concerns about risks and the lack of a suitable donor. At the age of 9 years, in an attempt to suppress erythropoiesis and thus reduce the overproduction of porphyrin, hypertransfusion was initiated in combination with subcutaneous administration of deferoxamine but was discontinued because of its minimal efficacy. Analysis of the uroporphyrinogen III synthase gene identified Cys73в†’Arg and IVS8-23Aв†’G mutations, a combination previously described in a patient moderately affected with congenital erythropoietic porphyria.4 At 19 years of age, our patient became pregnant. There were no antenatal complications. The plasma porphyrin level increased during the second trimester and fell during the third trimester (Fig. 1), changes that were consistent with physi622 ologic changes in erythropoiesis and fluid balance during pregnancy.5 At 39 weeks of gestation, elective caesarean section for breech presentation was performed under dimmed lights with minimal exposure of the patient’s skin, without complication. A female infant with normal Apgar scores and birth weight of 3.52 kg was delivered. The plasma porphyrin level in the infant was 231 nmol per liter at the time of the birth (adult reference range, 0 to 11.2 nmol per liter) and decreased to 104 nmol per liter at 48 hours. No follow-up blood samples were available. Teeth erupted when the infant was 6 months of age; they showed distal brown pigmentation, with a sharply defined margin — consistent with porphyrin staining — where calcification had occurred before birth in association with exposure to maternal porphyrin (i.e., erythrodontia) (Fig. 2). This condition has been recognized in patients with congenital erythropoietic porphyria. The child has had normal development and no photosensitivity during 3 years of follow-up. The severity of congenital erythropoietic porphyria correlates with the degree of residual uroporphyrinogen III synthase activity, with more activity resulting in less severe disease.1,2 The patient’s early clinical presentation was assumed to indicate severe disease. In retrospect, the clinical course suggested a moderate clinical phenotype, confirmed by subsequent genotype studies. Cys73в†’Arg is the most frequently reported mutation in patients with congenital erythropoietic porphyria, accounting for one third of affected alleles,1,2 and leads to complete loss of function of uroporphyrinogen III synthase. In contrast, the n engl j med 357;6  www.nejm.org  august 9, 2007 Plasma Porphyrin Level (nmol/liter) correspondence congenital erythropoietic porphyria who are not severely affected may do well with conservative management and that successful pregnancy is possible in such patients. Nirmala Hallai, M.R.C.P. 4000 3000 Royal Hallamshire Hospital Sheffield S10 2JF, United Kingdom 2000 Alexander Anstey, F.R.C.P. 1000 Royal Gwent Hospital Newport NP20 2UB, United Kingdom 0 в€’18 12 20 23 28 31 33 38 Gestation (wk) Figure 1. Plasma Porphyrin Levels during Pregnancy. 1st AUTHOR: TheICM reference range Badminton is 0 to 11.2 nmol per RETAKE liter. On the x axis, indicates1 18 of 2weeks before conception; the2nd REGв€’18 F FIGURE: 3rd intervals between values vary. CASE Revised EMail Enon ARTIST: ts Line H/T Combo 4-C H/T SIZE 16p6 AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully. JOB: 35706 ISSUE: 08-09-07 Figure 2. Brown Staining of the Infant’s Teeth. IVS8-23Aв†’G mutation occurs at a branch point, and some function is retained.3 The present case indicates that patients with Shevaun Mendelsohn, F.R.C.P. John Williams, F.R.C.O.G. Gareth Evans-Jones, F.R.C.P.H. Sadia Malick, M.B., B.S. Countess of Chester Hospital Chester CH2 1UL, United Kingdom Michael N. Badminton, Ph.D., F.R.C.Path. Cardiff University Cardiff CF14 4XN, United Kingdom mike.badminton@cardiffandvale.wales.nhs.uk 1. Desnick RJ, Astrin KH. Congenital erythropoietic porphyria: advances in pathogenesis and treatment. Br J Haematol 2002;117:779-95. 2. De Verneuil H, Ged C, Moreau-Gaudry F. Congenital erythropoietic porphyria. In: Kadish KM, Smith KM, Guilard R, eds. The porphyrin handbook. Vol. 14. Medical aspects of porphyrins. San Diego, CA: Academic Press, 2003:43-63. 3. Tezcan I, Xu W, Gurgey A, et al. Congenital erythropoietic porphyria successfully treated by allogeneic bone marrow transplantation. Blood 1998;92:4053-8. 4. Fontanellas A, Bensidhoum M, Enriquez de Salamanca R, Moruno Tirado A, de Verneuil H, Ged C. A systematic analysis of the mutations of the uroporphyrinogen III synthase gene in congenital erythropoietic porphyria. Eur J Hum Genet 1996;4:27482. 5. Milman, Byg KE, Agger AO. Haemoglobin and erythrocyte indices during normal pregnancy and postpartum in 206 women with and without iron supplementation. Acta Obstet Gynecol Scand 2000;79:89-98. Correspondence Copyright В© 2007 Massachusetts Medical Society. instructions for letters to the editor Letters to the Editor are considered for publication, subject to editing and abridgment, provided they do not contain material that has been submitted or published elsewhere. Please note the following: •Letters in reference to a Journal article must not exceed 175 words (excluding references) and must be received within 3 weeks after publication of the article. Letters not related to a Journal article must not exceed 400 words. All letters must be submitted over the Internet at http://authors.nejm.org. •A letter can have no more than five references and one figure or table. •A letter can be signed by no more than three authors. •Financial associations or other possible conflicts of interest must be disclosed. (Such disclosures will be published with the letters. For authors of Journal articles who are responding to letters, this information appears in the published articles.) •Include your full mailing address, telephone number, fax number, and e-mail address with your letter. Our Web site: http://authors.nejm.org We cannot acknowledge receipt of your letter, but we will notify you when we have made a decision about publication. Letters that do not adhere to these instructions will not be considered. Rejected letters and figures will not be returned. We are unable to provide prepublication proofs. Submission of a letter constitutes permission for the Massachusetts Medical Society, its licensees, and its assignees to use it in the Journal’s various print and electronic publications and in collections, revisions, and any other form or medium. n engl j med 357;6  www.nejm.org  august 9, 2007 623 The n e w e ng l a n d j o u r na l of m e dic i n e b o ok r e v ie w s Preventing Medication Errors (Quality Chasm Series.) By the Committee on Identifying and Preventing Medication Errors and the Board on Health Care Services. Edited by Philip Aspden, Julie A. Wolcott, J. Lyle Bootman, and Linda R. Cronenwett. 463 pp. Washington, DC, National Academies Press, 2007. $54.95. ISBN 978-0-309-10147-9. Medication Errors Second edition. Edited by Michael R. Cohen. 680 pp., illustrated. Washington, DC, American Pharmacists Association, 2007. $89.95. ISBN 978-1-58212-092-8. H ealth care is inherently risky, and filling a handwritten prescription could be the most dangerous of all medical procedures. Medication errors, which are often caused by illegible handwriting, are a subgroup of medical errors and may cause as many as 7000 of the 98,000 deaths in the United States each year that the Institute of Medicine (IOM) attributes to medical errors. Now the IOM, in its new report in the Quality Chasm Series, Preventing Medication Errors, estimates that in the United States, the average hospital patient is subject to at least one medication error per day and that each year more than 1.5 million patients have injuries resulting from preventable adverse drug events. The new study covers the development of an evidence-based review of drug safety as well as guidelines for policymakers and government agencies. The IOM authorship committee (disclosure: two of its members are employees of Intermountain Healthcare) has clearly fulfilled its charge concerning prescription and over-the-counter drugs and complementary and alternative medications. However, the book has little practical advice for clinicians. Indeed, the major purpose of the committee was to recommend agendas for consumers, health care organizations, and the industries and regulatory agencies involved with drugs, medical devices, and health care information technology. I was surprised that the evidence for the most highly touted prevention strategies, such as computerized provider order entry, computer-based decision support systems, smart pumps, and bar coding, was reviewed only in the last appendix. The second edition of the book Medication Errors, edited by Michael R. Cohen, takes up where 624 the IOM report leaves off and complements it with detailed information that is useful for clinicians and clinical pharmacists. A pharmacist and the president of the nonprofit Institute for Safe Medication Practices (ISMP), Cohen has been a voice crying out in the wilderness for three deВ cades and was a 2005 recipient of a John D. and Catherine T. MacArthur Foundation “genius grant.” Cohen is coeditor of a widely read periodical published by the ISMP that focuses on “high-alert medications” and recent problems with particular drugs. He devised a method that uses “tall man” lettering to prevent errors in the use of drugs with look-alike, sound-alike names, and he also created a voluntary system for reporting errors, now called the United States Pharmacopeia– ISMP Medication Errors Reporting Program. Cohen’s ISMP proficiency tests have shown the inability of many pharmacy computer systems to detect unsafe and potentially fatal medication orders and have been an important impetus for the design of safer systems. Cohen defines a medication error as “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer.” This definition includes errors at any stage of medication use and not just during the process of drug administration. Cohen believes that the “five rights” of safe medication use (the right patient, right drug, right time, right dose, and right route of administration) place too much focus on individual performance and overlook the systemic problems that underlie the human errors. He emphasizes that “finding out who was involved is less important than learning what went wrong, how, and why.” The IOM report represents, so far as possible, a consensus of the committee and looks toward fundamental reforms in the health care system, including the pharmaceutical industries and regulatory agencies. In addition to systemic reforms, its authors mention some of the things that individual physicians, nurses, pharmacists, and caregivers can do to prevent errors. Cohen’s book, on the other hand, contains chapters by authorities from a variety of disciplines, several of whom n engl j med 357;6  www.nejm.org  august 9, 2007 — including Cohen — also contributed to the IOM report. Cohen’s book better describes specific medication errors and how to prevent them. The centerpiece is an excellent chapter on “highalert medications,” which Cohen defines as drugs with a high risk of causing patient injury or death if they are misused; the chapter includes a comprehensive table of safety measures for various drug classes. Many physicians who trained in the old days will be surprised to learn that there are good reasons for using trade names as well as generic names when prescribing certain medications, such as lipid-based amphotericin B products. Both books call for the elimination of handwritten prescriptions and for the use of electronic decision-support systems by prescribers and pharmacies by the year 2010. Yet the authors of both books also recognize that electronic prescribing is not a panacea. The IOM committee also calls for a gradual shift of the research agenda from defining incidence rates to prevention strategies and suggests a starting budget of $50 million to $100 million to fund these studies through the federal Agency for Healthcare Research and Quality. However, the committee does not further explain its rationale. Medication errors are a complex epidemiologic problem as well as a quality problem, and those who study such errors are saddled with a profusion of poorly defined concepts, such as “near miss,” “intercepted error,” and “potential adverse drug events.” The focus on errors has been useful because it draws attention to preventability. However, the definitions that have been used for various types of errors and adverse events vary widely, and the IOM committee calls for an international consensus conference to define terms. This effort is analogous to the methods used by intensivists to define the sepsis syndrome. Most medication errors, such as a missed dose, do not cause harm to patients, and conversely, most adverse drug events are not due to mistakes. In addition, certain types of adverse drug events that once were considered nonpreventable can now be ameliorated by intensive monitoring and early recognition — or even prevented entirely. For example, the failure to adjust the dose of a nephrotoxic antibiotic when a patient’s renal function declines would probably not precipitate an incident report to the voluntary reporting systems in most hospitals. Yet the number of these errors can be re- Example of a Potentially Fatal Computerized OrderEntry Error Intercepted by a Pharmacist. Mix-ups due to large differences in the dosages of conventional and liposomal amphotericin products have led to deaths. Courtesy of John Benson, Pharm.D. book reviews duced with the help of computer-based decisionsupport systems and electronic health records. Both of these books provide reviews of methods that are purported to increase drug safety, such as improved drug naming, labeling, and packaging; analysis of the root causes of important adverse drug events; failure mode and effects analysis of the processes of medication use; and voluntary reporting of important adverse events. The book by Cohen describes all these methods in greater depth than the IOM committee does. It also includes chapters that discuss how to disclose errors to patients and accounts of some of the emotional experiences of providers who have made fatal errors involving medication. These books with similar titles are authoritative, thorough, and well written. Both aim to improve drug safety and together represent the most up-to-date and broadest coverage of the subject now available. Both these books are fact-filled and visionary, but unfortunately, the benefits of many of the drug safety measures could have been better assessed and measured in the clinical setting. Nonetheless, the books might provoke varied responses from readers: frustration or despair because of the enormous gulf between what we do and what we know, admiration of what has been accomplished, and hope for the future. John P. Burke, M.D. LDS Hospital Salt Lake City, UT 84103 john.burke@intermountainmail.org n engl j med 357;6  www.nejm.org  august 9, 2007 625 The new england journal of medicine Medical Management of Vulnerable and Underserved Patients: Principles, Practice, and Populations Edited by Talmadge E. King, Jr., Margaret B. Wheeler, and Andrew B. Bindman, with four others. 454 pp., illustrated. New York, McGraw-Hill, 2007. $41.95. ISBN 978-0-07-144331-9. M any physicians consider the care of vulnerable and underserved patients to be an unsatisfying and often frustrating endeavor, but this new book offers an optimistic and evidence-based approach to the care of such patients. The editors define medically vulnerable populations as “those that are wounded by social forces placing them at a disadvantage for their health.” The book serves as an important reminder that many of the issues it raises are relevant to the broader landscape of American health care. The authors elicit the voice of the patient to explain and offer guidance on some of the difficult clinical and societal issues that physicians face in practice, including behavioral change, noncompliance, health literacy, health disparities, and the plight of the hidden poor. The book should become an essential primer for teachers, physiciansin-training, and practicing physicians because it offers important tools for teaching, critical concepts, common pitfalls, core competency concepts, and discussion questions for each chapter. A challenge for the editors and authors of this kind of book is to emphasize the importance of the physician’s own attitudes and practices toward vulnerable patients without being preachy. The editors’ decision to use the patient’s voice and a strong, evidence-based orientation helps them meet this challenge. The first part of the book, “Principles,” includes a chapter on the theoretical groundwork and context for understanding care of complex patients. There are also excellent reviews of disparities in health and health care and of the financing and organization of health care for vulnerable populations. Other chapters are excellent primers on legal and ethical principles and are written by respected leaders in the field. There is a remarkable focus on what health care providers and systems can actually do to improve care and reduce disparities. The chapters in the second section of the book, “Practice,” contain important insights on behavioral change, cross626 cultural communication, health literacy, home visits, group visits, interactive health technology, quality improvement, case management, and care in the context of community. The author of a superb chapter on cross-cultural communication emphasizes the importance of assessing one’s own values in order to improve care and communication. A chapter on behavioral change offers some practical tools to use with patients who have resistant behaviors in the context of cultural and financial pressures. The authors of the chapter on medication adherence make the case that this problem is not unique to vulnerable populations, and they offer some common-sense approaches. The chapter on limited health literacy should be required reading for all medical students and physicians. The role of interactive health technology in filling in safety-net gaps is emphasized, with real-life examples of how health information technology has been transformative in the care of vulnerable patients facing language and cultural divides. The third section of the book deals with a variety of vulnerable populations that need special consideration when they seek care. The chapters on many different population groups stand on their own and offer important lessons for the care of patients who often are not mentioned in standard medical textbooks. These groups include patients with a history of incarceration, patients with limited English proficiency, immigrants, patients with disabilities, patients who have been victims of domestic violence, patients with chronic pain, and patients with substance-abuse problems. The information is provided in a nonjudgmental manner on the basis of strong evidence and with practical guides for improving care. The chapters on immigrant health and language barriers offer useful guidance, such as advice on how to work with interpreters, that could help to bridge divides. The authors of chapter 20, “The Hidden Poor: Care of the Elderly,” emphasize functional assessment, elder abuse, and the limitations of prescription-drug coverage for the elderly. Several chapters in the third section serve to remind us to consider care in the context of family and community, such as chapter 19, “The Family as the Context for Care,” and chapter 38, “HIV/AIDS: Impact on Vulnerable Populations.” Chapter 40, “Caring for Oneself While Caring for Others,” offers important insights on reducing clinician burnout. n engl j med 357;6  www.nejm.org  august 9, 2007 book reviews This book is an ambitious and important contribution to the care of our most wounded patients. For those of us who regularly care for vulnerable patients, it provides an excellent resource and supportive guide. However, it should also become part of the standard library for all medical students and practicing physicians. All physicians have much to learn from the practical, evidencebased approaches to the societal issues we all face in practice. Ultimately, this is a book that could help all clinicians take better care of all patients, especially those who may need extra help and support as they navigate our complex health care system. Helen Burstin, M.D., M.P.H. National Quality Forum Washington, DC 20005 hburstin@qualityforum.org New and Evolving Infections of the 21st Century (Emerging Infectious Diseases of the 21st Century.) Edited by I.W. Fong and Ken Alibek. 375 pp., illustrated. New York, Springer, 2007. $129. ISBN 978-0-387-32647-4. I West Nile virus, a striking example of an established viral disease that after being transplanted to a new continent has adapted and expanded its dominion in North America. This chapter sets the stage by illustrating one of the central aspects of emerging infectious diseases — that most of them are naturally resident in animal populations and thus are of equal importance in the field of veterinary medicine. The events that culminate in the transition from an often unrecognized infection in a domestic or wild animal to a human disease are important to understand. Zoonotic diseases (those transmitted from animals to man) often have complex dynamics, occasionally leading to cross-species exposures and human infection; in some cases, a disease develops, and in even rarer cases, the disease is transmitted from human to human. Understanding the nature of these events is crucial in the prevention and control of future outbreaks. For instance, the backto-back chapters on hantaviruses and poxviruses include descriptions of the differences between genetically promiscuous RNA viruses and viruses with more conserved DNA genomes. These contrasting chapters serve as examples to illustrate the complexities that may give rise to clinically apparent zoonotic infections when they cross the species barrier into naive human populations. Numerous chapters in the book, including those on the severe acute respiratory syndrome and avian influenza, illustrate the shifting continuum between human medicine and veterinary medicine. The health problems these infections cause in both fields are comprehensively handled, and from the perspective of human disease and diagnosis are well presented. There are inherent weaknesses in a multiauthored book such as this one. Most chapters cover the spectrum, from virology and epidemiology to clinical presentation and management, but they differ greatly in strength and content. However, these shortcomings are outweighed by a good number of well-written, high-quality, comprehensive chapters. This book will be a useful and relatively current resource not only for experts and researchers in public health and infectious diseases but also for veterinary and medical professionals as well as graduate students. t is not a matter of if, but instead when, the next epidemic will strike. Historically, infectious diseases have inflicted much misery and, in so doing, have shaped humankind as we know it today. From past plagues, we not only have vestiges of older immunologic defenses but also still possess the genetic skeletons of some viral incursions into our genome. How will the next epidemic reveal itself, and where will it come from? This book is well timed, and it places perceived and real viral threats in perspective. The title of the book, New and Evolving Infections of the 21st Century, may seem prophetic, given that the first decade of this century has yet to run its course. Nevertheless, the book will be a valuable contribution to education and preparedness. Its editors have called on experts in infectious diseases of the very recent past to document and compile current and recent threats, while also providing examples of evolving insidious infections that in some cases are relatively common in our population. The book is divided into three sections: “Evolving Infectious Diseases,” “Newly Jonathan L. Heeney, D.V.M., D.V.Sc.(Path.), Ph.D. Recognized Human Viruses,” and “Emerging ViUniversity of Cambridge ruses in Asia.” Cambridge CB3 0ES, United Kingdom The first section begins with a chapter on jlh66@cam.ac.uk n engl j med 357;6  www.nejm.org  august 9, 2007 627 Book Reviews Vaccine: The Controversial Story of Medicine’s Greatest Lifesaver By Arthur Allen. 523 pp., illustrated. New York, W.W. Norton, 2007. $27.95. ISBN 978-0-393-05911-3. O ver the past several decades, most vaccine-preventable diseases in the United States and other Western nations have been reduced to rare occurrences to such a degree that physicians, nurses, health care workers, and patients are unfamiliar with them. In contrast, some of these same infections remain the major causes of illness and death in resource-poor nations. A number of books about specific infections (such as polio and smallpox) and the vaccines that prevent them have appeared in recent years, but Arthur Allen has chosen to highlight most of the vaccines that have evolved in the two centuries since Edward Jenner introduced smallpox vaccination in 1796. Allen’s themes are the research and development that led to the creation of these vaccines, the personalities of the people who were involved in this progress, and the concomitant rise of the antivaccine movement in the United States. Allen is a freelance writer who has published articles in the Washington Post, the New York Times Magazine, the New Republic, Mother Jones, Redbook, and other publications. In writing this book, his first, he has attempted to interview both those who are involved in vaccine development and policy and those who have become active and vocal in the antivaccine movement. As a journalist, he provides thoughtful insights into the personalities and activities of all who have been available to him for interviews or less formal conversations. As a result, he is able to present much information that is unknown to many of us who trumpet vaccines as exerting the greatest impact on infectious diseases — second only to clean water supplies. Allen begins with the history of Jenner and the controversies that surrounded the adoption of the smallpox vaccine during the 150 years after the publication of Jenner’s seminal paper. After further commentary on Louis Pasteur and the development of rabies vaccines in France, Al- 628 len devotes the rest of his book to events, products, and people in the United States. He concentrates most energetically on the personalities — Jonas Salk and Albert Sabin, among others. Fortunately, he was able to interview Maurice Hilleman, a power in the vaccine industry, before his death in 2005. He recounts the stories of the contamination of yellow fever vaccine with hepatitis B virus during World War II, the paralytic polio that was transmitted by Cutter’s Salk vaccine, and the swine flu vaccine that caused Guillain–BarrГ© syndrome in 1976. In the last third of the book, Allen discusses the controversies surrounding the diphtheria, pertussis, and tetanus vaccine; the measles, mumps, and rubella vaccine; and the use of thimerosal (ethyl mercury). He again describes proponents and opponents of the vaccines from a journalist’s perspective. Although some might disagree, I found his writing well balanced, and he includes more information about opponents of vaccines than one usually finds in similar sources. The audience for this book should be broader than just vaccinologists. Physicians who administer vaccines in their practices — including pediatricians, family physicians, internists, and geriatricians — will find much information that affects their patients and their interactions with those patients. Allen has cast a different light on much of the contention that has arisen in recent years, and he challenges those of us who are committed to its resolution and to the continued prevention of disease. Samuel L. Katz, M.D. Duke University Medical School Durham, NC 27710 katz0004@mc.duke.edu Dr. Katz reports receiving consulting fees from the Merck Vaccine Advisory Board. Book Reviews Copyright В© 2007 Massachusetts Medical Society. the journal’s web and e-mail addresses: For letters to the Editor: authors.nejm.org For information about the status of a submitted manuscript: authors.nejm.org To submit a meeting notice: meetingnotices@nejm.org The Journal’s Web pages: www.nejm.org n engl j med 357;6  www.nejm.org  august 9, 2007
© Copyright 2025 Paperzz