November
1995
PSYCHIATRIC
SERVICE S
A Journal
American
Association
Formerl
(;ornnlilnitv
When
Learning
Mistakes
Less
Is Less:
From
of the
the
Past
#{149}
Best
Practices:
Mental
the
Health
Primary
Keeping
Care
Care
in
Setting
of the
Psychiatric
Hospital
afld
Psychiatry
#{149}
Impact
and
a VA
Program
Homeless
Cost
for
Veterans
of
Decanoate 100
HALDOL#{174}
(HALOPERIDOL)
Offer
INJECTION
your
patients
100 mg/mL
the
most
consistent
relapse
protection
Establish a safe, effective oral haloperidol dose
How Much?
Patients
1o
who are stabilized
mg/day,
Initial month’s
who are elderly,
on oral doses
or who are debilitated2
Patients
who are maintained
>10 mg/day,
who are tolerant
or who are at risk for reIapse
dose is 10 to 15 times patient’s daily oral dose*2
on oral doses
to oral medication,
(
Initial month’s dose is 20 times patient’s daily oral dose*2
How Often?
#{149}
Once a month
. Since the first injection should not exceed 100 mg, the balance of the first month’s dosage can be administered 3 to 7 days later
How
U
High?
Maintenance
*Supplemcntatin
U
Total monthly dose should not exceed 450 mg
Maximum volume per injection site should not exceed 3 mL
U
10 to 15 times daily oral dose depending on clinical response2
with oral haloperidol
Decanoate
HALDOL
can be used during periods ofdose
50 I HALDOL
Decanoate
adjustments
100
(h.IodoI)
T lIsuIg
a
ammsiy oily. lusts
pmaIb,
compk. ,scdbEn iuIsrmaon in HALDOLs
HkD
Dscaaoa
-4
tONTRAIICAT1ONI Smce the pharmacog and cmc xo
of KkDOI Decanoate 50 and NALDOLDecanoate 1 are attflbuted to
H*iDO1 hatopefld
the xtM medcabon, CONTRAINOATIONS,WARNINGS,and addon Utormabon are those of HALOOLmodified
to reflect tt prolonQedtioit HkD o controddicated in severe toot ceatod nervotmsm
premoon or comatose states from any
causeand in#{241})divduais
whoare hypersensitiveto did drug orhave Parkmsoos disease.
WARIIPIG$:TIrdM DysEkissla: Tardivedysisnesi a syndrome consot ot potenhafly rreveodbl involuntary,dysisnodc mements may
deodop in patodts tread edth anflpsychohc dmgs. Althoughthe preodence ofthe syndmme appears to be isghest among the isdedy, aspe
dertywomen,
d o enposmb to retyupon preodence bmatas to predict attt ncepfionotanfipsychofictreatment wflfl pahents am
hedlyto developthe nymdrome.Whether anfipsychoficdnig products differin then potented to cause tard dysidnena is unknown. Bothfl
osk of deodopisg ta(dM dysisneod ami the kkethood that dwdl become irreversdi are ved
to ncrease as the dumfion oftreatment and
tt ted cumisatiea dose of anfitmychote:drofisadministered to the it
nn:rease.Hnr,
the syndmmo can dendop, aJthoih much edo
commordy, aften reedvely brief treatment penods at w doses. There o no known treatment for essafifished cases of tard dyskasesia
aIthotfl the syndrome may mmd. mty oncompletely, danfihOI
trement is withdmon. Mtipsychoeictreatment, died, howeesr, may
suppress (an rtiay sopp(ess)ttm signs and symptonm of the sysdmme and thereby may possibty mask the underlyingpross. Tfn effect
fled nymptomat soppressmn Z upon the konQ1ermcourse of fl syrismme o unedn. Gwenthese consiserahons, anhpsychotc dni
shoskt ed prescisbed is a manner fled is most Iy to nenmoze the xcurrence of rthes dysiosesa Chmn anfipsychot treatment shoukt
enery be reserved tor
edo sofferfrom acflroni itkresstfoat1)o kno to respond to anflpsychoeicdni, and 2)torntrorn atternafl equallyeffectsie, but
tess harmfultreatments am no avadaise or appropisate. In patatnts who do requne chmmc treatment the
snodtest dose and the shortest durahonof treatment producm9a sahstactory dinis responseshosidbenaught TheneedforcondonedtreatmeisthouI he reassessedafty.
Usons andsymptomsoftardsiedysknessiappearina paflenton aohpsychohcdrog disconfinuahon
shoukt he considered. Hovec, somo patients may requne treatment despde the presence of the syndrome. (Fortorther flrformahonabotdttn
descispIon cdtarderedystenesiaaod ff5deheat detechon, ptease referto ADVERSERETIONS.)
Nsc
$s
(N
A potenhaflyheat symptom com#{216}eo
somehmes referred to as Neurisepti Matoaot Syndrome
(NMS)f been reported tnassociahnn edth asflpshot( dregs. Ghnicatmandestahoes at NMSam hyperpyreis&muscat rdy, attend menstus(inctudir coseon sigtro)aat esidence ofautonom nrstty(irregular puise or isood pressum tachycardi diaphoresis,and condiec dysrh1hnoas). Adddionatsrm may urctudeatevaedtcreatho phosphisunase, mysgteisnuho(rhabdomyisysm)aod ute rend
The
diagnostc evatuationof pahents edththis symirome o conyatcated fl arrivv at a diagnosis, d o impoflantto isenhfy cases wherethe choecat
presentation includesboth seflous medat iNness(e.g,pneumonasystemi erlechon, etc.)aod untreatedor inadequatelytreated eotrapyramidat ogro and sym
(EPS). Other impodant consideratmns inthe ddlerentnddiagnosis Uododecentrat anhchohoerg toiscdy, heat stroke,
dregteesr and pismarycerflratnermo system(CNS)pathotogy. The maoement of NMSshouh inchide 1) immediatedisconhnuahon of
anhpsychoflc dregs and other drugs not essenthe to concurrent therapy, 2) ntensree symptomafic treatment and method monftoisng,and
3)treatment ofanyconcomdant seflous method proteenroforwhch specifictreatmentsareavadibk. Thereis nogeneris reemerdabout stecific pharmacologacattreatment remerm for uncnmphcated filMS.fi a patient requires anflyshot dreg treatment after recoveryfrom NMS,
the patented odntrodoctisnofdnig therystroukt hecarehiftycOns$dered.Thepaflentshouid hecarefuffymoistored, once recurrences of NMS
have been reported.ttyperpflleolaand heat stroke, rotassociated withtheabove symom compIe havealso been reported withHALDOL
heap Pmpacy(sea
PRECAUTKtNS
- Usain
Pregnancy)
camI
UN W U1um:(sea PRECAU11ONS-DrUg
Interachons)
GsNra Bronchopneumnni snmehmes tat has ho
am of anfiterychoficdregs.incsidir odognodotProm remededtherapyshonAt
he rosfitotedd dehydration, hemoconcentratmo or reducedpulmonaryntntdahonoccur,especiodyn theteddy. Decreasedserumcholesterd
andisr cutasenes and acsiar changes kent been reported eath them-rekeed
drugn, atthough not eath hatopefldoi See PRECAUTtONS
tnlormabon for Pahents for intormafionon mend andierphyncat atethesand on concoodtent usewdh othersobstences.
PRECAUTiONS:Mmsnister cauhousty to patents: 1) wrth severe cardiovascuko thsorder due to the possthuldyof transrent hypotenoon
and/or preapitahon olaogAratn)davasopressor
is required,nnephnneshosid not he used since HALOOImay blockttsvasopressorachvdyand paradoiscatfurther Hweflngof blood pressure may occur metararnino),phenylephflseor norepmephflre shouH he used); 2) recer
anficonvuisardmodcokons, edth a hotory at seizures or who EEGahnormatdies, because HALDOImay isrfl
convokevethreshoot. fluidceded,ateqUateWbCOnVOISant
theryshOUH be concomHArttynskntaaned;(3)w*h knownateogno ora historyof atterg( machorn to dregs;
)4) recerving articoagulants. since or notated instance of interferenceoccurred with the effects of one anticoagulant )phenindione).
Concomdantanhpattdnson
medafion, Hrequired,mayhaveto he confinuedafter HALDOLn disconhmed because of ddterent excrefionrates;
d both are disconhnued snouIneousiy, extrryrantttA synrorrm may occor. Intraocolarpressure may iscrease when antichotnergic drugs,
wrdodnrganflgsrtonson drugs, am odrmootered concormtanffyeath HALOOLWhen HAW is used for owes in tepoter disorders, there may
be a repel mood swmg to depression. Severe nesratoocfly may occur in pahents wok thyrotoiscoso receromganhpsychofic meduiotuir
mctudingHALDOL.
Wsi*Iu
ed PIsutr Mentis ardor physicat abdfiinsreqiared for hazardoes tasire or drerug may be impaned Aicohidshount he avoided
dueto pOSSdeeoddOiVeefteCtS
and hypotension
Drip hdsmchout Pahents receskng kthium pbs hatopendis shosid he monoored cuisidyfor eady evidence of seuhoogat toiscfiyand treatmont disconhnued prornpttyfisuch sigosappear. As edth otheranhpsychohc agents, 0 shount he noted that HALDOLmay he capabteof patesflaflogtNS depressants such asanesthefics, opotes, aodaicohid
caicio
. ipakusW ii Feff
No matageho potentid of hatopendcdwas found in the Ames Satmoneta n*rooonot achvaiion assay. Negafiveor erconsistent posdon fodugs have keen obeaned ir a, wOnid re ides studies of effects at hatopeisdcdon
chromosome structure and number The available cytogeoetic evidence is considered too inconsistent to he conctusive at this fime.
Carcisogencty stunted
orat odopefidis were conducted n Wntar rats)dosed at up to 5 mgthg dy for 24 months)and mAJtenoSatss
nice )desed up to 5 mgliQ HA ton 18 months).tr the rat study surevat was edo than openrot is ott dose groups reductug 9 number at
ratsat flsktor developingtumors. Hor,
atihotigha relaMy greater nundrer at rats sinvoed to fl tint atthe study n hh dose node aid
temate gmup these aismals did nat havea greater incidenceattomors then contris aimats. Therefore,altho4 not opfimat,this study does
suggest the ahsence at a fndopefldcdrotatedincrease ui the iscotence at neoptesia ii rats at doses up to 20 horns the usuat doty human dose
terchrononresotaotpienes.
trtemmisett5and2Oflmesffrehflestnded
dadydosehothrooicor resished patients, therewasastahshcaffysignthcant nicrease in mammary gtand neo#{216}asis
and tent tumor rocidence;at 20 tidies the same dady dose there was a stahshcoty
sniflrant increase In pdufiarygtend neoptasia In male m no stahstlcaflysigrdficantdifferencesin inddences at totat tumors or specthc
tumor pes were noted. Anhpshot dregs idevatepnntactn veis; theetevahon porsots duflng chmoiodminitraflon Issue cuflureeopeflmeeds indatn that ugproism&y one-druidat human breast cancers am prolacbn dependent is idtro,a factor at potenhat Unportanceif the
#{149}
10 to 15 times daily oral dose depending on clinical response2
. 1120 times the daily oral dose is used, monthly dose should
be reduced based on clinical response (by approximately
25% of the original dose, each month for 2 months) until
appropriate maintenance dose is reached3
until steady state has been achieved.
prescnpflon at these dregs o coirteni1ated in a pabent with a preidoustydetected breast cancer. Althoughdisturbances such as gatactorrhet
amenorrhea gynecomasb&and kepotence tens been reported,the cbrdcatsnificance at elevatedtenon prokechntends is unknownfor most
patients. do increase n mammay rwo#{216}asois
has beer found in rodente after chroisc ednuidsOratiOnat anfipoychoficdregs. NidtherctrWcat
studies nor epideeneato$ skated conducted to date,hnoer, Poseshownan associahontatweer thmoi odmoristrahOr
at these drugs and
mammaiytumoisgenesis: theavaitabItevidence iscOns)deredtOOlimied to beconctusiveatthisbnw.
Use,. to Pviguoc PregruocyCategory C.Sate use in pregnancyorinwomenOkidytohecomeprnatif has not been estabtehed; useMy if
benefitCteaify)UShfieS
potentot hazardstothe fetus.
N
Methenc tnfantsshoute not be nursed duflng drug treatment
Petetrfc Use: Controtedtrislsto estabhohthe safetyand effechvenessof intrarnuscuteradminitrahon in chddren havenot been conducted
AOVERU REACTiONS:Adverse machoes fotmwmgthe edministrahor of HALDOLDecanoate 50 or HALDOt.Decaooate 1HAare those at
HALDOLedopefldot Suice vastexpenence hasaccamufated edth HALDOLtheadveise macboos am reported forthatcoinpourid as t astor
hatopeisdo)decanoate. Made at in
medicahons, iscatbssoe machoes hans been reported who huopefldd decaooate.
csisEIci EThymm Syu#{216}oms($)- EPS doflyp theabniisstrahon at HALDOI(fatopefldot)have teen reported frequenfly,often
duisug the first few days of treatment. EPS can be categonzed generafly as Partunson-like symptoms, akethisia,or dystonis (inctioting
opisthotonosandacidogyriccrisis).Wtd aftcan occurat refafivety doses, they occar morefreguenttyandwithgreaterseesnityat tegher
doses. The synoptonromaybe coiflrofed withdose reductionsor odministrafionat anhparfdnson drugs such as berotropore mesytate USP or
thhexyphenid)1hydrochuidde USP. f shotid he noted that persistent EPShans teen reported;fla dreg may have to be disconfimuedin such
cases. WftbIrIWII Emst
Nsmio,ic& $os - Abrupt disconhnuahon of short-term anh-psyshnhc therapy is generallyunenentful.
However,some pahentson matntenance treatment eugeisencetraruterd dystenefic signs after abrupt wifhdrawat.tn certisr cases these am
indishnguishabtefreonTarthve Dysuinesia”except for durahon, ft is unknown whethergraduat Wifhdrawatad) reduce the occurrence at these
signs, but unfi)further evidence is avistebteHALDOLshouot be graduoty wfthdrawn.TardlvsDystdossia - As who at) anttpsychoficagents
ItALDOLhas beenassocatted wifhpersisttmdysidnesias. Tardise dysidnesi&asyndronu consisbog of poterthaflyirreversth1 inviduntary,dys#{149}
uinetc monements, maypear insorne pabentson king-termtheryor may occarafterdnig thery has been disconhnoed. The flskappeais
to begreater is eldedy patents on h#{231}h-dosetherapy,
especaNyfemales. Thesymptomsam persistentand insnow patients appearirreversisle
Thesyndromeis charactenzedby rhylhskcatinvotantarymovementsat tongut fain, mouthor w e.g., protrusionat tongue,puffingat
cheetu, puckenng at month, chewng moesments). Sometunes these may be accompaised trj iruntaty mmests at erifrenibes and the
trunk There o no knowneftecbve treatment for tendon dyshmesia anbpartenson agents usuafty do not aJeidate fla penifonre at that syredrome. fi n suggested that at)anbpsychot agentsbedisconhooedfithesesymptomsappear.Shouhiifbe rwcessatyto rnnstihdetreatnoen
or kicrease thedosageof the agent or switchto a differentanhpsychot agent, this syndrome may he masked. ft has been reportedthat floe
venrmcutermovementat the tongue may he an earfysign at tardsie dystunesiaand ifthe medicahon is stopped at that how the fat) syndrome
may not devetop.Titles Dysloufa - Tandsiedystona not assoaated edth the above syndrome, has aiso been reported. Tardise #{216}ystorila
is
charactenuedby detayedonset ofchoroc ordystoruc movement is often persistent, and hasthe potenhatat becoming irreversdot fiber NS
Efiscis - )nsornn resttessness, anroety, euph* agifahon, drowsiness, depression, )ethargy, headache, contusion, verfigo, grand mat
sesiurns, and enacerbatuin of poychof symptoms inchidinghafluctnahons,and catatoioc-)ikebehaidOot states wfoch may he responsive to
drug withdrawatand)ortreatmentedth anhchokneypcdrugs.
Bodyas a Wsfs: Nesr
mahgnant syndrome )NMS),hyperpyreroaand heat stroke have been reported ado HALDOL.Sea WARNINGS
forfurther intormahonconcerningNMS.)
Csidtevaacalat Bisdi Tzhycard hypotension, hypertension and EcG changes, iscludAigpridongahon of fla O-Tirftervatand EcGpattern
cfwngescornpahhte withthe pofymorphotoconfigurahon attorsades do porntes.
Nimaite#{231}k
Efl.c Reports at mALusuaty transient edhOpemaand teukocytosis,nodmat decreases ot red Hood cef counts, anernj ora
tendencytoward monocytosis;
agceoidosy1osisrarefyreported and My inassocishonwhoOthesmedahOn.
UWEIPIdE tmred fiverfUnctiOnanWorureiice.
OsiiiaI
AsasDoerMaradopapufarandacneifonn
machors,isofatedcasesofphidoserottMty,isss at hur.
EndocetueDteoodsnc Lactahon, breast engorgenient, masta
menstniat irreguhohes, gynecomas* impotence, increased libido, hypergceini hypogcernisand hyponatrern
GastrointeetloalBhctt Anorexj consbpahon, diarrhea hypersatsiahon,dyspepsa nauseaand vomifing
AiNomic Rudloos: Drymouth, blurredvision, urinaeyretenhon, diaphoresis and priapism.
Rssoiy
tecf Laryogospasin,bronchospasm and ircreaseddepth at respirahon.
s_I
Sins Cataracts,rehhyandidsuat
disturbances.
mlii,: Cases atsudder and anexpected death bans teen reported inassociatior withthe administrabonat HALDOLThe natureatttw evidence
nodies if impossible to determine deflnthvelywhat rote, if any, HALDOLplaynd in the outcome at the reported cases. The possdoldy that
HALDOLcoused death cannot at cours he erduded, bid if is to be kept vi mod that sodden and uneopected death may occur vi
when
theygo untreatedoration theyamtreated wiffiOthenanhpsychObrdrugs.
Psaait
Eneir Hyperammonema has teen reported ina 5/ year old cfnd with citrolhnemi an inherded disorder at ammonia tomehoe, tidtuedngtreabneeifidth HALDOL.
PORTAIIT: Fell dbadieiwtenaeaalmete be read before NALD or NALD Decaneats prodacteats edmtetensd anpnescotbad.
Fot*rmatfse ooppmptsssauhoaImudetevseteaap,
see tell prsscdbhig hdonoalloa.
Theshoif-achug HWDO1inform
isuiteodedoisytoracid&yagdated psychohcpahents who moderatidyseoeretovesysevereponp(orns.
1th192
1. DaviiJM, KanCJM. Marder SR.,et al. Dose response oiprophybctk antipsychotics J a: Piyb:a.
1993;54(suppl 3):24-30.
2. HALDOL2 DecanoatePackc risen. McNeil Pharmaceutical.
Spring House. PA i94”. Revised 0/13/92. 3. Ereshefsky L. Toney G,
Lyman RL Saldad S1 Anderson co, RichardSAL. Halopendoldecanoatc
an effective dising strategy. Presented at the American Psychiatric
Association
44th Annual Meermg. May 991; New Orleans, La.
Rcferc&es;
1’
McNEIL
PHARMACEUTICAL
RARITAN,
08H02978/02-i4-95
NEWJERSEVOSeOG0002
NOVA
P0001000UOICALS
I
I
-
HALDOL
/morr/i
Provides
the
protection
with
no
increased
X T E N 1) 1 N G
consistent
from
relapse...
risk
as compared
E
most
to oral
PROTECTION
of side
therapy
Fioi
HALDOL#{174}
Decanoate
(HALOPERIDOL)
V
\{
i
INJECTION
effects
R
#{128}
L A P S E
100
100 rng/mL
%
4’
She’s
anxious.
She’s
agitated.
She can’t sleep.
She’s depressed.
Paxil effectively
relieves
depression and associated
symptoms of anxiety.14
60% to 90% of depressed patients exhibit associated
symptoms of anxiety such as agitation, sleep disorders,
weight lossand gastrointestinal problems56
Incidence of agitation with Paxil iscomparable to
placebo (2.1% vs 1.9%);incidence of nervousness and
of anxiety vs placebo is 5.2% vs 26% and
5.0% vs 2.9%, respectively7
Most common adverse events include:
nausea, somnolence, asthenia, dizziness, insomnia,
sweating, ejaculatory disturbance and other
male genital disorders*7Concomitant use of Paxil
in patients taking monoamine oxidase inhibitors (MAOIs)
iscontraindicated.
�Incidence of 5%or greater and incidence for Paxil
at least twice that for placebo
Please see brief summary of prescnbing
information on adjacent page of this advertisement
ONCE-DAILY
20
MG
hC/
LIFTS DEPRESSION.
LOWERS
ASSOCIATED
ANXIETY
SYMPTOMS.
3
Sm,thKhne
Pharmaceuticals
Philadelphia,
PA 19101
Beecham
_____________________________
В© SmithKline
Beecham,
1995
Body as a Whole: headache, asthenia, abdominal pain, fever, chest pain, trauma,
back pain. Cardiovaacular:
palpitation, vasodilation, postural hypotension. Dermatologic: sweating, rash. Gastrolnteetinal:
nausea, dry mouth, constipation,
diarrhea, decreased
appetite, flatulence,
vomiting, oropharynx
disorder, dyspepsia,
increased appetite. Musculosk&.tal:
myopathy, myalgia, myasthenia.
Nervous
System:
somnolence,
dizziness, insomnia, tremor, nervousness, anxiety, paresthesia, libido decreased,
agitation, drugged feeling, myoclonus,
CNS stimulation,
confusion. Respiration:
respiratory disorder, yawn, pharyngitis. Special Senses:
blurred vision, taste perversion. Urogenital
System: ejaculatory disturbance, other
male genital disorders,
urinary frequency,
urination disorder, female genital
ONCE-DAILY
IAKL
PAROXET/NEHC/
disorders.
Studies show a clear dose dependency
for some of the more common adverse
events associated with Paxil use. There was evidence of adaptation to some adverse events with continued Paxil therapy (e.g., nausea and dizziness). Significant
weight loss may be an undesirable result of Paxil treatment for some patients but.
on average, patients in controlled trials had minimal (about 1 Ib) loss. In placebo-controlled clinical trials, Paxi/-treated patients exhibited abnormal values on liver func-
References:
1. Dunbar G,
398. 2. cohn
cohn JB, Fabre LF, et al. BriPsychiatry.
1991;159:394JB, Wilcox
J Clln Psychiatry. 1992;53(suppl): 52-56.
3. Feighner JP, Boyer WE JCIIn Psychiatry. 1992;53(suppl):44-47.
4. Fabre LE J Clln Psychiatry 1992;53(suppl):40-43.
5. Sheehan D,
Dunbar G, Fuell DL. Psychopharmaco/Bull.
1992;28:139-143.
6. clayton PJ, Grove WM, coryell W, et al. Am JPsychiatry. 1991 ;148:
1512-1517. 7. Paxil (paroxetine
HCI) Prescribing
Information.
cs.
PAXIL (brand of paroxtine
tion tests
hydrochloride)
See complete
prescribing
information
In SmithKllne
Beecham
Pharmaceutior PDR. The following
is a brief summary.
AND USAGE: Paxil is indicated for the treatment of depression.
CONTRAINDICAT1ONS: Concomitant use in patients taking monoamine oxidase
inhibitors (MAOIs) is contraindicated.
(See WARNINGS.)
WARNINGS:
Interactions
with MAOls may occur. Given the fatal intractions
reported
with concomftant
or immediately
consecutive
administration
of
MAOls and other SSRIs, do not use Paxllin
combination
with a MAOI or withIn 2 weeks of discontinuing
MAOI treatment.
Allow at least 2 weeks after stopping Paxil before starting
a MAOI.
PRECAUTiONS:
As with all antidepressants,
use Paxil cautiously in patients with a
cal. literature
INDICATiONS
history
of mania.
Use Paxil cautiously in patients with a history of seizures. Discontinue
it in any
patient who develops seizures.
The possibility of suicide attempt is inherent in depression and may persist until significant remission occurs. Close supervision of high-risk patients should accompany
initial drug therapy. Write Paxil prescriptions for the smallest quantity of tablets consistent with good patient management
in order to reduce the risk of overdose.
Reversible hyponatremia
has been reported. mainly in elderly patients, patients taking diuretics or those who were otherwise volume depleted.
Clinical experience with Paxil in patients with concomitant systemic illness is limited. Use cautiously in patients with diseases or conditions that could affect metabolism or hemodynamic
responses. Observe the usual cautions in cardiac patients. In
patients with severe renal impairment Icreatinine clearance <30 mLJmin.) or severe
hepatic impairment, a lower starting dose 110 mgI should be used.
Caution patients about operating hazardous machinery, including automobiles,
until
they are reasonably sure that Paxil therapy does not affect their ability to engage in
such activities. Tell patients 11 to continue therapy as directed; 2) to inform physicians about other medications they are taking or plan to take; 3) to avoid alcohol
while taking Paxil; 41 to notify their physicians if they become pregnant or intend to
become
pregnant
Concomitant
warfarin.
during
therapy,
or if they’re
use of Paxil with tryptophan
When
administering
Paxi/with
nursing.
is not recommended.
cimetidine,
dosage
Use cautiously
adjustment
with
of Paxi/after
the 20 mg starting dose should be guided by clinical effect. When co-administering
Paxil with phenobarbital
or phenytoin, no initial Paxil dosage adjustment is needed;
base subsequent
changes on clinical effect. Concomitant
use of Paxil with drugs
metabolized
by cytochrome
P450llD6 lantidepressants
such as nortriptyline,
amitriptyline, imipramine, desipramine and fluoxetine; phenothiazines
such as thioridazine; Type 1C antiarrhythmics
such as propafenone,
fecainide and encainide) or
with drugs that inhibit this enzyme (e.g., quinidine) may require lower doses than
usually prescribed for either Paxil or the other drug; approach concomitant
use cautiously. Administration
of Paxil with another tightly protein-bound
drug may shift
plasma concentrations,
resulting in adverse effects from either drug. Concomitant
use of Paxil and alcohol in depressed patients is not advised. Undertake concomitant use of Paxil and lithium or digoxin cautiously. If adverse effects are seen when
co-administering
Paxil with procyclidine,
reduce the procyclidine dose.
In 2-year studies, a significantly greater number of male rats in the 20 mg/kg/day
group developed
reticulum cell sarcomas vs. animals given doses of 1 or 5
mg/kg/day. There was also a significantly increased linear trend across dose groups
for the occurrence of lymphoreticular
tumors in male rats. Although there was a
dose-related
increase
in the
number
of tumors
in mice,
there
was
no drug-related
increase in the number of mice with tumors. The clinical significance
ings is unknown. There is no evidence of mutagenicity with Paxil.
Serotonergic
Impaired
compounds
reproductive
and post-implantation
are
function
losses,
known
to affect
reproductive
in rats (i.e., reduced
decreased
viability
pregnancy
of pups)
was
function
of these findin animals.
rate, increased
found
pro-
at Paxil doses
15 or more times the highest recommended
human dose.
Pregnancy
Category
B. Reproduction
studies
performed
in rats and rabbits
at
doses up to 50 and 6 times the maximum recommended
human dose have revealed
no evidence of teratogenic effects or of selective toxicity to the fetus. However,
there are no adequate and well-controlled
studies in pregnant women. Paxil should
be used in pregnancy only if the benefits outweigh the risks. The effect of Paxi! on
labor and delivery in humans is unknown. Paroxetine is secreted in human milk;
exercise caution when administering
Paxil to a nursing woman.
Safety and effectiveness
in children have not been established.
In worldwide Paxi/clinical trials, 1 7% of Paxi/-treated patients were 65 years of age.
Pharmacokinetic
studies revealed a decreased clearance in the elderly; however,
there were no overall differences
in the adverse event profile between
older and
younger patients.
ADVERSE
REACTiONS:
Incidence
in Controlled
Trials-Commonly
Obs.rv.d
Advrs
Events In Controlled
Clinical Trials: The most commonly
observed
adverse events associated with the use of Paxil(incidence
of 5% or greater and mcidence for Paxil at least twice that for placebo): asthenia 115% vs. 6%), sweating
(1 1 % vs. 2%), nausea (26% vs. 9%), decreased appetite 16% vs. 2%), somnolence
123% vs. 9%), dizziness (13% vs. 6%), insomnia (13% vs. 6%), tremor (8% vs. 2%),
nervousness
15% vs. 3%l, ejaculatory
disturbance
(13%
vs. 0%) and other male
genital
disorders
(10%
vs. 0%).
Twenty-one
percent
(881/4,126)
of Paxi! patients
no more
frequently
than
placebo-treated
patients.
Other Events observed
During the Premarketing
Evaluation
of PaxM During
premarketing
assessment,
multiple doses of Paxil were administered
to 4,126
patients, and the following adverse events were reported. Note: frequent
= events
occurring in at least 1/100 patients; infrequent
=
1/100 to 1/1000 patients; rare =
less than 1/1000 patients. Events are classified within body system categories and
enumerated
in order of decreasing frequency using the following definitions. It is
important
to emphasize that although the events occurred during Paxil treatment,
they were not necessarily caused by it.
Body as a Whole: frequent: chills, malaise; infrequent:
allergic reaction, carcinoma,
face edema, moniliasis, neck pain; rare: abscess, adrenergic syndrome, cellulitis,
neck rigidity, pelvic pain, peritonitis, ulcer. Cardiovascular
System: frequent: hypertension, syncope, tachycardia; infrequent:
bradycardia, conduction abnormalities,
electrocardiogram
abnormal, hypotension,
migraine, peripheral vascular disorder;
rare: angina pectoris, arrhythmia,
atrial fibrillation, bundle branch block, cerebral
ischemia, cerebrovascular
accident, congestive
heart failure, low cardiac output,
myocardial
infarct, myocardial
ischemia,
pallor, phlebitis, pulmonary
embolus,
supraventricular
extrasystoles,
thrombosis, varicose vein, vascular headache, yentricular extrasystoles.
Digestive
System:
infrequent:
bruxism, dysphagia, eructation,
glossitis,
increased
salivation,
liver function
tests
abnormal,
mouth
dysarthria,
dyskinesia,
dystonia,
euphoria,
fasciculations,
grand
mal convulsion,
hos-
tility, hyperalgesia,
hypokinesia, hysteria, libido increased, manic-depressive
reaction, meningitis, myelitis, neuralgia, neuropathy, nystagmus, paralysis. psychosis,
psychotic depression, reflexes increased, stupor, withdrawal syndrome. Respiratory Syst.m:
frequent: cough increased, rhinitis; infrequent: asthma, bronchitis, dyspnea, epistaxis, hyperventilation,
pneumonia,
respiratory flu, sinusitis; rare: carcinoma of lung, hiccups, lung fibrosis, sputum increased.
Skin and Appendages:
frequent: pruritus; infrequent: acne, alopecia, dry skin, ecchymosis, eczema, furunculosis, urticaria; rare: angioedema,
contact
dermatitis,
erythema
nodosum,
maculopapular rash, photosensitivity,
skin discoloration, skin melanoma. Special Senses:
infrequent:
abnormality
of accommodation,
ear pain, eye pain, mydriasis, otitis
media, taste loss, tinnitus; rare: amblyopia, cataract, conjunctivitis, comeal ulcer,
exophthalmos,
eye hemorrhage,
glaucoma, hyperacusis, otitis externa, photophobia. Urogenital
System:
infrequent: abortion,
amenorrhea,
breast pain, cystitis,
dysmenorrhea,
dysuria, menorrhagia,
nocturia, polyuria, urethritis, urinary incontinence, urinary retention, urinary urgency, vaginitis; rare: breast atrophy, breast carcinoma, breast neoplasm, female lactation, hematuria, kidney calculus, kidney function abnormal, kidney pain, mastitis, nephritis,
oliguria, prostatic
carcinoma,
vaginal
moniliasis.
Poatmarketing
Reports
Voluntary reports of adverse events that have been received since market introduction and not listed above that may have no causal relationship with Paxil include
elevated liver function tests (the most severe case was a death due to liver necrosis, and one other
case
involving
grossly
elevated
transaminases
associated
with
severe liver dysfunction), toxic epidermal necrolysis, priapism, thrombocytopenia,
syndrome of inappropriate ADH secretion, symptoms suggestive of prolactinemia
and galactorrhea,
neuroleptic
malignant
syndrome-like
events; extrapyramidal
symptoms which have included dystonia, akathisia, bradykinesia, cogwheel rigidity, hypertonia,
oculogyric
crisis (which has been associated with concomitant
use
of pimozide), tremor and trismus; and serotonin syndrome, associated in some
cases with concomitant use of serotonergic drugs and with drugs which may have
impaired
Paxil metabolism
(symptoms
have included
agitation,
confusion.
diaphoresis,
hallucinations,
hyperreflexia,
myoclonus,
shivering, tachycardia and
tremor). There have been spontaneous
reports that abrupt discontinuation
may
lead to symptoms such as dizziness, sensory disturbances,
agitation or anxiety,
nausea and sweating; these events are generally self-limiting.
DRUG ABUSE AND DEPENDENCE:
Controlled
Substance
Class: Paxil is not a
controlled substance.
Evaluate patients carefully for history of drug abuse and
observe such patients closely for signs of Paxil misuse or abuse (e.g., development
of tolerance, incrementations
of dose, drug-seeking behavior).
BRS-PX:L8
in
worldwide clinical trials discontinued treatment due to an adverse event. The most
common events (1 %l associated with discontinuation
and considered to be drug
related include: somnolence,
insomnia, agitation, tremor, anxiety, nausea, diarrhea,
dry mouth, vomiting, asthenia, abnormal elaculation, sweating. The following adverse events occurred in 6-week placebo-controlled
trials of similar design at a frequency of 1 % or more.
ulceration,
rectal hemorrhage;
rare: aphthous stomatitis, bloody diarrhea, bulimia, colitis, duodenitis, esophagitis, fecal impactions, fecal incontinence,
gastritis, gastroenteritis,
gingivitis, hematemesis,
hepatitis, ileus, jaundice, melena, peptic ulcer, salivary
gland enlargement,
stomach ulcer, stomatitis, tongue edema, tooth caries. Endocrine System:
rare: diabetes mellitus, hyperthyroidism,
hypothyroidism,
thyroiditis.
Hemic and Lymphatic
Systems:
infrequent:
anemia, leukopenia, lymphadenopathy, purpura;
rare: abnormal erythrocytes,
eosinophilia, leukocytosis, lymphedema,
abnormal lymphocytes,
lymphocytosis,
microcytic anemia, monocytosis,
normocytic anemia. Metabolic
and Nutritional:
frequent:
edema, weight gain, weight loss;
infrequent:
hyperglycemia,
peripheral edema, thirst; rare: alkaline phosphatase
increased,
bilirubinemia,
dehydration,
gout, hypercholesteremia,
hypocalcemia,
hypoglycemia. hypokalemia, hyponatremia,
SGOT increased, SGPT increased. Musculoskeletal
System: infrequent:
arthralgia, arthritis; rare: arthrosis, bursitis, myositis, osteoporosis,
tetany. Nervous System:
frequent: amnesia, CNS stimulation,
concentration impaired, depression, emotional lability, vertigo; infrequent: abnormal
thinking, akinesia, alcohol abuse, ataxia, convulsion, depersonalization,
hallucinations, hyperkinesia,
hypertonia, incoordination,
lack of emotion,
manic reaction,
paranoid reaction; rare: abnormal electroencephalogram,
abnormal gait, antisocial
reaction,
choreoathetosis,
delirium,
delusions,
diplopia,
drug dependence,
SB
Smsthkhn.
Bescham
Fma;eu
Philadelphia, PA 19101
JANSSEN
g
Business
Information
Services is a monthly
interdisciplinary journal published by the American Psychiatric
Association,
1400 K
Street, N.W., Washington,
D.C. 20005.
(The journal
was named Hop ital and Community Psychiatry untilJanuary
1995.)
Psychiatric
Editor: John A. Talbort, M.D.
Managing
Editor: Teddye Clayton
Office
Phone, 202-682-6070
Fax, 202-682-6189
Editorial
Inquiries:
Editorial
Periodicals
Joyce
Ailstock
202-682-6250
Fax, 202-682-6347
Director:
Nancy
Frey
Advertising
Production
Laura Abedi
Manager:
Advertising:
Services
Brian
Buono
Services
(see address
Directory:
above)
subscription
Washington,
D.C. 20005
Phone, 202-682-6240
Fax, 202-789-2648
Director:
Assistant
Marketing
Director:
Director:
1106
located
above
Beth
Prester
Jacqueline
Elizabeth
Young
Flynn
from previous
volin the current
volpurchase
from the
Single
copies
$7 outside
the U.S.
Reprints
Reprints
of single
articles
are available
from the APA library; phone,
202-6826080, or fax, -6248.
The charge is $10 per
article, or $5 per article for APA members
and staff in organizations
affiliated
with
the Psychiatric
Services Resource
Center.
Bulk reprints
of journal
articles
are
available
(a minimum
of 100 copies).
Al-
Electronic
and
PsycbiatricServicec
the name on
for
residents
Residents
may receive a free
to Psychiatric Services through-
residency training.
Residents
requesting
a free subscription
should send
their name and address
along with the
name and location of their residency
program, their year of training,
and the
name of their training
director
to Susan
Kuper,
APA Member
Services,
1400 K
Street,
phone,
copies (issues
earlier issues
available
for
department.
the U.S. and
low four to six weeks
out their
Circulation
Department
American
Psychiatric
Association
1400 K Street, N.W.
Back
umes or
ume) are
circulation
are $6 in
for delivery
placing
an order. For a reprint
or other information,
contact
services
at 202-682-6250.
Subscriptions
health flicilities
Subscriptions
Psychiatric
Classified
Advertising
Rita Bellinger
APA Periodicals
Services
1400 K Street, N.W.
Washington,
D.C. 20005
Phone,
202-682-6250
Fax, 202-682-6347
Circulation
in the Wash-
area).
and organizations
can receive group subscriptions
toPsychiatnc Services at discounted
rates through
APA’S Psychiatric
Services Resource
Center. For more infbrmation,
contact
Mary
Ward; phone, 202-682-6173;
fx, -6348.
202-682-6329
and
number
Group
Mental
202-682-6347
Products
(202-682-6240
D.C.,
the mailing
label. For address
changes,
include
both the old and the new address. Please give at least six weeks’
advance notice ofa change ofaddress
to ensure uninterrupted
service.
1400 K Street, NW.
Washington,
D.C. 20005
Fax,
(see be-
low), the journal
is available
only through
paid subscription.
One-year
subscriptions (12 issues) within the U.S. are $40 a
year for individuals,
$60 for institutions,
and $20 for students.
Subscriptions
outside the U.S. are $60 fbr individuals,
$80
for institutions,
and $30 for students.
(Copies are shipped
to foreign countries
by
air freight.)
Make checks payable to APA
and mail to the circulation
department
at the address
at lower left. Credit
card
orders are accepted
by phone;
call 800-
ID.
Buono
Phone,
residents
For address
changes
or inquiries
about
subscription
status
or billing,
contact
the circulation
department.
For faster
service, refer to the seven-digit
personal
Pharmaceutical
Advertising
Director:
RaymondJ.
Purkis
2444 Morris Avenue
Union,
New Jersey 07083
Phone,
908-964-3100
Nonpharmaceutical
Rates
for psychiatric
Address
Changes
and
Subscription
Inquiries
Sales
APA Periodicals
Except
ington,
Phone,
Brian
Subscription
368-5777
Services
Advertising
for Readers
N.W.,
Washington,
D.C. 20005;
202-682-6062;
fax, -6385.
Missed
Issues
and Back Copies
Please notify the circulation
department
of missed
issues
within
two months
the publication
date and allow
two
three weeks for delivery.
Psychiatric
of
to
Services
after
order form
periodicals
Microform
Formats
is available
in CD-ROM
as part of the American
Psychiatric
Electronic Library.
For more in.fbrmation, call
800-368-5777.
able
University
more
List
The
The journal
is also availand microfiche
from
in microform
Microfilms
inlbrmation,
International;
for
call 800-251-0600.
Rentals
journal’s
list can be rented
ofthe material
to be
mailed
must be approved
by APA before
the list is provided.
Call 202-682-61
58 to
request
a list rental brochure.
lbrmailings.
subscriber
A sample
Advertising
For advertising
rates and other infbrmation,
contact
one of the advertising
sales staff
members
listed in theleft-hand
column.
All ads are subject
to editorial
approval
before publication.
APA accepts
no responsibility
for claims
made by advertisers.
The acceptance
of advertising
does not in any way constitute
APA en-
dorsement
service
or approval
ofany
advertised
or product.
Permission
to Copy
or Reproduce
APA freely grants permission
to photocopy material
from the journal
in limited quantities
for educational
or classroom use. Reproduction
in any other
form or for any other purpose
must be
approved
in advance
by APA. For more information,
contact
periodicals
services.
November
1995
Vol.46
No.
11
Information
for Contributors
Psychiatric Services, formerly
named
Hatpital and Community Psychiatry, is a peerreviewed
interdisciplinary
journal
published
monthly
by the American
Psychiatric Association.
The journal provides
comprehensive
coverage
of all aspects
of psychiatric
care, treatment,
and service delivery.
It has a strong
clinical
focus but also offers in-depth
coverage
of
administrative,
legal,
economic,
and
public
policy
issues.
Submission
General
of manuscripts
requirements
Psychiatric
Services reviews
material
for
publication
on condition
that it has not
been previously
published
and is not being reviewed
for publication
elsewhere.
Submit
manuscripts
to the editor,
John A. Talbort,
M.D., Psychiatric Servicer,
1400 K Street, N.W.,
Washington,
D.C.
20005.
(Phone
inquiries,
202-6826070;
fax, 202-682-6189).
Six copies of
all material,
including
figures,
are
needed
for peer
review.
Include
telephone
and flix numbers
for the corre-
sponding
author.
For peer review,
ing case reports
all material,
and references,
includ-
must
be
double-spaced
on 8’/2-by-1
1-inch paper,
with margins
a minimum
of 11/2 inches
on all sides.
All pages should
be numbered.
Authors
will be encouraged
to
submit
the final version of the paper on
an IBM-compatible
disk.
Because
Psychiatric
Services is an interdisciplinary
journal,
authors
should
write clearly
and concretely
and use a
minimum
of jargon.
To communicate
more eftctively,
authors
should
use active voice,
first person,
and short sentences whenever
possible.
Authors
must
use gender-neutral
language.
Authors
must
careftilly
protect
patient
anonymity,
and must
disguise
identifying
infbrmation.
Copyright,
Psychiatric
financial
disclosure
Services
requires
transfr
of
copyright
to the American
Psychiatric
Association
so that the rights of authors
and the association
can be protected.
The journal
also requires
disclosure
of
financial
interests
in products
or ser-
Psychiatric
Services
November
1995
vices
described
in the paper.
A form
requirements,
which
must be signed
by all authors,
will be
sent to the corresponding
author.
describing
these
of articles
state in the covering
letter
the
type of article
submitted
and the word
count (excluding
references
and tables).
Regular
articles,
including
research
Types
Please
reports.
In general,
articles
should
not
exceed 3,000 words excluding
references
and tables, although
some exceptions
are
permitted.
For articles
not reporting
research
studies,
include
an abstract
(100
to 1 50 words)
providing
factual
information.
Research
reports
must
include
a
structured
words)
abstract
(maximum
with
250
the following
headings
and
information:
Objective, the study purpose
or research
question;
Methods,
including
study design,
setting,
the study population,
intervention(s)
if any, and main
outcome
measure(s);
Results,
the main
results
of the study; and Conclusions
directly supported
by the data.
Research
reports
should
follow these
guidelines:
1) Use the standard
format of introduction,
methods,
results,
discussion,
and conclusions.
2) In the last paragraph
of the introduction,
state the purpose
of
the research.
(If the purpose
is not stated
as a research
question,
it should
be translatable
into a research
question.)
Also
indicate
the type
of study
design.
3)
Include
data on the sex, age, and race of
the study subjects.
4) Preferably
in the
methods
section,
describe
the data analysis procedure
concisely
but in a manner
understandable
by nonstatisticians.
5) In
the results section,
including
tables,
report
only the findings
related directly
to
the research
purpose
or research
question. Omit
other data. 6) Report
numbers thr all percents.
7) When
reporting
statistically
significant
results,
always
report observed
test statistic
value,
degrees of freedom,
probability
level, and,
fbr t and F tests, whether
repeated
measures were used.
Literature
reviews
and special
articles. Generally
they are solicited
by the
Vol.46
No.
11
editor and are 4,000
to 7 ,000 words plus
no more than
100 references.
Anyone
interested
in submitting
such material
should
consult
the editor.
Reviews
should
focus on recent
literature.
Literature
reviews
must
include
a
structured
abstract(maximum
250 words)
with the following
headings
and information:
Objective, the primary purpose of
the review; Methndc, data sources searched,
how studies
were selected
or excluded,
and (if applicable)
how data were abstracted;
and Results and Conclusions, the
main findings
or conclusions
from the
review and their clinical
or other applicability.
Brief
reports.
Maximum
length
is
1 ,200 words, plus no more than ten references and one table or figure. Include
an abstract
oflOO words maximum.
When
reporting
research,
follow the guidelines
for research
reports,
above.
Reports
of unusual
cases. Such repOrts, describing
unusual
or challenging
patients
and their management,
should
not exceed
1,200
words plus ten references. They should
consist
ofa brief literature
review,
an account
of the case
and its treatment,
and a discussion.
Commentaries.
Authors
may submit commentaries
of up to 1 ,200 words
for the Open Forum section.
The editor,
at his discretion,
may invite one or more
commentaries
(for the Open Forum section or elsewhere)
on any paper accepted
for publication.
Letters. Letters (published
at the cditor’s discretion)
can be no more than 500
words plus five refrences.
Letters
related to material
published
in Psychiatric
Services will be sent to the author
for
possible
reply.
Ideas section.
This section
contains
brief
flictual
descriptions
(maximum
200 words) of programs
or activities.
Columns.
Material
for columns
is solicited
by the column
editors.
Authors
of possible
submissions
should
contact
the column
editor directly.
Book
reviews.
Books
to be considered
for review should
be sent to the
book
review
editor,
Jeffrey
L. Geller,
M.D., M.P.H.,
try, University
Department
of Massachusetts
of PsychiaMedical
1107
School,
55 Lake Avenue
North,
Worcester, Massachusetts
01655.
Book reviewers are selected
by Dr. Geller;
potential
reviewers
should
contact
him.
Arranging
the manuscript
Title page
Psychiatric
Services uses a blind
review
system;
thus on all manuscripts
except
letters
and book reviews,
put authors’
bylines
and identifications
on a title
page
that
can be removed
when
the
manuscript
is sent for review.
Please
provide
a second
title page with only
the manuscript
title.
Authors.
Only principal
researchers
or writers
should
be listed
as authors.
Persons
listed
as authors
must
have
made a substantial
contribution
to the
paper and must be able to take public
responsibility
for it. Other collaborators
can be named
in an acknowledgment.
For each author,
list a maximum
of
two academic
degrees
or certifications
and the author’s
primary
current
affiliation
(including
specific
title and department
or agency).
List a second
affiliation if desired.
If an author’s
affiliation
when doing the work described
was different
from the current
affiliation,
give
the previous
affiliation
also.
Acknowledgments.
List all financial
support,
including
drug company
support, and any financial
relationships
that
may pose a conflict
of interest.
(See the
financial
disclosure
form sent to the corresponding
author
for details.)
For
grants,
include
the grant
number
and
full name of the granting
agency.
Acknowledgment
of individuals
is limited
to those who contributed
to the intellectual or technical
content
of the paper.
Other
title-page
information.
Include
the full address
of the corresponding
author
(and phone
and fax
numbers,
for editorial-office
use only).
List the word count, excluding
refrences and tables.
lithe
paper was presented
at a meeting, give the meeting
name,
city and
state, and full meeting
dates.
Tables
andfigures
Include
tables only when
they present
relevant
numerical
data more
clearly
than
could
be done
in text;
data in
short tables
often can be incorporated
more concisely
in text. Specify
all units
of measure
clearly.
Tables
will be edited to conform
to journal
style,
and
authors
will be asked to delete extraneous tables.
Figures
are published
only when they
contain
essential
information
that cannot be adequately
presented
in text or
tables.
Many
figures,
especially
flow
charts, are judged
nonessential.
Figures
1108
accepted
for publication
must be of professional
appearance;
ifcomputer
generated, they must come from a high-resolution
laser
printer.
Figures
must
be
clearly
readable
when reduced
to one- or
two-column
width.
PsychiatricServices
discourages
the use
ofpreviously
published
tables or figures.
Authors
who use such material
must
obtain written
permission
for reprinting
from the copyright
owner and include
it
with their submission.
Checklists
and forms
generally
are
not published.
A note that such material
is available
from the author
may be included
in the paper. However,
to flicilitate reviewing
and editing,
please
indude five copies ofany
pertinent
checklist or questionnaire,
marked “background
only,”
with the submission.
References
Limit
references
to relevant
published
material
cited in text, including
all but
widely known
tests and scales. Complete
literature
reviews
are rarely necessary.
Only
material
that has been
published,
accepted
for publication,
or presented
at a major national
meeting
can
be included
in the reference
list. Citations of material
in press must include
journal
or publisher
name.
(If unpublished material
is cited,
note the source
and year in parentheses
in the text of the
paper.
Citation
of such material
should
be kept to a minimum.)
Double-space
all refrrences.
Arrange
and number
them in order of appearance
in text, not alphabetically.
In the refrence
list, name all authors
and editors
through
the third; if there
are more than three, list the first three,
followed
by et al. Spell
out journal
names; do not underline
or use italic or
boldface.
Follow
PsycbiatricServices
reference punctuation
style.
Journal
articles.
Include
authors,
title, journal
(not abbreviated
or underlined),
volume
number,
first and last
pages,
and year. Example:
Golier
JA,
Marzuk PM, Leon AC, et a!: Low serum
cholesterol
level and attempted
suicide.
American
journal
of Psychiatry
152:419424,
1995
Books
or monographs.
Include
authors or editors,
title (not underlined),
volume
or edition,
(for federal
government publications,
any series designation), city, publisher,
year, and, if pertinent,
page numbers
of the material
cited.
Example:
Kaplan
HI, Sadock
BJ
(eds):
Comprehensive
Textbook
of
Group
Psychotherapy,
3rd ed. Baltimore,
Williams
& Wilkins,
1993
Chapters
in books.
Include
chapter
authors,
chapter
title, book title (not underlined),
volume
or edition,
book edi-
Psychiatric
Services
tors,
city,
Clark
publisher,
HW,
Kanas
and year.
N, Smith
Example:
DE, et a!:
Substance-related
disorders:
alcohol
and
drugs,
in Review
ofGeneral
Psychiatry,
4th ed. Edited
by Goldman
HH. Norwalk, Conn, Appleton
& Lange,
1995
Legal proceedings.
Follow
The Bluebook: A Uniform System ofCitation,
published
by the Harvard
Law Review
Association.
Review
process
Manuscripts
submitted
for publication
(including
invited
papers)
are sent for
blind review
to at least three independent reviewers.
Separate
statistical
review is often obtained.
The final dccision is the editor’s.
Authors
are usually
notified
of a decision
within
three
months,
although
delays are sometimes
unavoidable.
Revised
manuscripts.
Authors
are
usually
asked if they wish to make suggested
revisions
in a paper and resubmit
it. Ifsubstantia!
revisions
are requested,
the paper will be sent again for outside
review.
Every effort will be made to cxpedite
such
review
and
inform
the
author promptly
ofthe
editor’s
decision.
Revised
manuscripts
must conform
to
the general
requirements
listed
above,
including
minimum
1 1/2-inch margins,
flail double-spacing,
and a word count.
Processing
of manuscripts
Manuscripts
(including
revised
manuscripts)
are accepted
with
the understanding
that they are subject
to editing for clarity,
elimination
of redundancy,
and conformity
with Psychiatric
Services style. Generally
manuscripts
are
edited
within
three
or four months
from the date of acceptance.
The corresponding
author
receives
a
printout
of the edited
paper before it is
typeset.
He or she will be asked to check
the printout
carefully
to make sure the
editing
did not introduce
any inaccuracies and to make any necessary
changes,
answer
editorial
queries,
and contact
the
editorial
office
by a specified
date.
Authors
do not receive
galley
proofs.
All authors
receive
complimentary
copies of the issue as well as a price list
for ordering
reprints.
Indexes
Psychiatric
Services is covered
in index
Medicus,
MEDLINE,
Psychological
Abstracts, PsydNFO,
Social Science Citation
Index, Cumulative
Index to Nursing
and
Allied
Health
Literature,
Current
Contents, Excerpta Medica,
Hospital Literature
index, and other indexes
and databases.
The journal
in December.
November
publishes
1995
an annual
Vol.46
index
No.
11
Because lives
complicated by
psychosis
further
complicated by EPS.
are
�15
C
E
8
15
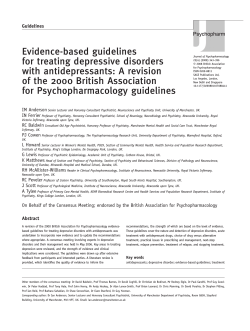
31%
20%
13%
16%
13%
2
6
10
nsperidone
placebo
16
(mqJday)
Spontaneous complaints of EPSin North Amencan clinical tnal (n=51 3).
*Mtipsychotjc
efficacy was demonstrated in a dose
range of 4 to 16 mg/day in clinical tnals, supporting
the effectiveness of RISPERDAL Doses above 6mg/day
were not shown to be more efficacious than lower
Risperdah.fr
R ISPE1 I[)(I)NJ E
#{149}
symptoms
and
demonstrated
and
adverse
an not
increase
effects.
inevaluated
extrapyramidal
safety of
doses
16 other
mg/day
has
been The
in
dinical above
trials.
Please see the brief summary of Prescribing
Information adjacent to this ad.
В©Janssen Pharmaceutica Inc. 1995
__________
h2.3-4mg
tablets
a
JPI-RS-123C
A first
choice
in
psychosis.
In vitro studies indIcate that rridone
Ia a relatively weak Inhibitor ci
cyhoctircnia PlD,
arid la not sapsc$sd hr situhulaly
Wild Vu dsswice ci
th=*.Houses,
dsicito
A
choice in psychosis.
first
__
RISPERD*L#{149}
(T
8.1cr. prucdbing,
consul coMp*
pt.wIbng
kouIon
of
iWcli lelolloulna
a bdofsumwy.
#{149}IDICAT1OI6
AN#{246}IAG RISPEROAL’
dcisd
for
meilgemed
the maofseIoo&
I*.oIdelL
OIITRAiNDICATIONS:
RISPERDAL#{176}contmiidca$sd
m patients with a
Scm.
(NMS) I
mikaco
moiIoie
bee
repodud m a,oan
______
edi*
th#{231}th.dIat*Ib.caayanudMt
iicseainenoas
NMShSbNn
Mi
I a
T!e&loL
mpoflst
A ayn*om. of Iy
sbs,
iofey
dvdnsc
movsmeis may
cv.k;
m hiadah
esyhaaugi
*Mmu#{216}ith.
pievienca ci
the sdroma
appears to be Ngh.st among the aldsdy, sepeciaMy alderly
manei 1 s cssb
isly icn pFSValInOSISnISSPIeb.
alIve limp
-
f
wd $yVI#{231}IOmSOIIanM dysidnesis pserm
a pei1cn
R1SPERDAI.,
iMig deconinuion
alocid be conideret
I4omar, acne pilents may reqwre
ItsWieci ciii RISPERDAL’W*ptsssnc.
cite ayr#{243}cme.
Potential for Proarrliythmlc
Efbcts:
Riaperidon.
and/or 9.hydroxy.
IdoM
3pS$
nhen
the 01 mval
i erme ps*
alioi4i them
no emi
Weiss i Pealed psi*
i
al 12.16 m9y,
eel thovethe
meommei#{224}d
dest Omerdei
Vial pcdon the 01 smal have been aaoc
aled Mth the xcwmnm ci mder
de pcia.
a lethisdanlig
wh1hmir
Bm
de
iithalsm, eoncom
ma cith other des th p
big 01, er ie .enm
ci cang.nl
pmloncn
m 01 i licreem the h
brccoirmiimci1#{224}wIiin
ooma&
H$1othMIoa. RISPERDAL#{149}
may Widece mtho
hpcIeneicn
ai deziess, ticerda.
aid Ii ermaith,
seccp.
eayedaly
m i*al doss1on
psdo prcb
mlsofng
aha.eenevc
wdaoiiic
piccei
The ,Ii ci oithoi*
mnuian
sal aempe may be
mininbed by hnIng the ii#{225}al
doss b I m BID m cocci Ub
aid 0.5 n
BID rn the ekIand
pe,dawIth
renal er1iepc
i#{231}imeci(See DOSAGE
NC ADMNSTAATIQI4 A dose isdecion aliccid be ccnldamd I hpcIsnsion
xcits
RISPERDAL aliocid be used ciii p.bcciw caalcn ii pes
eli
known caniovascube claeaae (hialoly ci iayocelal ofeofon
behenim, best
ta o condectlcn denormalls), cembrovaeciiar 1aeaa and
elch woiAdpreilupase perU
hypcthnsian (dehp&alici hypovclsnj
sal
odiad
-
::
pJSpEpnAIe
I4wlimath:
be used csdeuuly
A. eli
w
#{149}m
nta
&up thal elagonbe
eli
dopsalne
a tisloiy ci
D ramp
Tissis cithum .ay.dmsib
#{225}idic1st appraidmisly
taiNt imii
we prciac
depended
Ii *0, a tader ci palm
pmertliui
ci the. &m#{231}a
Iconimaybeed
Ii ap*rdalth
prealo
detected breast cancerS A. is common with conipounde eltich
we.NlmN SI lmcM ki plmy
munny
mi
sal
mpcmde: blal cal hWeipl
s&maschivedic
the layeddan.
camnc.nicIy
*idln. ccnaldsd ii rain. sal el (S.. CARc1NOGBIES1S)
H,
neither aliddd alialan ner ayidsddolo
audi. ccndaclsd
hem ahesi an esodalmi
between ciwamic skmddddon
ci ida s
ci &u
aid kimoisnMs
bi bems* the avle
evidence lmcanmidsied o lmsdb
Iid
athiiinl*on.
ci hiana
Ir#{231}cibeim
I Ira
Iw
Scemolsam
a caimmnaaly
repail.d and dose4eled
steams meal ansoceded ciii RISPEADAI? tree.
meat Since RISPERDAL’ has the potential to bTia udgmeal thinldn or
molar ddI
chci#{225}d
be cethaned tctd cperelig hasadaus ndinsy,
maddemmsancethiIVSPERDk
thempy
dean nc*althsm
advsm4
Raren.eescl
sm
have been repcdst
A aln#{216}
cane ci TIP wan rupoitsd m a 28.aar-old female pedeid remiving
RISPERDk?Tt*mlicnal#{231}lRISPEIAL
thSIVlmIAmn.IL
Fdone
Pes WI ualuanc
alhal ii sdmala II sisal may also coot ki
tunsi
add may ma ciessal
$VIIeSOmIcimaalOU9eII1CeI
dnigaor
tdcoMlaisiuth
an bae#{227}iicbliucci
ASy.ay1deCm..
salbainbemor.
caiaii I adaled stem aISOtlmQPSIda
edia el beeayo.sd
blsmpsr
ThelItyci
a anIddeSIric
ichemid
ii sthizcphrerda,
and di#{231}t
mod pdde,* mmngamesd bIOIdSrk radeantha IIkcimaIdOSS.
Clrdcal impedance eli RISPEHDAI.’II pedemis eli ceitin comicoudlati aye.
hula lassase
la lmnlst Csdan la shwisula m pulsals eli alssanss orco,
ilians hal aside allsal malohsm ci bsmodnmdc maycrest Osmaise cite
AskaciOsthOalic
hepalmnian sidOl ptolonpio,
cualon shoald becbesrvsd
bicsrdlacpisrds(Sse
WARNINGSwd PRECAUTiONS).
hr pulerds eli severe renal Impskmsid (cmulr*e dssrsrce 40 mLM*1.73
m’), oreli sevsrs hspudc hnpsimiss a baeeraludagdosealioiidbe
uset
Ptisr*s shoidd be sMssd ci the rho ci
lmof
anperialy altO
krgthe pedodci hilti dose lisbon.
Ptisnts shoide be car*icnsd shcib cperting hszudous manhijery, hrchialng
adamcbllss, raIl they we ressonshlp csrhor Vial RISP8hDAL’ thsrmpy doss
sal allul them edveissly. Tel psbssli hr rely thE physician I they become
prsrsl
or *rhsnd to become prersd
dudng Viermp not hr brsant hid err
hr hdonnthshpbysidue
Itheywetidni
crpluihrtim
urypmscr’
terorosmV*cowbsralu
toIvOidaloOhaL
No sdkhoorIlorylmem
isoommsndst
The mbsrecbcns ci AISPERDAL sal Ohist alugs have not beer syshamelcaly
rist
Cusion ahosid be used stan lien to conbilasboir eli Ohisrcss**
aIngalugssid1xh
msPL5nuysten.VuhmpotamPeelsEcialwVisaysLliagsliell
thlapotenbiwehl
maysbugoOizsthedlsc1acilmvodopaeraldopui*seugosi
Chronic aalnlnlshratlon of caibsnszeplne.
or chozsyrine eli rlspsrldone may
usiweetudsersicaci
dupsddont
Fhispsddons m mshoclzsd bycylocteoms P1.IID.. as enzyme Vicar be With.
bad by a variety ci psdrotrcp
and othsiiugL
Analysis ci alnici stulss
hrvclehrg a modsi minter ci poor metaholosis (n-70) doss not eruosi Vi
poor anasxhsnslvs melicllzarsirsie
dismal riesci idoerse .IsotsJlo
comrn
psnson ci elfecttvsnesa to the two ougs
has been made. In vitro studIes
ironed that tugs mstircbzed by olrsr P Ieozymss am only usE Wtbors
ciriepeddorsemstahcbsnt
caichiotisnioly *dan sers conaldad rn Sedan sthro mice aid Wisher rats
Ibspsdcbne
asbnlniiaisd hr the dii
doses ci 0* 2.5, aid 10 is#{231}ior
18mortahrnteandbmostabsshs
Thssedossaaeequlriasbhra4,
94 sal 375 haN Vu mudmimis biases dose (16 mday) on a mIsg Iie or
0.2, tl5and3thnssthensetnum
lssnmdaan(nice)ora4,
15, aId6VuSS
Vu midosim lamer dose (rie) on a ss’
beuis. There usia ieliciy
.
sliced rncrsssss hr plitibey #{216}snd
shsnoms
endocritie percuss adenoman
Sal mwsnsiy cisal arlsnocssinomst
Thus neoplemu we conidsmd hr be
scthr.rnsrb#{243}t The relevance tar homes risk ci Vu hirings ci prohobn.
rn.dshedendocdnebinors
hr rodsibs laradmona
Noevidenoeci msiugsnic pcissli Iardupsddonausstount
Fhsdone
(Oil ho 5 mcilmj wan irmar to licE msbn t*a not Isslily, hr
Wisher rim hr Ivan rdve
skdss at doses Oi hr 3 trims Vu masters
recommended human dose on a mm#{176}
basis The sIsal appeared hr be hr
fsmis& hr a aitcirroibo abide hr Issala dog mpsnn mobilly sat conceiVilon
usia dscrssasd at douse 04 to 10 those the turner dose on a mgho besis
Doae4sIisd decrsssss we also soled hr aerum hastosharcne et the sane
dcses. Serum tealosherone aid spans psranetera
partially recovered but
mmsted dacrsansd star itsahosal
clsccolnuet No nodsal doses were
notedhrelwust
ordo
=Jscsisssy The harshogsnic
ci doiu
studIed Es
ardthlisr
me sal hr flaw Zalend riel
Thu Esddsnca ci
mikiminalons
not hscreaned ccnwsd
hr carded rn disyshig ci rala or tu
his vsn t4hr6*nsste
humeri dosson a mn#{176}
tea. hr three rsprochicbvs
ahides to rst Vurs
an Escisane hr pr. delis cEJIErgVuVi 4 days ci
sian at doses 0.1 hr 3 hose Vu Issuer dose on a mn0 basis I la not knoms
wtisthsr these deal. were situ hr a dEed alsal as the Ishiass or pu or hr
elsots onteiess
Themwan no riodsi
dOssIOrhIcreaned ratpmp mosely.
hr one Segsrs,d I shady, Vureussas
hrciswe hr silicon ratps#{231}satadass 15
hose i#{216}ssrthsr
Vu tuners doseon amn#{176}bis.
Piecenti trasslar ci dnpsddane ascurs rn rat act Them we no sdsgsie sal
wslkcsbrclsd sitidan hr prsgserb wcmst However, tern wan one Impost a
ci agurast ci Vu corps. caisson hr err Wait mpcsed hr dspsddons hr
Iisr Tiucuisal rsliionslhr
RISPERDAL’Vurapyie wmmmat
RISPEIAL’&sosidbeuaedrEidngprugnsncycnlyVupclssblibensVijusb.
basVu
risittoVutius
Itudsalon
Wioraiddslivssyhrtunssa
la radmows
N ie not incus wtisthsr ci not dspsddene I eacrelad hr humor m& hr animi
atudea, rispeddons add 9.hy&oxydspddone
usia excreted hr breast soils.
ThsreIo werner .csling FISPERDAL Ohcsid notbmsihest
Saalelssstssus
hrdrltsn hsiunotbSsnssEliisd.
Ohrici dsdlan Id not hrdsde aIlcisid mistime ci plumbs aped 65 ash mar
hrdsIsnin.stsVwtheymsdismsshyimmyswsger
hr gsnsr
a lower atarthrg doss Is recommended for an elderly patient. reflecting a
decreased mscoidnst:
clawaice hr Vu elderly,
usi
a grsisr he.
gssncy ci dsc,sansd
renal, or ceidec itmalos aid a gusher hndsncy
hriul
tion(Sse
cLINICAL PHACLOGY
aid DOSM3E AND
ss*t*dusreseanEssntrscsiisghiopsdni(3f126).
Ottur Ev.ats
Observed
Dunlag this Pre.Msrhathisg
Evalestlos
of
PERDAL#{149}
During Is prsmatk.bng asaeasmnsnt msitsls doses of RISPERDAL were
adaisilsiad
hr 07 pissla hr phase 2 aid 3 skalan sal Vu blowing man.
hose ware reported: (Note �tmquss( we those occurring hr at least 11100
_s*
kiss(
we Isima ociunhrg hr 11100 hr 111000 pdssba
a.
1mm occurrIng hr I
thus 111000 pssdi
it la hs#{231}cstsd
hr sssshulaa that,
asaurVusmsderspodedisisdtinrQbsahssibeli
FISPDAL’Vuy
wese not nSCSssUIycSISsdbyL
PlyiIl#{224}kiew
Fmpenthsonusd
doses_,
dulnlshed seoul dei,
nsmausnsss
Mfreys*t i.d
ds
,cieont
msalo e#{231}hoda
hrowsidtid
asmesa Rs
emoloni silty, nholnersa
dste*
datuwi
syndecmp,
cMfrwIasdMwsese
Sysis. es*re
Frequent
increased sleep tmian.
omt
dysertep, walgp, *
coEi
oc
p,
th
tcme,
isulp,
Wiu psmlysj
Iegciumpatonllaoli
asma
ndgtinp, hugsndudp,dremoddais
Oasfro4vfsstlnal
Disorders:
Frequent anorexia, reduced salivation.
d
hoaned
shomelp, misnp,
gia. hemorrhOids, tis.
Rsre focal incontinence, eructatlon, gastroe.
Vip,
tongue sdsma, Ilverliculitia. nvltIs,
discolored faces. GI hemorrhage,
hsma.tsmesis.
lady as a Whote.ussI
Dbaordsrar Frequent fatigue.
Infrequent adams, rigors, malls.,
hrfluenza.hIke symptoms. Rare: pallor,
-
-
Disiis
t
homanid p9nwmsbon,
photouerisity
Emesssd ses*
amp, dscisssd
da
iopsdp, sdaieia
po
kp,ihredolsbolL
Ibaerbdmaoaiisiosrsbaa
tunmoidosip, vsrrucp, dansaths bobeno
hypelhonis,
gerdli
urticads wolousscubor
Dbao,iear
Infrequent psigliatien, hsflsnslon,
hyPotSn5IOn,AVbIOcE,IIIyOc.diEOSt
erVSI*IOiVWihyCsdII,ar.
ire pectods, premature Eli coitactions,
I wave inversions, ventrIcular
szkss
STdsoa
nymcur1
bVwMbmpatsknOr.
mieccommomiop,nis
opjsyepitrsphadbaphohap
sip, isbupholsj
ahnamsb hotnalos
hb*
aid ffitsi
is,w
Wi
hy
t
homane, cuhore phcuphddnans homa.,
thkstdahetanmdtus
R.ocdacmesidssnmnimacachmdp,
-.
Wi_
hrcodasnci,
hsmiudp, dysuds Ilast
retention, cysth
masi insufficiency. ibaacubakdasi
Syslie
DViieoc
*t
mysi#{216}s
&st adamip, sninia
teasilp,
skeletal pain. fleproahsctls’. orisrs,
Fssseho Frequent msnordsaa’,
-
tsp, Vials bmsi
pip, hlsissniwi
eriearhrowaned,
chOie
bea
Phi
Rare: bemge,
,_
Msoclierlwlii
0ISCW1IsMsbOSofTNsIl
9%psrcssdl2m4l2eol)
ciRISPBIDAL Waled psbssdehr#{216}rme
2 studIes
treatment tie to as adieme sisal, cosugered eli
about 7% on o
aid 10% on ecbvs control tuqs. The more common
event ( 0%)sescclisdelr
daccilirualon asdcoswsdsrsdbbepossitlycr
tued
et
sdempsOidd
ayn#{231}ham
dsstss
*
alsomnohnciaalmmut
iddadssrodiadiVdacooimaIonEs
12%ciRlSPE.’.Wisd
sni
colr*wsd hr 0.6% cibo
psbssba bs. #{216}vsn
Vu sknoi 404o1d
ciuiermpcstse
Visa hr FiSPBIAL0asnisuwd
hr plsosbo
I la isaluly
#{234}tisolOidaIlusdieaFilSP.’seliadhossiemad(SsePRECAUTIONS).
EICIdIuCSIeCaelsISdTdiI
usesvWwe
E
bo Chutd
7EVi hr tan 6.
hrBwsEsboixmbmisdhlis,
mpcstersousIy.mposls
Wiesaalemsrgss*
adverse events wIth an incidsnce ci 5% or greater Es at seat one ci the
mSPERDAL#{149}
oi*
and at Iesi nice that ci plscubo eeoc stisty, sonme.
==
dssinmL as
mmse
-
-
nip, titunhea
Iessdnp, i
mulila mamnt
Vials pemial
hamoithsgs UInderySys
iims.sdSGFT.
stbeila
dideldaip,
be
ste.
IM1daoctspImia
prapust
pidirila VirombugNEila
thmotoc1opeds
d
simi
sri VesS
.orE
Rast bonbap, hypsmmudp, decresssd
sh*oc
ht
hymchromla wends
Rast non.xc
wends mahwli,
ariea
I
Fieqsatemalh
ddion.
Infrequent ejaculation failure WIsIba Call arid AssIstance
ar
Rust Iesiusyhaip,
hisythadensyday,
twmope
P&gHmi
-.
daw
Asus gurecomu
mis hosi
w*bemimsdaontr.
. hrddsncsbessdon
eldlnd reports
tethsosiMvemamant
reportadiecemadsinto.
rhiction eNds we hampordy (bib not nscessariy
caussly) mIsled hr
RISPERDAL.#{149}
______
therapy, Include to. following: anaphytactic
reaction,
an_
athi Vio
ouretwowascular dIanea
dIsbehas mdaa
aggravated.
hypothermia.
intestinal ObstructiOn,
jaundice,
mania,
PsIldnsons
dssmm aggsaelsd,
psimonery embolIsm, suddsn dads.
w
Cuntr
Pelsiba
-
Si*stiici
ches RISPERDAL’ Is not a controlled sststance.
sirosid be evalulad carefully or a hIstory ci demahsup, sal such
shard be ctsssved dossly ho shins ci Rlth’ERDA[’ ndauan or skies
Bdledadraransvent
hr one cithssstwotdisprsssrbiat
Iesi 5%WdtsIOe
Vu rie ci be
wsus Wscrsansd teen ushelly, Esciesed daraloss ci step,
accunmiodalon dsh
malicad sinio,
stabs
abmcsp,
d
tep,
gip, me
dntduhsd sawn deE smdie d#{216}malos
lMmirmSPEA.’(sIepsddane)isoide
be ahadidnlsisdon a BID
sdrsrkia, g5IW*bSI5*IgelI
I srgillDhdldy,elshars.sshrhicrsmsrbs
ci 1 sap BID on Vu ucosal sal brEd day.
halsrIla hr atigat dose ci 3 leg
BID by the third day. In some patients, slower tItration may be medIcally
lie toSsing edossie swede occwnid at as Eimdsnce ci 1% or mo sat usia
appiopilie. FulVi*shsisIde
Ihdcisd,
alsoridgsnsralyocawat
Ebeivals ci not less than I week, since shady ies for the solve mslisoila
at Issi a id
among RISPEL4eisd
psbssba Waled at douse ci
would not be achiaved for approxinisly
I week hr Vu typical pallet When
10 mthan
smongplscsbotreshadpalssbshrtepocladmsstscitao6.hr
6.weE coalmiad st
OVideroc WiomOip, aliim
sudety,
*sEnsnts
are nsossessy, mmd dose hrcmmsrbsfdacmmsstis ci I rug
BIDwe recosomsodat
mst
limman S
Aa*ssycholcdicscywednmonskstadhradoee
rasaci4to
l6mqitieyhrVu
beadsip, dsn.st
EuViM
Smm
asnuloi
mmssp, pop
r*dccilrlis
ss#{231}sg dsalvsnsss
ci RISPERDAL however, mssdmci ilIad
sip,vemliahdonini
SalvaEscmansctoOVisEs
RasplasherySysbaus
dinil cou#{216}risoila,
phsubs
dyspnss. BodyaWlsoler
beds pE
sea generally seen Esa range ci 4to 6 mgfday. Doses shove 6 mgtey were not
hr be mars elilcecious than lower doses were aaaccislsd eli
chsipsk1sver.
iasbOi*t
ma tysld
ssbonhss. tisolsuer
i#{231}pst dsmonetrisd
respiratory.
Viasal: abnormal vision. U.scslo.Sk.twtal:
arthralgla.
mars utadi
______
onre
sat olwshimma
eisds aid we nb gsnsrdy
moonsoendat The sthty ci dosan ahues 16 mchbay ten not been ev#{224}isdEs
cwdIsv.cal
I hrcludas tremor, nls,
hnesip,
hypertonla, hypsddn.sia,
oculo.
darici his Dosage its scsiPspidaisnm
The mccmmindsd eli doss ie
gyric crisis. ataxia. abnormal gait. involuntary muscle contractions,
0.5 me 01Dm paleieilmemeldsdycidsbihia
pilasdselsesvsse
mnalor
tupdssr
andpsbsalaslherpmdspossdhrlegalsnuhocibstom
hyporsileala, and extispyramidi
diaordsrs. Although the Incidence ci
tapalsireirer wosti pose a rIe Dosage Escresan hrtess pelside irasid be Es
�extrepyrernidi symplairu does not sppsw hr dINer or Vu � 10 mcidW
Ercrssnsrdecinomorsthuro.5mgBm.
hrCmSSShrdOSsgNahOVS
lSmgBID
croon aid phoebe, Vu data tar hrdlviskii dose ciosme Es lied doss bids
alioidd ly
ocowi Ebsivis ci al Iesi I wss hr some paula
stew
;7t
a dos&rssponse
islalonihis (See DOSE DEPENDENCY OF
*danmsybemsdciyapprcpstis
Bdedycrdabliiad
aidadssde
sir renal hr#{231}ims*may 1mm Wa
Dos.oepsiAdmmsEvuuliDalaimmVibeddoseIis
provided
abilty to siminste RISPERDAL’thsn
normal stilts. PatIents with svldsnce ci dosersIischreas
for extrepyramidi
syn#{231}tonrs
associated wIlts
hs
function may have Increases hr the free fraction ci the’
dona
Wsknsst Asrse sisal die dialled by a chsduat for Ida dads
po
msulbng Es an enWacedillsd(SseaJNICAL
PHARMACOLOGY).
1mm alsge*idycoss#{231}stngshssaddosssci
RISP8bAL’(1,
p, 12, aid 16
Psbsdadaapradsposlanhrhysdnnshomsolansortwwhomaudlmsalons
_1
reveisda
Vi
burst torte Iolruhrg adverse mmli isepiessa
hrcmanedrhirsbon dslesp, aocosrsnodsbon disibuross
csthoida dozkresa
would pose a cciw
rIsk Sundae need hr be bashed cudously arid caddy
mud
(See PRECAUTiONSsp*mastMapWidsThem
we no svslsmdcdv
oalsclsd die hr spscllcly adrksss milchhrg from slier
arlrcbcsto
RISPERDAL#{149},
orconcsiningasncom*uisdsbillonelr
Ss
usest
RISPERDAL Es ansocishad eli osthoetatic tymclsnslon
other antipsychotica.
While Immediate discontinuation
of the previous
asihotucuds
(SsePRECAUTiONS
anbps
treatment may be amepisbie for some patients, more gratial
as:1huprcpcalonscilbSPERDM.’ardsbo.Imiad
dIscontinuation may be most approprIate for other patients In all caasp, the
ms*gawedgisodlntnci7%cibodyni#{216}dwemcosspwedhrapoOici
ci ovsdng
amisycholc acksiemsbadoir should be mhslmtret When
6. hr&.SSkVi5bO.OOI*sOI5dtdiS
mesisigailsbcdyiw*sdygseisr
WiemaciwebREDAL(16%)con#{231}ssdhrphosbo(9%
LaIsmiy
:
A biesen vssy cossyuiscrr or 6. hr ussk
coslmleia*jSmsdcdonshosidbemadIiadPsdad*.
coi*clsd this revealed ire sbciy
iilcub
IiSPEWslsosbo
sr
incus hr Vu prcpoaloswcipdaiempsisnsthigpclsslslyir#{231}asterddsangsshr
Anguat iisnter
1994
roses semis dry,
tumialogy, or udniysls psiuniers
Slmlerty, them
were no R$SPEALlecsbo
darenoss
hi Vu hrcldanoe ci dIscoslnusbons
for cMngein
serum chemistry, hematology,
or urinalysis. However,
.-==..
RISPERDAL atnhrlstrsbon wan .soclisd eli hromanan hr susan prols
-
-
-
-
JANSN
T1TUSV5LLE.
r
electrocardio9rams
of 8 out of 380 patients taking
RISPERDAL’ whose baseline QTc mtsrval wan lana than 450 mass were
observed ho have QTc hrhssvals st
Vies 450 mesa tabsg Irslinssd (ass
WARNINGS). Qiangus ci this type we not mann ernong shout 120 phoebe
jpsnc
May1995
NJ 08560
Printed si USA
Because a whole
person is waiting
to emerge.
Although the exact mechanism of action is unknown:
#{149}
Improvement
of negative symptoms and lessened risk of EPS
are thought to result from blockade of serotonin 5HT2 receptors,
possibly through a
modulatory effect
on dopamine D2
activity in the
frontal cortex
and the basal
ganglia
#{149}lmprovementof
-
symptoms
is thought to result
from blockade of
dopamine D2 receptors
in the limbic systent*
r
*Ereshefky
L Lacombe S. Pharmacological
Can iPsychiatry.
SPERI DONE
adjacent to this ad.
В©Janssen
Pharmaceutica Inc. 1995
JANSSEN
Serotoninergic
profile of
1993;38(Suppl 3):S80-S88.
Please see the brief summary of Prescribing Information
rispendone.
iic
JPI-RS-123D
cTiSmsthKhn.
B..ch.m
A first choice in psychosis.
system
Calendar
a free
Psychiatric
For
listing
ofyour
meeting
in
Services’
monthly
calenus a note giving
the details
dar, drop
of the meeting-sponsor(s),
inclusive
dates,
location,
type ofmeeting
(workshop,
conference,
annual
meeting),
theme
or topicarea
(ifapplicable),
and
the name, address,
and telephone
numher of the person
to contact
for more
information.
only meetings
Because
oflimited
consideredofmost
space,
inter-
est to the readership
will be listed.
All notices
and changes
must
be received
no later than two months
before
date ofpublication
(for example,June
1 for August
publication).
Correspondence should
be addressed
to Calendar,
Psychiatric
Services,
American
PsychiatricAssociation,
1400 K Street,
N.W.,
Washington,
D.C. 20005.
November
November
seminar
29-December
1, national
on creating
employment
opportunities
for persons
with serious
psychiatric
disorders,
sponsored
by
Matrix
Reasearch
Institute,
Radisson
Plaza Hotel,
Orlando,
Florida. Contact
Barbara
Granger,
MRI, 6008 Wayne
Avenue,
Philadelphia,
19144;
215-438-8200,
1506,
flux 215-438-8337.
Pennsylvania
TDD
215-438-
November
29-December
conference,
National
the Dually
Diagnosed,
Towers
Hotel, Orlando,
Georgi
M. Hockaday,
ment
Excellence,
Inc.,
Dayton,
Ohio
45401;
&x 513-223-6307.
2, annual
Association
for
Radisson
Twin
Florida. Contact
CAE,
Manage-
P.O.
Box 2307,
513-223-8008,
November
30-December
1, conference on integrating
in-home
psychiatric care with partial
hospitalization
and
outpatient
services,
sponsored
by Global Business
Research,
the Fontainebleau
1112
Hilton,
Miami
Beach.
Con-
tact Conference
151 West
19th
York,NewYork
fax 212-645-4490.
Administrator,
GBR,
Street,
8th Floor, New
1001 1;800-868-7
188,
versity,
1823
nessee
37235;
327-7078.
Station
B, Nashville,
Ten615-327-7200,
fax 615-
December
1 3-17,
fill meeting,
Amencan
Psychoanalytic
Association,
the
Waldorf-Astoria
Hotel,
New York City.
Contact
APA, 309 East49th
Street, New
York, NewYork
10017;
212-752-9450,
extension
28.
December
December
tion deficit
cycle,
1-2, conference
on attendisorders
across the life
sponsored
by the Cambridge
Hospital
and Harvard
Medical
School,
Cambridge,
Massachusetts.
Contact
Judy
Reiner Platt, Ed.D.,
Cambridge
Hospital Professional
Services,
1 30 Bishop
Allen
Drive,
Cambridge,
Massachusetts 02139; 617-864-6165.
December
1-3,
annual
meeting,
American
Academy
of Psychiatrists
in Alcoholism
and Addictions,
Ritz
Canton
Hotel,
Amelia
Island,
Florida.
ContactJeanne
G. Trumble,
M.S.W., Executive
Director,
AAPAA,
8340 Mission
Road, Suite B-4, Prairie
Village,
Kansas
66206;
913-341-6680,
fax 913-6422431.
7-8,
conference
on disease
management
in behavioral
health care, sponsored
by the Instinote for Behavioral
Healthcare
and
CentraLink,
Ritz Carlton
Phoenix,
December
Phoenix,
Arizona.
rail, CentraLink,
Suite
108,
Portola
Contact
Tim
Har4370
Alpine
Road,
Valley, California
415-851-8411,
fax 415-851-
94028;
0406, e-mail tharrall@ix.netcom.com.
December
7-10, behavioral
therapy
institute on clinical consultation,
sponsored by the Obsessive-Compulsive Foundation, Interlaken Inn, Lakeville, Connecticut. Contact Institute
Planner, OCF, P.O. Box 70, Milford,
Connecticut 06460; 203-878-5669.
December
American
11-15,
annual meeting,
of Neuropsychopharmacology,
Caribe Hilton, San
Juan,
Puerto Rico. Contact Oaldye Ray,
Ph.D., Secretary,ACN, Vanderbilt UniCollege
Psychiatric
Services
1996
January
January
8-10,
international
conven-
iion of biological
psychiatry,
sponsored by the World
Psychiatric
Association
and the Indian
Psychiatric
Society,
Bombay,
India.
Contact
Amnesh K. Shrivastava,
Convenon,
Biological Psychiatry
Section,
IPS, Silver Mind
Hospital,
Shivknipa
Complex,
Gokhale
Road,
Thane,
Bombay
400 602, India;
91-22-539-1734,
fx 91-22-533-1084.
January
18-20,
havioral
healthcare
conference
outcomes
on
agement,
sponsored
by the
for Behavioral
Healthcare
traLink,
Red Lion Hotel,
be-
manInstitute
and Cen-
Costa
Mesa,
California.
Contact
Tim Harrall,
CentraLink,
4370
Alpine
Road, Suite 108,
Portola
Valley,
California
94028;
415851-8411, fax 415-851-0406,
e-mail
tharnall@ix.netcom.com.
18-2 1, midwinter
meeting
on the psychobiology
of personality
disorders,
sponsored
by the American Psychiatric
Association
and the
Colorado
Psychiatric
Society,
Sonnenalp Hotel, Vail, Colorado. Contact
Meetings Department, Colorado Psychi-
January
atric Society,
4596
East
Suite B, Denver,
Colorado
759-6045,
fax 303-759-6041.
huff Avenue,
80222;
303-
January
23-26,
winter
Royal College
of Psychiatrists,
meeting,
Harno-
gate, England. Contact Confrence
(Continued
November
1995
on page
Vol.46
Sec1126)
No.
11
4. Sharpley
cally
related
to trazodone,
nefazodone
has not been
associated
with
side effects such as priapism
and sig-
Drug
nificant
with drugs metabolized
by that system. Coadministration
of nefazodone
with terfenadine
or astemizole
is contraindicated,
because
carditoxicity
may result
(6). The clinician
may
need to reduce the dose ofother
drugs
orthostasis,
associated
which
with
have
trazodone.
been
There
is
of
no evidence
of potential
for abuse
nefazodone.
Overdosage
with
tion
ofup
not
to 11,200
proved
life
inges-
mg perday
threatening
has
or fatal.
Three areas in which nefazodone
may be distinguished
from the tricyclics and SSRIs are its low incidence
ofsexual
side effects,
its normalizing
effects
on
effects.
sleep,
The
sexual
its
antianxiety
reported
side
gasmia,
and
incidence
effects,
of
including
impaired
anor-
erection,
and
im-
ejaculation,
associated
with
tricyclic
antidepressants
and SSRIs
ranges from 1 0 percent
to 60 percent.
paired
The
incidence
of sexual
side
reported
with
less than
Many
5 percent.
patients
treated
report
sleep
increased
nefazodone
continuation
for additional
tion.
Use
of
often
with
decreased
medication
Therefore,
nefazodone
sleep
or the
is
sleep
helps
among
and
awakenings
not
being
with
depression
an admixture
The
pear
to
effects
have
and
well
zodone
as antidepressant
established
in
toms.
the
reducing
In a study
using
Rating
Scale
for Depression,
of the
scale’s
anxiety
revealed
toms
may
ment
of the
with
another
nefazodone
study
effect
until
ment
(2).
of anxiety,
need
pine
1114
did
the
depression
sufficient
first
not
third
patients
who
also
neflizodone
therapy,
an
adjunctive
or other
for
anxiolytic.
MAOIs
with
of ne-
should
be
potentia-
An
Nefazodone
with
is a new
a dual
HT2
reuptake.
inhibition
The
efficacy
nefazodone
are
over
of
they
in
A
the
Unlike
antidepressants,
not
appear
treat-
mild
many
nefazodone
to
impair
sexual
and
it does not impair
sleep.
As a result
of its novel
and
selective
mode of action,
its antidepressant
efficacy,
and its favorable
side
effect
significant
profile,
nefazodone
potential
of major
although
show
such
for
the
an
benzodiaze-
within
the
U.S.
U.S.
tional
be
is included
The
one-year
$95
one-year
student
rate
be
will
and
see
U.S.
subscrip-
$33.50
within
outside
the
subscriptions
For
more
Business
on page
circulation
the
the
$22.50
Longer-term
tion,
$45
institu-
outside
tion
U.S.
be
$65 outside
and
be $7 5 within
rate will
and
will
The
the
if
31.
individual
rate
are available.
informa-
Information
1106
or call
department
at
1-800-368-5777.
Group
Eison
AS, Eison
MS, Torrente
JR, et a!:
Nefazodone:
preclinical
pharmacology
of
a new antidepressant.
Psychopharmacology Bulletin
26:311-315,
1990
2.
FeighnerJP,
Pambakian
R, Fowler
RC, et
al: A comparison
of nefzodone,
imipramine,
and placebo
in patients
with moderate to severe depression.
Psychopharmacology
Bulletin
25:219-221,
1989
major
the
card
1 996 one-year
The
U.S.
Read-
increase
issue.
subscription
the
1996.
,
rate
by December
subscription
in this
holds
depression.
the
subscribe
rates
will become
1
avoid
treat-
1.
symptoms
may
in subscription
U.S.
References
of treat-
eliminating
ers can
medication’s
generally
time.
increase
effectivejanuary
ofaction-5and
ment
of major
depressive
disorder
appears
comparable
to that of imipramine.
Adverse
effects
associated
of treat-
(5),
alone
Increase
to PsychiatricServices
antidepressant
mechanism
antagonism
serotonin
decreased
with
Notice
of
Subscription
Rate
activity.
to
symp-
week
show
potentiated
for Readers
factor
week
For
not
APA’s
related
be significantly
end
Pharmacogenetics
and drug
of
newer
antidepressant
Journal
of Clinical
Psychiatry
suppl):38-45,
1994
metabolism
meta-
symp-
anxiety
CL:
the
Hamilton
items
1994
DeVane
is not affected.
psychomotor
ef-
ofpossible
ofserotonin
ment
medication’s
the
that
ef-
of nefa-
anxiety
analysis
by the
ap-
antianxiety
studies
However,
are
because
234-241,
6.
carbamaz-
is taken
together
The combination
with
avoided
5. Fontaine R, Ontiveros A, Elie R, et a!: A
double-blind
comparison
of nefazodone,
imipramine,
and placebo
in major depression. Journal
of Clinical
Psychiatry
55:
agents.
55(Dec
function,
symp-
SSRIs
significant
Premarketing
efficacy
of alcohol
when
alcohol
nefazodone.
Psychiatry
1992
medications
blockers,
and cisapride.
fects
system
triazolam,
bolism
of lorazepam
The cognitive
and
other
often
of anxiety
tricyclics
as
fects.
channel
does
Patients
toms.
calcium
31:1070-1073,
together
AES, Cowen
PJ: Neantidepressant-may
REM sleep. Biological
increase
interact
P4503A4
These
alprazolam,
and decrease
treated
for depression.
have
nefazodone.
epine,
P4503A4
may
prescribed
include
with
surprising
to normalize
patients
the
are
antidepressant
is associated
of
it
in-
medica-
light-stage
by
they
with
and
Conclusions
and
hypnotic
frequency
metabolized
when
the
system
AL, Walsh
novel
fazodone-a
SSRIs
awakenings.
result in dis-
of nefazodone
decreased
that
sleep
ofthe
need
(4).
with
inhibits
isoenzyme
fazodone
been
including
light-stage
Nefazodone
tion
disturbances,
creased
frequency
These side effects
effects
has
interactions
3.
Rickels
K, Schweizer
E, Clary
C, et a!:
Nefazodone
and
imipramine
in major depression:
a placebo-controlled
trial. British Journal
of Psychiatry
164:802-805,
subscriptions
to PsyServices are available
at
greatly discounted rates through
APA’s Psychiatric Services Rechiatric
source Center, which also
offers
a number
of other benefits for
mental health facilitiesand organizations. For more information, see page 1201 of this issue
or contact Mary Ward
at 202682-6173.
1994
Psychiatric Services
November
1995
Vol.46
No.
11
VENLAFAX/NE
HCI
A Serotonin
and Norepinephrine
Reuptake
Inhibitor
“Investigations of the action mechanisms of antidepressants
have provided support for the importance of fserotonin
and norepinephrinej
interactions in the patho physiology
of depression.”
-reported
Pharmacologic
Uptake
Inhibition
Compound
NE
5HT
TCAs23
,
1.##*
=
strong
Muscarinic
Affinities
Histaminergic
Adrenergic
affinity.
norepinephrine;
5HT
=
serotonin; TCA
The clinical significance
*Serotonin
Receptor
4#
i,##
EFFEXOR5
=
activity
/
SSRIs4
NE
in Kalus et al
reuptake
inhibition
tricyclicantidepressant; SSRI
of these in vitro data
varies
#{149}Like SSRIs and TCAs,
#{149}As with
=
among
=
selective serotonin
reuptake
inhibitor.
is unknown.
TCAs.
EFFEXOR
SSRIs, anticholinergic-like
is a weak
inhibitor
side effects
#{149}EFFEXOR
is a structurally
novel antidepressant,
to any other available antidepressant5
of dopamine
may occur
with
reuptake
EFFEXOR
and is chemically
unrelated
EXPAND
TREATMENT
YOUR
POSSIBILITIES
An effective
first-line
depressed
patients
Response
depressed
in
#{149}
EFFEXOP.
n
#{149}
Imipramine
n =
#{149}
Placebo
n
Baseline
I
therapy
=
=
for
outpatients’
39
33
47
2
3
4
6
Time (weeks)
No significant difference
between
EFFEXOR
and imipramine
was observed.
Significant difference
*Response
(P < 0.05); venlafaxine
and imipramine>
placebo at week 6.
to treatment
was defined as CGI improvement
score of I (very much improved)
2 (much improved).
In one randomized,
on venlafaxine
double-blind,
or imipramine
placebo-controlled
study of depressed
at 75 mg to 2.25 mg daily in divided
The effectiveness of EFFEXOR in long-term
cally evaluated in controlled trials.
patients
initiated/maintained
doses (observed
use (>6 weeks)
or
cases at week
6).’
has not been systemati-
EFFEXOR
Is contraindicated
in patients taking monoamine
oxidase inhibitors (MAOIs).
EFFEXOR
should not be used in combination
with an MAOI or within at least 4 days of discontinuing
treatmont with an MAOI because of potential
for serious adverse reactions.
Based on the half-ilk
of
EFFEXOR,
at least 7 days should be allowed after stopping EFFEXOR
before starting an MAOI.
Treatment
with EFFEXOR
is associated with sustained increases in blood pressure (BP) in some patients.
These appear to be dose dependent
and were seen at an incidence of >5% at dosages above 200 mg/day.
Regular monitoring
of BP is recommended.
As with any psychotropic
drug, EFFEXOR
may impair judgment, thinking,
should be advised to exercise caution until they have adapted to therapy.
The most common adverse events reported
in EFFEXOR
placebo) were: nausea, somnolence,
dry mouth, dizziness,
abnormal ejaculation/orgasm,
and anorexia.’
Please see brief summary
or motor
skills, and patients
clinical trials (incidence >10% and
2x that of
constipation,
nervousness,
sweating, asthenia,
of prescribing information on last page of this advertisement.
VENLAFAXINE
HCI
25 mg, 37.5 mg, SO mg, 75 mg, and 100 mg
Brief Summary
See package need for full prescribing information.
Clinical Pharmacology: The antidepressant action of venlafaxine is believed to be associated with
potentiation of neurotransmitter
activity in the CNS. In preclinical studies, venlafaxine and its
active metabolite, 0-desmethylvenlafaxine
(ODV). were potent inhibitors of neuronat serotonin and
norepinephrine reuptake and weak inhibitors of dopamine reuptakeVenlafaxine
and ODV have no
significant
aftinity for muscarinic,
histaminergic,
or a-i
adrenergic
receptors
in vitro.
Pharmacologic activity at these receptors is hypothesized to be associated with the various anticholinergic, sedative, and cardiovascular effects seen with other psychotropic drugs. Venlafaxine
and ODV do not possess monoamine oxidase (MAO) inhibitory activity.
indications and Usage: Effexor is indicated for the treatment of depression.
Contraindicatlons:
Contraindicated in patients with known hypersensitivity. Concomitant use in
patients taking monoamine oxidase inhibitors (MAOI5) is contraindicated
(see “Warnings”).
Warnings: POTENTIAL FOR INTERACTION WITH MONOAMINE OXIDASE INHIBITORS (MAOIs)Adverse reactions, some serious, have been reported when veniafaxine therapy is initiated
soon after discontinuation of an MAO1 and when an MAO1 Is initiated soon after discontlnuation of veniafaxine. Reactions have Included tremor, myocionus, diaphoresis, nausea, vomlt
ing, flushing, dizziness, hyperthermia with features resembling neuroieptic malignant syn
drome, seizures, and death. Given these reactions as well as the serious, sometimes fatal
interactions reported with concomitant or immediately consecutive administration
of MAOIs
and other antidepressants with pharmacological
properties similar to Effexor, do not use
Effexor in combination with an MAOI or within at least 14 days of discontinuing MAOI treatment.
Allow at least 7 days after stopping Effexor before starting an MAOI. Hyperthermia, rigidity,
myocionus, autonomic instability, mental status changes including extreme agitation progreasing to delirium and coma, and features resembling neuroleptic malignant syndrome have
been reported with concomitant selective serotonln reuptake inhlbitor/MAOI therapy. Severe
hyperthermia
and seizures, sometimes fatal, have been reported with concomitant tricyclic
antidepressants/MAOI
therapy.
SUSTAINED HYPERTENSION-Effexor
treatment is associated with dose-related sustained
increases in supine diastolic blood pressure. Regular monitoring of blood pressure is recommended, and, when appropriate, consider dose reduction or discontinuation.
Precautions: GENERAL-Anxiety
and Insomnia: Anxiety, nervousness, and insomnia have been
reported in short-term studies.
Changes in Appetite/weight: Anorexia has been reported in short-term studies, and a dose-dependent weight loss has been reported in patients taking Effexor for several weeks.
Activation of Mania/Hypomania:
Hypomania or mania has been reported; as with all antidepressants, use cautiously in patients with a history of mania.
Seizures: Seizures were reported in premarketing testing (0.26%). Use cautiously in patients with
a history of seizures. Discontinue it in any patient who develops seizures.
Suicide: The possibility of suicide attempt is inherent in depression and may persist until significant remission occurs. Closely supervise high-risk patients during initial drug therapy. Write
Effexor prescriptions for the smallest quantity consistent with good patient managementto reduce
risk of overdose.
Use in Patients with Concomitant Illness: Clinical experience with Eflexor in patients with concomitant systemic illness is limited. Use cautiously in patients with diseases or conditions that
could affect metabolism or hemodynamic responses. In patients with renal impairment (GFR=1O7OmL/min) or liver cirrhosis, clearance of venlafaxine and its active metabolite were decreased,
resulting in prolonged elimination half-lives. A lower dose may be necessary; use with caution in
such patients.
INFORMATION FOR PATIENTS-Clinical studies revealed no clinically significant impairment of psychomotor, cognitive, or complex behavior performance. However, caution patients about operating
hazardous machinery, including automobiles, until they are reasonably sure that Effexor does not
adversely affect their ability to engage in such activities. Tell patients to 1) notify their physician if
they become pregnant or intend to become pregnant during therapy, or ifthey are nursing; 2) inform
physicians about other medications they are taking or plan to take; 3) avoid alcohol while taking
Effexor; 4) notify their physicians if they develop a rash, hives, or related allergic phenomena.
DRUG INTERACTIONS-Cimetidine:
Use caution when administering Effexor with cimetidine to
patients with pre-existing hypertension or hepatic dysfunction, and the elderly. Drugs Inhibiting
Cytochrome P,IID, Metabolism: In vitro, venlafaxine is metabolized to its active metabolite,
0-desmethylvenlafaxine
(ODV), via cytochrome P4,lID,. Therefore drugs inhibiting this isoenzyme
could potentially increase plasma concentrations
of venlafaxine and decrease concentrations of
ODV. Drugs Metabolized by Cytochrome PlID6:
In vitro, venlafaxine is a relatively weak inhibitor
of this isoenzyme; clinical significance
is unknown.
Monoamine
Oxidase Inhibitors:
See
Contraindications” and “Warnings.” CNS-Active Drugs: Use of venlafaxine with CNS-active
drugs has not been systematically evaluated; therefore, use caution when administering Effexor
with such drugs.
CARCINOGENESIS. MUTAGENESIS, IMPAIRMENT OF FERTILITY-Carcinogenesis:
In 18-month
studies, there was no evidence of carcinogenicity in mice given 120mg/kg/day (16 times the maximum recommended human dose (MRHD)]. In 24-month studies, there was no evidence of carcinogenicity in rats given 120mg/kg/day.
Mutagenicity: In male rats receiving 200 times (on a
mg/kg basis) the MRHD, chromosomal
aberrations were found in the bone marrow in vivo.
Impairment ofFertiity: No impaired reproductive function was found in rats given 8 times (mg/kg)
the MRHD.
PREGNANCY-Teratogenic
Effects-Pregnancy
Category C. Reproduction studies in rats given 11
times, and rabbits given 12 times the MRHD (on a mg/kg basis) revealed no malformations of offspring. However, in rats given 10 times the MRHD, there was a decrease in pup weight, increase
in stillborn pups, and an increase in pup deaths during the first 5 days of lactation when dosing
began during pregnancy and continued until weaning. There are no adequate and well-controlled
studies in pregnant women; use Effexor during pregnancy only if clearly needed.
LABOR, DELIVERY, NURSING-The effect on labor and delivery in humans is unknown. It is also
not known whether Eftexor or its metabolites are excreted in human milk; exercise caution when
administering to a nursing woman.
PEDIATRIC USE-Safety
and effectiveness in children (<18 years) have not been established.
GERIATRIC USE-In clinical trials, 12% of Effexor-treated patients were 65 years of age. Overall
differences in efficacy or safety in the elderly have not been demonstrated, however, greater sensitivity of older patients should not be ruled out.
Adverse Reactions: ASSOCIATED WITH DISCONTINUATION OF TREATMENT-Nineteen
percent
(537/2897) of Effexor patients in clinical trials discontinued treatment due to an adverse event. The
more common events (1% associated with discontinuation and considered to be drug-related
included: somnolence, insomnia, dizziness, nervousness, dry mouth, anxiety, nausea, abnormal
ejaculation (male), headache, asthenia, and sweating.
INCIDENCE IN CONTROLLED TRIALS-Commonly
Observed Adverse Events in Controlled
Clinical Trials: The most commonly observed adverse events associated with the use of Effexor
incidence of 5% or greater and incidence for Effexor at least twice that for placebo): asthenia
12% vs. 6%), sweating (12% vs. 3%), nausea (37% vs. 11%), constipation
(15% vs. 7%),
anorexia (11% vs. 2%), vomiting (6% vs. 2#{176}!.),
somnolence (23% vs. 9%), dry mouth (22% vs.
11%), dizziness (19% vs. 7%), nervousness (13% vs. 6%), anxiety (6% vs. 3%), tremor (5% vs.
1%), blurred vision (6% vs. 2%), abnormal elaculation/orgasm male (12% vs. <1%), and male
impotence (6% vs. <1%).
Adverse Events Occurring atan Incidence of 1% or More Among Effexor-Treated Patients: The following occurred in 4- to 8- week placebo-controlled
trials, with doses of 75 to 375 mg/day, at a
frequency of 1% or more. This includes patients with at least one episode of an event at some time
during treatment. Body as a Whole: headache, asthenia, infection, chills, chest pain, trauma.
Cardiovascular:
vasodilatation,
increased blood pressure! hypertension, tachycardia, postural
hypotension. Dermatological:
sweating, rash, pruritus. Gastrointestinal:
nausea, constipation,
anorexia, diarrhea, vomiting, dyspepsia, flatulence. Metabolic: weight loss. Nervous System:
somnolence, dry mouth, dizziness, insomnia, nervousness, anxiety, tremor, abnormal dreams,
hypertonia, paresthesia, libido decreased, agitation, confusion, thinking abnormal, depersonalizalion, depression, urinary retention, twitching. Respiration: yawn. Special Senses: blurred vision,
taste perversion, tinnitus, mydriasis. urogenital
System: abnormal ejaculation/orgasm,
impotence, urinary frequency, urination impaired, orgasm disturbance, menstrual disorder.
Studies indicate a dose dependency for some ofthe more common adverse events associated with
Effexor use. There also was evidence of adaptation to some adverse events with continued Effexor
therapy over a 6-week period.
Vital Sign Changes: In clinical trials, Effexor was associated with a mean increase in pulse rate of
about 3 beats/mm, and a dose-dependent increase in mean diastolic blood pressure of 0.7 to
2.5 mmHg.
Laboratory Changes: During clinical trials, only serum cholesterol exhibited statistically significant
differences from placebo (increases of 3 mg/dL from baseline); clinical significance is unknown.
ECG Changes: Only heart rate exhibited a statistically significant difference, with mean increases
of 4 beats per minute from baseline.
OTHER EVENTS OBSERVED DURING THE PREMARKETING EVALUATION OF EFFEXOR-During
premarketing assessment, multiple doses of Effexor were administered to 2,181 patients, and the
following adverse events were reported. Note: “frequent” = events occurring in at least 1/100
patients; “infrequent” = 1/100 to 1/1000 patients; “rare” = less than 1/1000 patients. Events are
classified within body system categories and enumerated in order of decreasing frequency using
the definitions above. It is important to emphasize that although the events occurred during
Effexor treatment, they were not necessarily caused by it.
Body as a Whole - Frequent: accidental injury, malaise, neck pain; Infrequent: abdomen enlarged,
allergic reaction, cyst, face edema, generalized edema, hangover effect, hernia, intentional injury,
moniliasis, neck rigidity, overdose, chest pain substernal, pelvic pain, photosensitivity
reaction,
suicide attempt; Rare: appendicitis, body odor, carcinoma, cellulitis, halitosis, ulcer, withdrawal
syndrome. Cardiovascular
system - Frequent: migraine; Infrequent: angina pectoris, extrasystoles, hypotension, peripheral vascular disorder (mainly cold feet and/or cold hands), syncope,
thrombophlebitis;
Rare: arrhythmia,
first-degree
atrioventricular
block, bradycardia,
bundle
branch block, mitral valve disorder, mucocutaneous
hemorrhage, sinus bradycardia, varicose
vein. Di#{231}estive
system - Frequent: dysphagia, eructation; Infrequent: colitis, tongue edema,
esophagitis, gastritis, gastroenteritis, gingivitis, glossitis, rectal hemorrhage, hemorrhoids,
melena, stomatitis, stomach ulcer, mouth ulceration; Rare: cheilitis, cholecystitis, cholelithiasis,
hematemesis, gum hemorrhage, hepatitis, ileitis, jaundice, oral moniliasis, intestinal obstruction,
proctitis, increased salivation, soft stools, tongue discoloration,
esophageal ulcer, peptic ulcer
syndrome. Endocrine system - Rare: goiter, hyperthyroidism,
hypothyroidism.
Hemic and lymphatic system - Frequent: ecchymosis;
Infrequent: anemia, leukocytosis,
leukopenia, lymphadenopathy, lymphocytosis, thrombocythemia,
thrombocytopenia,
WBC abnormal; Rare:
basophilia, cyanosis, eosinophilia, erythrocytes abnormal. Metabolic and nutritional - Frequent
peripheral edema, weight gain; Infrequent: alkaline phosphatase increased, creatinine increased,
diabetes mellitus, edema, glycosuria, hypercholesteremia,
hyperglycemia,
hyperlipemia, hyperuricemia, hypoglycemia, hypokalemia, SGOT increased, thirst; Rare: alcohol intolerance, bilirubinemia, BUN increased, gout, hemochromatosis,
hyperkalemia,
hyperphosphatemia,
hypoglycemic reaction, hyponatremia, hypophosphatemia,
hypoproteinemia,
SGPT increased, uremia.
Musculoskeletal system - Infrequent arthritis, arthrosis, bone pain, bone spurs, bursitis, joint
disorder, myasthenia, tenosynovitis;
Rare: osteoporosis. Nervous system - Frequent: emotional
lability, trismus, vertigo; Infrequent
apathy, ataxia, circumoral paresthesia, CNS stimulation,
euphoria, hallucinations, hostility, hyperesthesia, hyperkinesia, hypertonia, hypotonia, incoordination, libido increased, myoclonus, neuralgia, neuropathy, paranoid reaction, psychosis, psychotic
depression, sleep disturbance, abnormal speech, stupor, torticollis; Rare:akathisia, akinesia, alcohol abuse, aphasia, bradykinesia, cerebrovascular accident, loss of consciousness, delusions,
dementia, dystonia, hypokinesia, neuritis, nystagmus, reflexes increased. Respiratory system Frequent bronchitis, dyspnea; Infrequent asthma, chest congestion, epistaxis, hyperventilation,
laryngismus, laryngitis, pneumonia, voice alteration; Rare: atelectasis, hemoptysis,
hypoxia,
pleurisy, pulmonary embolus, sleep apnea, sputum increased. Skin and appendages - Infrequent
acne, alopecia, brittle nails, contact dermatitis, dry skin, herpes simplex, herpes zoster, maculopapular rash, urticaria; Rare:skin atrophy, exfoliative dermatitis, fungal dermatitis, lichenoid dermatitis, hair discoloration, eczema, furunculosis, hirsutism, skin hypertrophy, leukoderma, psoriasis, pustular rash, vesiculobullous
rash. Special senses - Frequent abnormal vision, ear pain;
Infrequent cataract, conjunctivitis, corneal lesion, diplopia, dry eyes, exophthalmos, eye pain, otitis media, parosmia, photophobia, subconjunctival
hemorrhage, taste loss, visual field defect;
Rare: blepharitis, chromatopsia, conjunctival edema, deafness, glaucoma, hyperacusis, keratitis,
labyrinthitis, miosis, papilledema, decreased pupillary reflex, scleritis. Urogenital system Frequent: anorgasmia, dysuria, hematuria, metrorrhagia , urination
impaired, vaginitis”;
Infrequent albuminuria, amenorrhea” , kidney calculus, cystitis, leukorrhea, menorrhagia”,
noctuna, bladder pain, breast pain, kidney pain, polyuria, prostatitis” , pyelonephritis, pyuria, urinary
incontinence, urinary urgency. uterine fibroids enlarged”, uterine hemorrhage” , vaginal hemorrhage”, vaginal moniliasis”;
Rare: abortion” , breast engorgement, breast enlargement, calcium
crystalluria,
female lactation”,
hypomenorrhea,
menopause” , prolonged erection”,
uterine
spasm. (“Based on the number of male or female patients as appropriate.)
Drug Abuse And Dependence: CONTROLLED SUBSTANCE CLASS-Effexor
is not a controlled
substance. In a retrospective survey of new events occurring during taper or following discontinuation, the following occurred at an incidence of5%, with incidence for Effexor at least twice that
for placebo: asthenia, dizziness, headache, insomnia, nausea, and nervousness. Taper the dose
gradually and monitor the patient. Evaluate patients carefully for history of drug abuse and
observe such patients closely for signs of Effexor misuse or abuse (e.g. development of tolerance,
incrementations of dose, drug-seeking behavior).
Dosage and Administration: The recommended starting dose is 75mg/day in 2 or 3 divided
doses, taken with food. If needed, dose increments of up to 75mg/day should be made at intervals of no less than 4 days. Maximum recommended dose, for use in severely depressed patients,
is 375mg/day, in 3 divided doses. When discontinuing Effexor after more than 1 week of therapy,
the dose should be tapered to minimize the risk of discontinuation symptoms.
SWITCHING PATIENTS TO OR FROM A MONOAMINE OXIDASE INHIBITOR
At least 14 days should elapse between discontinuation of an MAOI and initiation of therapy with
Effexor. In addition, at least 7 days should be allowed after stopping Effexor before starting
an MAOI (see “Contraindications”
and “Warnings”).
Please consult full prescribing information for detailed dosing instructions.
This brief summary is based on CI 4193-2, issued May 23, 1994.
References: 1 Kalus 0, Asnis GM, van Praag HM. The role of serotonin in depression. Psychiatric
Annals. 1989;19:348-353.
2. Preskorn SH, Burke M. Somatic therapy for major depressive disorder: selection of an antidepressant.
J C/in Psychiatry. 1992;53(suppl):5-18.
3. Richelson E.
Synaptic pharmacology
of ant/depressants:
an update. McLean Hosp J. 1988;8:67-88.
4. Physicians’ Desk Reference’. 48th ed. Montvale, NJ: Medical Economics Co Inc; 1994;
Prozac’:877-880;
Zoloft’:2000-2003;
Paxil#{176}”:2267-2270.5. EFFEXOR#{176}
prescribing information,
Wyeth-Ayerst Laboratories, Philadelphia, PA. 6. Data on file, Wyeth-Ayerst Laboratories.
WYETH-AYERSF
a
В© 1994, Wyeth-Ayerst Laboratories
83561
LABORATORIES
August 1994
]IRIEALTIH[
NEWINPAPERBAO(
AFFAIS
“[A]
compelling
phy
of an acute psychiatric
coln1d1}r
unit.
A fascinating
account that describes how
the staff of such a unit
managed briefly to treat
and then �place’ the often
poor and destitute
.
Mceiniftai IRleatllth
in th
age
ethnogra-
f
.
.
emergency
Miia#{236}gcd1
C&ur
patients.”
-Contemporaty
“Rhodes’
Sociology
observations
are
I
_.j
couched in the theoretical formulations
of
Michel Foucault.
The
description of the unit’s activities
are bloodcurdling
and funny and precisely accurate.
A readable, accurate, and a’arming work of
-;
-
Philip
Boyle
ethical
and
Daniel
on the
Callahan
ramifications.
Susan
states
Essocic and Howard Goldman on how
are catching up with the marketplace.
Roger
Meyer
and
Stuart
care and the training
Mary Jane England
can improve mental
Anthony
of life.
Lehman
-
.
Journal
of Psychiatry
MP1YING
BEDS
of psychiatrists.
The Work of an Emergency
and Robert Cole on how we
health care for children.
on improving
.
-
anthropology.”-American
on managed
Sotsky
.
Psychiatric
Unit
LORNA A. RHODES
Comparative Studies of Health Systems & Medical Care
$12.95 paper at bookstores or order tolL-free 1-800-822-6657.
the quality
Lt1IVRSITY
OfCAVIORNIA
PR(SS
Richard Frank, Tom McGuire,
Nwhouse
on risk contracting.
and Joe
Barbara Burns and colleagues on the Great
Smoky Mountains Study: Children’s Mental
Health Service Use Across Sectors.
U
Order your copy today!
I
Call 1-800-765-7514.
7y a new
can easily
ofyour clienL
Why einvetU
die wheel?
gtvup approach
thoiyou
adjust
to meet die needs
S
U
and improves
competence
Staff or clients
can be instant
teachers
Flexible
format for all mental
health
settings
Inexpensive
and fun
Raises
self-esteem
HEALTH AFFAIRS
22i:iiiii’
Fall 1995, 288 pgs.
In the U.S. and
)“,
Canada,
.#{176}-Mai
�a
$25 each.
Bulk discounts
available:
-
inquire.
please
Ask about
subscriptions
to
Sa1
Instructr
Innwathne
and Student
Roleplaylng
11 ABC’s
Courses:
#{149}
Keeping
#{149}
Handling
in Shape
Medication
Decisions
#{149}
Making
Games.
#{149}
Handling
Hassles
a Friend
#{149}
Managing
Money
#{149}
Being
#{149}
Handling
for Children
#{149}
Understanding
#{149}
Caring
#{149}
Preventing
Guides.
Card
Anger
#{149}
Being
Creative
Mental
Accidents
illness
and
Crimes
HEALTH AFFAIRS, and
1
stay
informed
health
about
Please
policy issues
call orse,sd
for afree
brochure.
Each Course
is $45.00
Telephones
: 718-430.3353
1-800.925-8025
FAX: 718-931-7307
year-round.
ABC’S
SKILLS
P.O. Box 148, Congers,
Tel: 800-765-7514.
NY 10920.
Fax: 914-267-3479.
ACURRICULUM
FOR
LIVING
Jack F. Wilder,
Mental Health
Albert Eiftstein
1300
Bmnx,
MorrIs
New
M.D.
Education
College
Park
York
Pmgram
of Medicine
Avenue
10461-1602
VIIe’ve changed
our name and
our video collection!
expanded
he APA’s Psychiatric Services
Resource Center Video Library
you knew us as the H&CP
Service Video Rental Library
now has a collection of close to
250 videos on mental health and
related issues. Check them out!
j
-
!J
New titles include:
ADHO in Adults
Building Bridges:
Hispanics
A Guide for Interviewing
The Drop-In Group
DSM IV: New Diagnostic
Family Assessment
.
Issues
Hospital Without Walls
The Psychoeducational
Profile
Stressfullssues
for Clinical Clerks
The Touching Tree Winner ofthe 1994 H&CP
Institute Video Award!
-
Understanding
and Communicating
with a
Person Who is Hallucinating
.
What is Schizophrenia?
All videos have been reviewed and selected for
their usefulness in stafftraining,
patient support,
family education,
Yes! Send our facility
a FREE COPY of the 1995 Video Rental
Library Catalog.
Also send information
Psychiatric
Services
about how our facility
Resource
can join the
and community service.
If your facility’s
Psychiatric
not yet a member
Services
1400k
Po u
Stunt
310
30-
3)0
D uonuutuu
005
u Cutour
D7Sr/u31?
DC 20005 iPirune
Center,
now’s the time to join.
Center.
In addition to discounted
A 13110
Resource
of the
PS) ufriatoc
2026826173,
Fan
Association
202-682-6348)
facility will receive
group subscriptions
fees for video rentals, your
to the journal Psychiatric
Services
Facility
Psychiatric Practice & Managed Care, a
bimonthly newsletter
APAS Practice Guidelines series
Discounts for the Institute on Psychiatric
Services, APA Library Literature Searches,
Address
publications.
Name
Psychiatric
PS1195
-
Services Resource Center
isaprogram
of the
American Psychiatric
Association
APA
ference
March
Calendar
Department,
6000
Executive
Suite 5 13, Rockville,
Mary20853;
301-231-5484,
fax 301-
Boulevard,
land
1112)
(Continuedfrompage
231-7392.
March
retary,
RCP,
1 7 Belgrave
Square,
don SW1X
8PG, England;
2351, fax 11-071-245-1231.
Lon-
1 1-07
1-235-
24-26,
national
seminar
on
creating
employment
opportunities
for persons
with serious
psychiatric
disorders,
sponsored
by Matrix
Research
Institute,
Holiday
Inn IndeMall,
Barbara
Avenue,
Philadelphia.
Granger,
MRI,
Philadelphia,
19144; 215-438-8200,
1506, fax 215-438-8337.
Contact
6008
Wayne
Pennsylvania
TDD
treating
seminar
215-438-
on guidelines
addictions,
Cambridge
January
pendence
1-2,
for
sponsored
Hospital
and
by the
Harvard
Medical
School,
Boston. Contact
Reiner Platt, Ed.D.,
Cambridge
pital
Professional
Services,
1 30
Allen Drive, Cambridge,
02139; 617-864-6165.
March
ciation
6-9,
Hyatt
Regency
for
Judy
HosBishop
Massachusetts
annual
meeting,
AssoAcademic
Psychiatry,
Westshore,
02238;
Tampa,
617-499-5198,
March 7-10, biennial
meeting,
Society for Research
on Adolescence,
Westin Hotel, Boston. Contact Maryse
Richards,
Ph.D., SRA, Loyola Univer-
February
sity
of Chicago,
Department
of
Psy-
self-destructive
behavior
in children
and
adolescents,
sponsored
by Harvard
Medical
School
and the Cambridge
chology,
Chicago,
Hospital,
March
7-10,
third
annual
conference on using
behavioral
information services
and advanced
tech-
February
Platt,
2-3,
seminar
Boston.
Ed.D.,
Contact
Judy
Cambridge
fessional
Services,
Drive,
Cambridge,
02139;
on
Reiner
Hospital
1 30
Pro-
Bishop
Allen
nologies,
Massachusetts
February
12-17,
American
Group
Psychotherapy
meeting,
As-
sociation,
Hyatt
Regency
San
Hotel,
Franciso.
Contact
Karen O’Brien,
Education and Meetings
Director,
AGPA,
25 East 21st Street,
6th Floor,
New
York, New York 10010; 212-477-2677,
fax 212-979-6627.
26-28,
on
February
conference
service
health
national
children’s
research
mental
sponsored
by
systems,
the Research
and Training
Center
for Children’s
Mental Health,
Tampa,
Florida. Contact Krista Kutash, Ph.D.,
Deputy
Director,
Mental
Health
South
Florida,
Boulevard,
974-4661,
RTCMH,
Institute,
13301
Tampa,
Bruce
fax 813-974-4406,
of
B. Downs
33612;
813-
e-mail
kutash@hal.fmhi.usf.edu.
28-March
2, first international conference
on philosophy
and
mental
health,
sponsored
by the
Royal College
of Physicians,
Marbella,
Spain. Contact Mrs. Jean
Wales, RCP,
February
17
Belgrave
Square,
London
SW1X
11-071-235-2351,
fax
11-071-235-1231.
8PG,
1126
England;
fax 312-508-8317.
sponsored
by the
Institute
traLink,
4370
Alpine
Road, Suite 108,
Portola
Valley,
California
94028;
415851-8411,
fax 415-851-0406,
e-mail
tharrall@ix.netcom.com.
March 9-10, international
workshop
on cross-cultural
epidemiology,
phenomenology,
and nosology
in psychogeriatrics, sponsored
by the International
Psychogeriatric
Association,
India International
Centre, New Dehli.
Contact
IPA Secretariat,
1-3,
14th annual
3127
and
on
leisure
skills, sponsored
by the Medical
College of Pennsylvania
and Hahnemann University,
Adams Mark Hotel,
Philadelphia.
Contact Pat Lewis, Medical
College
of Pennsylvania,
3200 Henry
Avenue,
Philadelphia,
Pennsylvania
19129;
9028.
215-842-4380;
fax 215-843-
April 24-26,
seminar
on creating
employment
opportunities
for persons
with
serious
psychiatric
disorders,
sponsored
by Matrix Research
Instinate,
Executive
Tower
Inn, Denver,
Colorado. Contact Barbara Granger,
MRI,
6008 Wayne
Avenue,
Philadelphia,
Pennsylvania
19144; 215-438-8200,
fax 215-438-8337.
May
May 1-2, symposium
on excellence
in
the implementation
of computerbased
patient
record
systems,
sponsored by the Computer-Based
Patient
Record
Institute
and the Managed
Health
Care Technology
Institute,
Washington
Convention
Center, Washington,
D.C.
70 Blanchard
lington,
270-6000,
Contact
Road,
CPR/Healthlnfo,
Suite
4000,
Bur-
Massachusetts
0 1803;
617fax 617-270-6004,
e-mail
hlthinfo@nmhcc.com.
Greenleaf
60091;
708-
March
2 1-24,
14th annual
symposium
in forensic
psychiatry,
sponsored by the American
College of Forensic Psychiatry,
Chateau Sonesta Hotel, New Orleans.
Contact
Conference
Planner, ACFP, P.O. Box 5870, Balboa
Island,
California
92662;
714-8310236, fax 714-675-1107.
March 28-31,
national
conference
on
the impact
of stress,
trauma,
and
anxiety
on the family,
sponsored
by
the Anxiety
Disorders
Association
of
America,
Hyatt
Orlando,
Orlando,
Florida. Contact Jan Ross, ADAA
Con-
Psychiatric
conference
activities
TDD 215-438-1506,
Avenue, Wilmette,
Illinois
966-0063,
fax 708-966-9418.
Florida
University
Florida
6525 North
Sheridan
Road,
Illinois
60626;
312-508-
for Behavioral
Healthcare
and CentraLink,
New Orleans Macriot,
New Orleans.
Contact
Tim
Harrall,
Cen-
617-864-6165.
annual
3007,
April
therapeutic
Florida. Contact AAP Executive
Office,
Department
of Psychiatry,
Wyman
2,
Mount Auburn
Hospital,
Cambridge,
Massachusetts
fax 617-499-5498.
April
Services
**May
4-9, annual meeting,
Amencan Psychiatric
Association,
Jacob
Javits Convention
Center,
New York
City. Contact George Campbell,
Director, Meetings
Management,
APA, 1400
K Street, N.W., Washington,
D.C. 20005;
202-682-6000;
fax 202-682-6114.
May 13-17,
meeting
on current
developments
in psychiatry
in France
and North
America,
sponsored
by
the Federation
Francaise
de Psychiatnie in collaboration
with the American Psychiatric
Association,
Paris,
France. Contact John A. Talbott,
M.D.,
645 West Redwood
Street, Baltimore,
Maryland
21201; fax 410-328-3693,
email
jtalbott@umpsy.ab.umd.edu.
November
1995
Vol.46
No.
11
MEDICAL
The
American
manage
APA
and
Psychiatric
the
operation
currently
the
day-to-day
of the
is seeking
oldest
medical
has approximately
direction
plans
psychiatric
and
care,
communication
international
Candidates
strong
of the
administration
strategic
policies,
40,000
a Medical
association
members,
Director
in the
a budget
presence
should
and
must
who
country.
of $26
will
The
million,
ability
Board
to develop
for quality
policy,
facilitates
a strong
leadership
and
to motivate
and
implementation,
with
education
member
national
and
curriculum
will be handled
letter
nominations
must
Medical
and
private
Search
P.O. Box 27876
Washington,
DC
academic
issues.
of the
APA.
and/or
nominations
Please
indicate
interest
Office
box
vitae.
be received
Director
employees.
involvement,
members
Applications
confidentially.
to the
advocacy
research
experience,
and
a strong
psychiatrists
by a detailed
management
members
prior
and
Employer.
APA
the
provides
efforts
maintains
Opportunity
cover
advocacy
experience,
be Board-certified
and
with
Director
Association.
clinical
familiarity
Medical
for Association
and
and
setting
All communications
and
major
demonstrated
include
be accompanied
Applications
works
develops
skills,
is an Equal
a CV
programs,
for the
have
of budget
submitting
of APA
involvement,
knowledge
APA
the
and
should
Candidates
of Trustees,
as spokesperson
interpersonal
background,
Board
acts
Background
must
Association
1 75 employees.
Under
The
DIRECTOR
20038-7876
Post
by January
Committee
listed
1, 1996.
below.
by
selective serotonin
reuptake hThibitor for OCD
A
fiuvoxamne
maeate
E&S
A SELECTiVE
SEROTONIN
INHIBITOR
REUPTAKE
EFFECTiVE
IN RELIEVING
THAT
IMPRISON
PATIENTS’
DEMONSTRATED
COMPULSIONS
RAPIDLY
ACHIEVES
SHORT
HALF-LIFE’
LOW
INCIDENCE
FAVORABLE
BLOOD
STEADY-STATE
OF AGITATION
SAFETY
OBSESSIONS
MINDSI*
AND
LEVELS;
(2% vs 1% for placebo)’
PROFILE
#{149}:#{149}
Relatively low incidence of anticholinergic
side effects in controlled trials of OCD and depression,
LUVOX Tablets vs placeb&: dizziness I 1% vs 6%;constipation
10% vs 8%; dry mouth 14% vs 10%
#{149}:#{149}
The most commonly observed adverse events compared to placebo were somnolence
22% vs 8%,
insomnia
21% vs 10%, nervousness 12% vs 5%, nausea 40% vs 14%, abnormal ejaculation 8% vs 1%,
asthenia 14% vs 6%’
#{149}:#{149}
Concomitant
FLEXIBLE
use of LUVOXTMTablets
monoamine
oxidase inhibitors
is not recommended’
DOSING
Dose: 50 mg once a day
Initial
HS
50-mg tablet
.�,
.-
and
Dose Range: 100 to 300
mg/day
#{149}Increaseby 50 mg increments
�is needed
#{149}BID
dosing
:
for over
recommended
ever
4 to 7 di s
100 mg/day
100-mg tablet
COMPREHENSiVE
DATABASE
SAFETY
(Worldde
Eposure
40 countries
+
Data from
+
Over 9 millionpatients
+
More than 37,000patientsstudied inclinical
trials
treated
LUVOXTM
fiuvoxamnemaleate
TARGETED
*Efftjven
Prescriben
FOR OBSESSIONS
TREATMENT
not established
beyond 10 weeks in controlled
should write the smalkst
Please see brief summary
COMPULSIONS
trials.
tablet quantity consistent
of prescribing
AND
information
with good
patient management toreduce
on adjacent page.
overdose
risk.
for
Reporting Overdose
t)1
LUVOX’
(fluvoxamine m.oteUobhis
BiiefStjmmoy (Forh Prescithinghifoimoh #{238}#{227}
to pockage inseit.)
DKAflONS AIS
*#{241}hwdRocacnhnlRi3
O&IdIdflIdrnDS*&
rK1RR,
chwoc
ths,
ceinoges(thsess#{243}e)
I
80 nw/&iy
L
dOmRJ&ERfS$m*nnOOI
thooithmsfrer
thmw,kcncl,d
OWRI1L
m#{224}R
L#{243}dMRUrY
ltR Sffed1iNOXRfliflICfl
Nm1 MsI.rs
cONTuII.IcATIONS
.eW**IGSPtICAM1OI6).
llXT,w*sth
kthRR
I1UIS6UflOWfl.
M&6dORRJRR1R&
aRfhNo*R*Rmi.
IIuIIGs
Piik
udN
.dsI
is#{224}I.dw
.
SulNm.Nhduu
tMI
..N
.
.s
Is.
,srb
d
114 ssu..
IN
,ss.#{225} Nu,ukIk.
I4#{224}i.sMAOL
si#{233}s.s.Thuih,
ThSTRROR*thS#{233}U9OMthIIDOc1RI
Uss
SiUX1b#{224}W
GsiIk Uss
flihs65dmsscbsmsd
mycps
i#{224}
*thuUssuspi.
h
MI*UIhUSt
UJVOXIsis
18oehowenbssn.st
Hw,
Comsqusn XTIV*R$ng
ADVSf RIACTIOI
2 wss
Is.
1_*d
thi hsism..i
s s
Iv
d
M #{233}s6
as.
.
s(i.ds.s
mowunsn I#{246}RdF,*p
aydose o mg/rn’eis)hdImiWOm#{224}*
sffee mo inua,
2 nss
mea,
ftJRES
fls
dXT1R
CInE
sposi& RInbIhmIOR
1Oweeks
Th#{227},#{224}aXTooMpedothcyreim$sIm
I
RO
dthiy.
I
(1%)
uss
, h ussss#{226}
AR.N4#{225}S, sd
hxs
.s Is
si ti. #{232}cpmfcs
U,dIIIh.bN5IUsUVSd
I
wUhuIh
Iuf.u,
ssissk
tht4phc#{225}o)E#{224}dhssds, *#{226}dQRIRPi
RRhYfl*k
j RXR*c$,
i&flU
flhIUR15SflU5
di.NICI#{225}d1i#{225}
.
mMO#{224}13ssI
(sss
ths
ds
oes
Ds
d5%Msth
M;PWAUUOIIS
bo) IfrOmTCUs
2 eve: nve
pod i 1
vcA
Usi, Ssmdkus
I.
WkOd
(e.Oom)
uM
(ei
ThthRb5RRthR?SmRSRith*SdL9
-
nma
R5RR#{228}l,
(1n
mRzIpRfl. RflR1
ecin
Ct
W1
,vua
*
nve*
events we emthsd
I%
th OLD,tetulosi
ANEwsO7iW.d
*Wpm*SaL
s*
dspssxak(6wssk)
dmi#{216}iPnsa
Rs_
1O3OOm
ntiz#{225}i
a
dsis
us thoss * #{232}ymoi
tasossdbA,, wflryksie
h2.wabssny
(1O
hdpstmsothgco
d 1%mmdsmas1thlipb#{225}R,
sc
so n
sthhnu*RR#{227}Jt
isi
OMRddUigRSRI1dOIdCOS1AR1bRS5d
UdionwyIsn#{225}i
Is*d
rWXT1s
dMgk.tSR*
msgab
im*spopst#{224}t
th
. AI.ksJy
PN4IC*UWSI.
BThrethammdavsmsIobah
s
hbdmgI*
AaEV.RSIOGI(I*SIIdS
?IthdEi
1.s
flsck,
hst
a Mti
I 1*
ssksart
*
D
Dasdss
*n
f#{225}#{225}
ic#{248}, nubse/*&
thist atk
bgoa
AIiWR!WEDYRR
msdcRI
atKD
(375ne442
4thso
mfls#{216}s)
12nuck
sv
ndsvams
Thsdewaesdthso#{216}Iswisdsasos
Wd%IsS
0)
dthsooL#{224}amc*
pRAdfRUMh
k&amias(5OOs
(2)
#{243}th1d
mrMihaaes
snresi
UX
Micoa
kiUMX1s
vs thioihion
ISOI
moi*sd
thi
Lsiwwy.qss
rs.d
Nodasos 4Ims
(anW5RR&&1Onaam#{224}a$ea1l
NICAIOI6
madVsRfltx
(1) dRn95frOmb5nSVRRWS6nJfl
ODOfldd5P1ISROR
(2)
nsnmniismiRtsondpocebo.
hen1oRiog w aiithhs
6.srd
Ec6
Rs1*athLGTiR.
n,ikssvvm
Miobyts
m
paw4o
1hs
S5iM
posviy asviddsIsi
#{241}wa
sthathsssoaw
pasay
PISSa&RUMtX
US.IMIII,R
Ms#{248}*
MIs 2 TlW1GBITAbYR
IIN
s*wcsnRpl:
C*IUIOV*SQJIAL
Pb(32).
ts,,_Iaaca_
bOkPRI dapi
zmodiv
CyPIieSdDd
weXTmaoveb
*mtsO,*
sun;
Usd.dsmA*n;
Oth hsutsUkins
LLMIXTJIe
PCPUtA11OIISCON
R6nmWs
i1d#{243}gcss#{231}
nn
sFNa.ke1k
tv#{224}..d
pa
Mskm#{226}
ks#{216}u
hc
MIRY1J,
UJVOXTsIs
C1kPasnISShCIMte
..
th WX 11
MMimdMoRaihUMXT
O*IDRfS$OU
;C*s(1OM;ips(1Ov&5);
1).NISohnce(22d);k&mi*2J
s. tO);yModh(t4vs
1O);Nsrusmss(12vs 5);Dizzie(11 vs6);Trsnu(5v& 1);k(S3);Voan’(3v&
1);etn(2vs
1);
Amon (2 vsM; Dsasos L#{252}
(2 v t); Dsrss (2 U; 06 Sn,iofl (2 v fl. RESPIRATORYSYSflUs UppaRsspo,y kIec (9 5);
Slt S,sai3).
SPEOMSBISUk TPaissiU3
1);M#{216}o(32). UIOGIUTAk Sns#{224}
ajoin’(8
1);3r2);kmssncs’(2
));M#{248}gOO);UiuyRs(1
SO).
1W#{224}RdeW.IS
C*MO6tUsgMoihets)
IYBITUIkI
IAUSSYKOYSYSUM
IUUYASWHOU
DIGtSUVESYS1
Us(4O14);mh(11
RthUMlXTs
AkkN.
e;RRJssocDRM*UsatdI.
thjthoos
odMA#{243}o#{224}.sss.venRaithc
addCOSTAUbsd
L#{226}.wws
ThPrRWstksRsonInsndst
iuiudIsm
bWurN
a
mwsdcnnmt
*l*sklszs
vp
U
a Ilsl#{225}#{225}adhy
Cyt.ka..
P450 .zp.ss
1) #{226}eod
hspk cptdvoms P450 (CYP450)
Th5hbRWhdg5cOnU
2,
ka#{224}pssn#{224}iUjss
a#{224}3)thmyaflsnolds
mP4ummbffia
v1Umski
a h
m OIR$RIR
Us4 ozia,
dkassoiad*s
9*a’i
IM-Aozoksn.
Evais s bifr dsd
w
hods*
bod spurn caisgodad emmisalsdm
ci dsashapany
uig afoksi
dthIRon
frSqUSRtRIaRsMnR
is
ith&isThioi#{224}avw#{225}
$is,aIaRMSIRd&
ibs1t6
isisiwsomdseoca,flnghith
1/)OOOsisr
(aJaR
s,
sL
AcUsJy *iissiEs
a voathaopsk
ipodji
d
wth imai
inizah,
ths
coda
s1LiIsddUIq
rn*isoh
U6S).
ka(a*Rh
hSe1ci&ROisrfln#{224}s1
moc*
mi
Ismdn.
daRxaia
aRlG*mi*wjE
SesUNGS.
izor
SasWMIG
qo
SssUPI6
Lzz
Ass$y
Wm#{224}kRSR (N=12) adasdisOmzspan
(4 nia)
edJci#{216}1a
ossogs, be mzepam wa ad bmzspavth bainlis so&ed iib
deesments mcoiM f#{252}ndi#{231}
asa, *a
1r bozipsn
d#{243}jcship ms ia.mi
sizspsn nt
LJai Is
Iw*cns
m
SsxihisbunmpoaRdwtIsco#{243}ion
kp*jir
mo.rmniIs
RRRm*JadId&Ma*.
aJad5R*
th’e
IRWIth
(5On
cao
b
isflmi5i#{216}OL
gaRei
M,oiuma iss*d oua
aRssopIucnthotp
w
asist
h*sqtm
timen#{188}i
mskn
fuiais
Syst
w
sn&s.
I#{243}
pithssrmi
Ri
aJ
U6dsprsa
si#{225}om1
w,sso
cois&
scams
ip:
laisneam
is otha) adnss
#{224}RPthMIeIIR
kvkh*i!eiis
(1Cm): S*aiyrnusasd
ce
mna.
(mnoNd*h*scte
dSmdWSaSIISdSpNd
moi
i
has
i
spaded shsn&iwoas
ndiRs
Mat
us,
opsd
flaR&WOW8IRIJaI*ES
Cothumoin
#{149}
hps#{224}n,
thap,iii;
ha,in
b*
hwoki*
ms
scka
#{233}
dsps#{224}sid
hodmn
s#{231}a,
sisiiiai;
w#{224}i#{232}sit
hsaJ
#{232}y
Rnd5OdIn5t
ii
hIsqat
aw
k1o1s dshskogioa
iewh
h.t
ho
Faat
laipiWarySys
idiksm#{243}spJacnay&ssasjns
#{224}sm svmaEi
*Ja
d*
isco1v,
hpefl ftxrim
*JaOmcbso
#{224}i
kcksa
a#{231}
ieisossd
h#{243}saf
iIaSiSiVI
iba
5psS
hIsat
Spamisi.#{225}’mos*msapaa,
msaithoo, mshonboo, noa
Ths#{241}p*s:
S.IIN6S.
pa
emsnsd
tie kiIkiOycflRIsmOIOIIImiO’,
spi#{232}ona,
wmy iecnnsni, ay
odited
wuuy gsn
Jinoi Ivpoie&va#{231}n
in
oiii
t,s
ntsao
Ius
NDdRRpO*JSI
)ravaith*nc
1Od*aismincaa
I#{243}R
IflO.
(tile
w mslopto auth mdsigo ap mebcn
snck
m#{225}io$
pmiy by rend sxaelioi Ufihr
See lN6S.
U#{231}oarIn*Od&JSOXIRm#{224}os
15mgdO#{226}fR
18 doi (N=8) nJcM$y
Jad*aimocokia1ksdo
1.25n#{216}4smisnivdas&
zin:
DiodycoJaIii i pon th a cothnioi
d Ikiwimia mi
i *zem.
z
ii SaJ
Smokis o 25%rnasosssa msRtha&vndSjaamisR
xaRm*as. Jaksi
Thay (ECTh 1hsteiermc*
a_a
aJR i sdccmb
isci ECTad&isiss
nss.
-
Ctsjsis#{224};
k
k
*y,
vhthIPRIdI
E&RdkCUR
.
dommmia
ththslss
dskm #{224}kab
#{231}ca’
hJeMo,
phoi
Sdss iscas
40 gdosssdsus
(iiaii
mcnsad
m
idhdi#{231}pamoiphommwdpioslaoIha.
beaRfpudsdth
thScOIJthRI1iOR&RRXaIR
RRN*,
Ciz#{231}ai:
mioN w ci,binozs
Akv#{225}a:5$cay
sveoead mhodons im
doa)
t
biayp
thck*
thIMia
xrgoia.
Us#{225}i4iISyItI.R
#{149}
ipi
pJaIOJ..
anrdozi
a,s,Ja
clnaJ,_
ms
(5On
TCAhsstsvs
mRthORC
ThsiusnosdanidcismogsiR
n1sidRiElimsWdtu*yM%,aernns
���“�
haisaRsoiL
flL OlTiRlikMdbL
cMmO*
3E1252
RQaRRRUsS.
isThiUsmwiyMme&ot
Rev 1/95
lderence:
1. Da61SolvayPhannzeudca1sjnc
m#{224}.
h#{225}
SOLVAY
i26tmi)mon
na mwintsn ho
&*,ss
i
a mqjm
saa#{226};
Reedenc.dnRsOgfl p*n
aisd24Oea#{243}maN#{234}6
w oeavsd ma mois misonudeus
SOLVAY
i
vude
&&#{149}
C 1995, Soay
L!J’
PHARMACEUTICALS
30062
Phanuaceuiica1
Inc
MI hgtns resenL
999217
USJ3863.OO
Sepenber
1995
charge
planning
functions
to perpetuate
homelessness
among
persons
with chronic
housing
instability.
Although
the number
of subjects
in the study was small,
the data suggest that inadequacies
in discharge
planning
are most apparent
for homeless subjects
with the triple disorders
of schizophrenia,
substance
abuse,
and antisocial
personality
disorder.
The act ofsigning
out ofthe hospital
against
medical
advice appears
to undermine
the staff’s efforts to conduct
adequate
discharge
planning.
However,
more
information
is
needed
about
the treatment
expeniences of homeless
men with schizophrenia and concurrent
substance
abuse
and antisocial
personality
disorder.
It is
possible
that patients
who traverse
the
roads between
jails, homeless
shelters,
and psychiatric
hospitals
(23-26)
are
the most difficult
to plan for because
they have the greatest
needs and the
fewest options
for adequate
housing
and treatment
in the community.
These characteristics,
combined
with
such patients’
greater
likelihood
of
refusing
treatment,
can present
serious management
problems
for inpatient staff, who are often compelled
by policy
mandates
to strictly
limit
length
ofhospital
stay.
The complex
interplay
between
treatment
refusal
and reduced
access
to needed
care is illustrated
by the
study
finding
that
antipsychotic
medications
were less likely
to be
prescribed
for homeless
subjects
than
for never-homeless
subjects.
Although
more information
is needed
about this important
issue, it is plausible that medication
was not prescnibed
for some homeless
subjects
because oftheir
past history of refusal
to comply
with medication
therapy.
Future
work
on service
use and
homelessness
should
focus
on the
problems
of treatment
refusal
and
service
access
among
severely
disabled
patients,
particularly
those
with comorbid
diagnoses
of schizophrenia,
substance
abuse, and antisocial personality
disorder.
We concur
with researchers
who have suggested
that successful
management
of such
patients
in community
settings
requires
specialized
supportive
housing and treatment
services
(27).
Psychiatric
Services
November
1995
16.
Acknowledgments
This
work
44705
was
supported
from
the
by grant
National
MH-
Institute
of
Mental Health.
The author thanks Patrick E. Shrout,
Ph.D.,
and Boanerges
Dominguez,
M.S., for their helpful
advice on the statistical
analysis.
1 . Bassuk
EL: The homelessness
problem.
Scientific
American
25 1 :40-45,
1984
2. Hopper
K, Hamberg
J: The Making of
America’s
Homeless:
From Skid Row to
New
Poor,
1945-1984.
New
York,
Community
Service
Society
of New
York, 1984
3. Baxter
E, Hopper
K: Troubled
on the
streets:
the mentally
disabled
homeless
poor,
in The Chronic
Mental
Patient:
Five Years Later. Edited
by TalbottJA.
Orlando,
Fla, Grune
& Stratton,
1984
4. Lamb
HR: Deinstimtionalization
and the
homeless
mentally
ill. Hospital
and Cornmunity Psychiatry
35:899-907,
1984
5. Lamb
HR: Will we save the homeless
mentally
ill? American
Journal
of Psychiatry
147:649-65
1, 1990
6. Homeless
Mentally
Ill: Problems
and
Options
in Estimating
Numbers
and
Trends.
Washington,
DC,
US General
Accounting
Office,
1988
7. Baxter E, Hopper
K: Private
Lives/Public Spaces:
Homeless
Adults
on the
Streets
of New
York. New York, Cornmunity
Services Society, 1981
8. Cohen NL, PutnamJF,
SullivanAM:
The
mentally
ill homeless:
isolation
and ad-
aptation.
chiatty
Hospitaland
35:922-924,
FischerPJ,BreakeyWR:
mental health:
1984
Homelessrssand
overview.
International
Journal
ofMental
Health
4:6-41,
1986
Sosin
MR.
Grossman
S: The
mental
healthsystem
and theetiologyofbomelessness: a comparison
study. Journal
o(Corn-
10.
an
19:337-351,1991
munityPsychology
11
Psy-
Community
.
Belcher
JR: On becoming
homeless:
a
study ofchronically
mentally
ill persons.
Journal
of Community
Psychology
17:
173-185,
1989
12.
Caton
CLM,
Shrout
PE, Eagle
Risk factors for homelessness
schizophrenic
men: a case-control
American
Journal
of Public
13.
Drake
RE, Wallach
Housing
instability
84:265-270,
among
PF, et at:
among
study.
Health
1994
MA,
Hoffman
and
homelessness
JS:
aftercare
patients
of an urban
Hospital
and Community
Psychiatry
40:46-5
1 , 1989
Drake
RE, Wallach
MA, Teague
GB, et
al: Housing
instabilityand
homelessness
among
rural
schizophrenic
patients.
American
Journal
of Psychiatry
148:
state hospital.
14.
330-336,
15.
1991
Susser
ES, Lin SP, Conover
SA: Risk
factors
for hornelessness
among
patients
admitted
to a state
mental
hospital.
American
Journal
of Psychiatry
148:
Rossi PH,WrightJD,FisherGA,etal:
urban
homeless:
estimating
The
composition
and size.Science 235:1336-1341,
18.
20.
21
22.
23.
.
1987
Susser
E, Struening
EL, Conover
S: Psychiatric
problems
in homeless men. Archives
of General
Psychiatry
46:845849,
1989
Caton
CLM:
The
Community
Care
Schedule. New York, New York State
Psychiatric
Institute,Jan
1989
First MB, Spitzer
RL, Gibbon
M, et at:
The Structured
Clinical
Interview
for
DSM-III-R Personality
Disorders,
Part
I , Description.
New
York,
New
York
State Psychiatric
Institute,
1993
Kay SR. Fiszbein
A,Opler
LA: The Posinyc
and
Negative
Syndrome
Scale
(PANSS) for schizophrenia.
SchizophreniaBulletin
13:261-275,
1987
HosrnerDW,LemeshowS:
Applied Logistic Regression.
New York, Wiley,
1989
Abram
KM,
Teplin
LA: Co-occurring
disorders
among
mentally
ill jail detainees.
American
Psychologist
46:
1036-1045,
1991
24.
Solomon
PL, DraineJN,
Marcenko
M, et
at: Homelessness
in a mentally
ill urban
jail population.
Hospital
and Commu-
25.
Michaels
D, Zoloth
SR. Alcabes
P, et at:
Homelessness
and indicators
of mental
illness among
inmates
in New York City
correctional
system.
Hospital
and Cornmunity
Psychiatry
43:150-155,
1992
Vitelli
R: Thehomeless
inmate
inamaximum
security
prison
setting.
Canadian
Journal
of Criminology,
July
1993,
nity Psychiatry 43: 169-1 7 1 ,
26.
1992
pp 323-33 1
27.
Gelberg
L, Linn LS, Leake
BD: Mental
health,
alcohol
and drug use, and criminat history
among
homeless
adults.
American
Journal
of Psychiatry
145:
191-196,
1988
J ournal
Care
Seeks
Success
Managed
Stories
Psychiatric
Servicer would
like to encourage
a dialogue
among
its readers
about
how to cope successfully
with
managed
mental
health
care.
The
journal
seeks case examples
or descniptions
of successful
model
programs
for a possible
future
section
in
the journal.
Potential
contributors
should send
a one-page
letter summarizing
the successful
experience
to John A. Talbott,
M.D., Editor, PsychiatricSenrces,
Amencan Psychiatric
Association,
1400 K
Street,
N.W.,
Washington,
D.C.
20005.
Longer articles
will be invited
based on review of the summary.
1991
1659-1664,
Vol. 46
JBW,
Gibbon
M:
Interview
for DSMDC, American
Psy-
chiatricPress, 1990
17.
19.
References
9.
Spitzer
RL, Williams
Structured
Clinical
HI-R.
Washington,
No.
11
1143
Health.
M.D.,
Ph.D.,
helpful
The authors
thank
Lisa Dixon,
Howard
H. Goldman,
M.D.,
and Eimer Keman,
M.S.W.,
for
comments.
pital
readmissions.
munity
15.
Hospital
and
Psychiatry 26:749-751,
Com-
Hospital
1975
Torrey FE: Violent
behaviorbyindividuals with serious
mental
illness.
Hospital
and Community
Psychiatry
45:65 3-
24.
1.
2.
Spilker
Clinical
1990
Swert
4.
Lehman
AF, Possidente
5, Hawker
F:
The quality
oflife
ofchronic
patients
in
a state hospital
and in community
residences. Hospital and Community
Psy-
chiatry 37:901-907,
5. Iamb
from
and
RH: What
did
we
really
26.
MillerDJ,
Beck NC, Fraps C: Predicting
rehospitalization
at a community
mental
health
center:
a double-crossed
validation.
Journal
of Clinical
Psychology
40:35-39,
1984
18.
Vaughn
27.
Goldman
HH,
JP, et al: Design
ation ofthe Robert
dation
Program
ness.
Hospital
28.
Derogatis
L: SCL-90:
Administration,
Scoring,
and Procedures
Manual-Il.
Baltimore,
Clinical
Psychometric
Research,
1983
29.
Lehman
AF: A quality
of life interview
for the chronically
mentally
ill. Evaluation and Program
Planning
11:51-62,
30.
Lehman
AF, Postrado
LT, Roth D, et al:
An evaluation
ofcontinuity
ofcare,
case
management,
and client outcomes
in the
Robert
Wood
Johnson
Program
on
chronic
mental
illness.
Milbank
Quarterly 72:105-122,
1994
family
Clarke
zation.
GJ: IndefenseofdeinstitutionaliMilbank
Memorial
Fund
19.
7.
8.
22.
Rice DP, Kelman
5, Miller
5: The economic
burden
ofmental
illness.
Hospital
and Community
Psychiatry
43:12271232,
1992
Mosher
LR, Menn AZ, Matthews
Soteria:
evaluation
ofa home-based
ment for schizophrenia.
American
nal of Orthopsychiatry
The influence
on the course
illness.
British
Journal
129:125-137,
1976
23.
SM:
treatJour-
J:
Falloon
L, Pederson
rnent in the prevention
schizophrenia:
family
unit.
147:156-163,
Quar-
LeffJP:
of
of
of
Schnur
DB, Friedman
5, Dorman
M, et
al: Assessing
the family
environment
of
schizophrenic
patients
with
multiple
hospital
admissions.
Hospital
and Cornmunity
Psychiatry
37:249-252,
1986
20.
21
terly57:23-57, 1979
CE,
and social factors
psychiatric
Psychiatry
109, 1981
6.
as pre5cr-
Brown
GW, BirleyJLT,
WingJK:
Influence offamily
life on the course ofschizophrenic
disorder:
a replication.
British
Journal
of Psychiatry
121:241-258,
expect
Hospital
32:105-
number
17.
1986
deinstitutionalization?
Community
Psychiatry
and
.
Family
manageof morbidity
of
the adjustment
of
BritishJournal
ofPsychiatry
1985
GoodpastorWA,
121, 1977
RJ: Neuroleptics
of schizophrenia.
17:325-351,
Lehman
AF, Morrissey
for the national
evaluWoodJohnson
Founon Chronic
Mental
Illand Community
Psychiatry4l:1217-1230,
1990
the
1988
BK:
Factors
associated
with multiple
readmissions
to an
urban
public
psychiatric
hospital.
Hospital and Community
Psychiatry
42:8587, 1991
Wyatt
course
Bulletin
Hare
A, Pardes H, Papernik DS, et
al: Aftercare
of psychiatric
patients
and
its relation
to rehospitalization.
Hospital
and Community
Psychiatry
28:118-
1972
Bigelow
DA, Brodsky
G, Stewart
L, et
al: The
concept
and measurement
of
quality
oflife
as a dependent
variable
in
evaluation
of mental
health services, in
Innovative
Approaches
to Mental
Health
Evaluation.
Edited
by Stahler
GH, Tash
WR. New York, Academic
Press,
1982
severity
25. Winston
388, 1986
3.
C: Symptom
Psychiatry
1985
PatrickJ:
Predicting
outcome
ofpsychiatric hospitalization:
a comparison
of attitudinal
and psychopathological
measures.
Journal
of Clinical
Psychology
40:546-549,
1984
B: Quality
ofLife Assessments
in
Trials.
New York, Raven
Press,
FranklinJL,
SimmonsJ,
Solovitz
B, etal:
Assessing
quality
oflife
of the mentally
ill: a three
dimensional
model.
Evaluation and the Health
Profession
9:376-
Community
ofprevious
psychiatric
admissions
dictors
of readmission.
Psychiatric
vices 46:482-485,
1995
662, 1994
16.
References
and
36:1305-1308,
and the natural
Schizophrenia
1991
31
Carpenter
MD, Mulligan
JC, Bader
IA,
et al: Multiple
admissions
to an urban
psychiatric
center:
a comparative
study.
.
Kiesler
native
potential
tients.
360,
CA: Mental
hospitals
care:
noninstitutionalization
public
policy
for
American
Psychologist
1982
and
alteras
mental
pa37:349-
45:455-467,
1975
9.
10.
Mosher
LR, Menn
dential
treatment
two-year
munity
follow-up.
Psychiatry
Lorei TW,
acteristics
employment
Counseling
40:426-430,
AZ: Community
resi-
for schizophrenia:
Hospital
29:715-723,
and
Coming
Com1978
Gurel
L: Demographic
charas predictors
of posthospital
and readmission.
Journal
of
and
Clinical
Psychology
1973
1 1 . Setze PJ, Bond
GR: Psychiatric
recidivism in a psychosocial
rehabilitation
setting:
a survival
analysis.
Hospital
and
Community
Psychiatry
36:52
1-524,
Appleby
Length
phrenia:
13.
Stickney
5K, Hall
RCW,
Gardner
ER:
The effect ofreferral
procedures
on aftercare compliance.
Hospital
and Community Psychiatry
31:567-569,
1980
14.
L, Desai PN, Luchins
DJ, et al:
ofstay
and recidivism
in schizoa study
of public
psychiatric
hospital patients. American Journal
of
Psychiatry
150:72-76,
1993
FranklinJL,KittredgeLD,ThrasherJH:
survey offactors
related
A
Psychiatric
Services
to mental
November
Clinical
Program
4
1985
12.
,
The
in the December
Computing:
of Case
a Consumer’s
Criticisms
Therapy
for Depression
Value
4 Another
A Cognitive
issue
Management
From
Viewpoint
Look at the Token
and Misconceptions
Economy:
hos-
1995
Vol.46
No.11
1165
Carol
Fujihara,
and
participated
Susan
struments
used
in
Essock-Vitale
this
and
the
study,
late
and
Carl
the
was supported
work
Health
tion,
NIMH,
Care
Policy
Care
and
and
the
and
from
3.
Agency
for
Health
Gaumer
GL: Medicare’s
payment
system:
a critical
Health
Care
Financing
Re-
RG, LiveJR,
TaubeCA,
et al: The
of Medicare’s
prospective
paysystem
on psychiatric
patients
in scatterbeds.
Health
EconomHealth
Services
Research
8:1-21,
7.
27.
DesHarnais
SI, Wroblewski
macher
D: How
the Medicare
tive payment
system
affects
patients
treated
in short-term
hospitals.
Inquiry
27:382-388,
15.
Schumacher
DN,
Namerow
et al: Prospective
payment
atry: feasibility
and impact.
land
Journal
of Medicine
28.
Kahn
KL, Rogers
WH,
Rubenstein
LV,
et a!: Measuring
quality
ofcare
with cxplicit process
criteria
before and after the
implementation
ofthe
DRG-based
prospective
payment
system.
JAMA
264:
English
JT, Sharfstein
55, Scherl
DJ, et
al: Diagnosis-related
groups
and general
hospital
psychiatry:
the
APA
study.
American
Journal
of Psychiatry
143:
131-139,
Cromwell
TEFRA
18.
Kahn K, Rubenstein
LV, Draper
D, et al:
The effects
of the DRG-based
prospective payment
system
on quality
of care
fonhospitalized
Medicarepatients:
an introduction
to the series.
JAMA
264:
1953-1955, 1990
19.
Draper
D, Kahn
KL, Reinisch
EF, et a!:
Studying
the effects
of the DRG-based
prospective
payment
system
on quality
ofcare:
design,
sampling,
and fieldwork.
JAMA
20.
Rupp
D, Salkever
D: The
effect
of hospital
payment
methods
on
the pattern
and cost of mental
health
care. Hospital
and Community
Psychia-
try 35:456-459,
10.
1984
Rosenheck
R, Massari
L, Astrachan
BM:
The impact
ofDRG-based
budgeting
on
inpatient
psychiatric
care in Veterans
Administration
medical
centers.
Mcdical Care 28:124-174, 1990
1 1 . Rosenheck
R, Massari
L: Psychiatric
inpatient
care in the VA: before,
during,
and after DRG-based
budgeting.
Amen-
1184
21
1989
A, Steinwachs
1990
Psychiatry 150:1799-1805,
MP,
Ellis
RP,
McGuire
T:
response
to Medicare’s
PPS: rein length
ofstay
for psychiatric
treated
in scatter
beds. Inquiry
26:192-201,
9.
264:1956-1961,
Wells KB, Rogers
WH,
Davis LH, etal:
Quality
ofcarefor
hospitalized
depressed
elderly
patients
before
and after imp!ementation
of the Medicare
prospective
payment
system.
American
Journal
of
(BA).
BeofMental
and Epi-
.
1993
Wells KB, KosecoffJ,Sherwood
M,etal:
Medical
Record
Abstraction
Form
and
Guidelines
for Assessing
Quality
ofCare
for Hospitalized
Patients
With
Depression. Contract
no N-2803-HCFA.
Santa
Monica,
Calif, RAND Corp, 1988
22.
Fleiss JL: Statistical
and Proportions,
Wiley,
1981
23.
LandisJR,
Koch GG: The measurement
of observer
agreement
for categorical
data. Biometrics
33:159-174,
1977
24.
1974-1979,
Methods
2nd
ed.
for Rates
New
York,
LM: Effects
ofMedicare’s
PPS and
Dual Payment
System
on Average Sevenityoflllness
Among
Depressed,
Elderly
Inpatients.
Doctoral
Dissertation, Dept
of Health
Services,
School
of
Public
Health,
University
of California,
Davis
TEFRA
Psychiatric
Services
estimate:
a nonparamethod.
JourStatistical
Associa-
1983
R, Schuprospecpsychiatric
general
1990
1990
29.
Roper
WL: Effectiveness
in health
care:
an initiative
to evaluate
and improve
medical
practice.
New England
Journal
ofMedicine
314:552-578,
1986
30.
Diagnosis
and treatment
ofdepression
in
late life: a consensus
development
cor&rence statement.JAMA
268:10181024,
1991
1986
J, Harrow
B, McGuire
T:
Psychiatric
Hospital
and Unit
Peer Group
and Case Outlier
Analyses,
Task 3 . Final report for contract
no HHS
100-88-0037.
Washington,
DC,
Dcpartment
ofHealth
and Human
Services,
Assistant
Secretary
for Planning
and
Evaluation,Jan
19, 1990
17.
1984 and 1985 . Final report forcontract
no
NIMH-278-86-0002
thesda,
Md, National
Institute
Health,
Division
of Biometry
demiology,
1987
MJ, Parker
for psychiNew
Eng315:1331-
Duan
N: Smearing
metric
retransformation
nal of the American
tion 88:605-610,
1336, 1986
16.
1988
Freiman
MP, Harrow
BS, Stone AG: ImAnalysis
of Options
for Including
Psychiatric
Inpatient
Settings
in a prospective
payment
system:
Descriptive
Analysis
ofMedicare
Discharges
for Psychiatric
Illness
and Substance
Abuse,
Freiman
Provider
ductions
patients
sity
and Probability.
Edited
by LeNeyman
J. Berkeley,
UniverofCalifornia
Press,
1967
LM,
Frank
RG, LaveJR:
Per-case
prospective
payment
for psychiatric
inpatients:
an
assessment
and alternatives.
Journal
of
Health,
Politics,andLaw
143:131-1
39,
1986
pact
8.
Cam
14.
LaveJR,
Frank
RG, Taube
C, et al: The
early
effects
of Medicare’s
prospective
payment
system
on psychiatry.
Inquiry
25:354-363,
Statistics
36:754-
26.
1987
6.
Psychiatry
B,
LaveJR,
Rupp
A, et al: Psychiatry
under
prospective
payment:
cxperience
in the first year. AmericanJournalofPsychiatry
145:210-213,
1988
icsand
BJ, et
Freiman
MP, Goldman
HH, Taube
CA:
Hospitalization
for psychiatric
illness
under
Medicare.
Hospital
and Community Psychiatry
41:5 1-58,
1985
Fogel BS, Slaby AE: Beyond
gamesmanship: strategies
for coping
with prospective payment.
Hospital
and Community
Psychiatry
36:760-763,
1985
treated
Community
Burns
and psychiatric
hospitals
with
units.
Hospital
760, 1985
RF,
Jencks
SF, Horgan
C, Taube
CA: Evidence ofprovider
response
to prospective
payment.
Medical
Care
25(9Xsupp):
S37-S41,
1987
Frank
impact
ment
ThompsonJW,
1991
Huber
PJ: The behavior
of maximum
likelihood
estimates
under
nonstandard
conditions,
in Proceedings
of the Fifth
Berkeley
Symposium
on Mathematical
13.
Research.
4. Taube CA,
5.
LosAngeles,
Administna-
view, ann supp 1991 , pp 45-77
2.
CA,
al: Prospective
payment
discharges
from
general
and without
psychiatric
References
1 . Coulam
prospective
appraisal.
148:888-897,
25.
Taube
12.
of
Health
design.
by grants
Financing
Ms.
Taube
ofPsychiatry
1991
of in-
the National
Institute
ofMental
(NIMH)
assisted
with study
This
canJoumal
Essock-Vitale
in the development
Reviewers
Needed
Psychiatric
Services seeks
expert
meviewers
in the following
areas:
. Outcome
research,
particularly in the area of psychopharmacological
treatment
ofmental
disorders
S
Rating
scales
for symptoms,
outcome,
and other aspects
of treatment
. Dual diagnosis
(mental
illness
and drug
abuse
and mental
illness
and mental
retardation)
. Rural psychiatric
services
. Patient and consumer
perspectives and attitudes
Reviewers
should
be familiar
with
the literature
in their areas of expertise, should
have published
in peerreviewed
journals,
and should
be familiar
with the content
and focus of
Psychiatric
Services.
Prospective
reviewers
should
send
a curriculum
vitae,
specifying
areas
ofinterest,
toJohn
A. Talbott,
M.D.,
Editor,
Psychiatric
Services,
APA,
1400 K Street,
N.W.,
Washington,
D.C. 20005.
November
1995
Vol.
46
No.
11
November1995
PSYCHIATRIC
SERVICES
RESOURCECENTER
a program ofthe American
Psychiatric
for mental health organizations
Center
America’s
Phone: 202/682-6173
Fax:
202/682-6348
Video
Rentals
Order
The
on
Catalog
PBS.
care
Psychiatric
definitive
discussions
Practice
Managed
Care
202/682-6175
and
Newsletter
on Psychiatric
Services
Services
�s Managed
Care
Arthur
confronting
pregnancy
Care
Revolution
I 570
AP9
Psychiatric
202/682-6173
Institute
Managed
Number
America
202/682-6349
1/800/366-8455
Video
Association
of the Month
Video
Services
Resource
Psychiatric
Resources
Center
Revolution
from
Miller
leads
just
a group
of
physicians,
patients,
hospitals,
within
a managed
care system.
executives,
advocates,
and
conclusions
are reached,
related
to the colliding
patient
the
forces
panelists
of the
video
Life”
series
Your
and
actual
scenarios
families
dealing
with
Panelists
include
physicians,
through
a woman’s
managed
a syndicated
columnist.
Although
video
is an excellent
tool
of business
and medicine.
Inc. in association
with Columbia
Thirteen/WNET
New York,
1995.
APA’s
State
Newsletter
a copy
Money
and
Seminars,
ism and
Update
purchased
the “Your
University
Graduate
(60 minutes)
no
for initiating
Produced
by
School
of Journal-
Reports
202/682-6237
New
APPI
Books
York’s
facilities
reportedly
1/800/368-5777
[State
Subscriptions
202/682-6158
Governor
Update,
me more
on membership
Psychiatric
Services
in
the
Center
Times
majority
come at a price,
or hard-to-diagnose
address
in July
authorizing
state
psychiatric
records.
The
patients.
legislation
1995]
published
a five-part
series
ofarticles
Revolution:
Remaking
Medicine
in California”
August
reports
in its first column
that the change
in health care
for the vast
name
a bill
to patients’
criminal
acts of court-committed
Update
The Los Angeles
Resource
signed
August/September
California
Please
send
information
Pataki
to have computer
access
was prompted
by violent
ofpatients.
They
conclude,
however,
which has been paid by the sicken
conditions
and the chronically
highest
level
of HMO
highest
(35.8%),
level
and
(38.3%)
followed
by Oregon
Massachusetts
(35.2%).
The
enrollment,
research
and
is available
delivery,
call
from
reporters
Times
Health
Care
that
these
changes
have
patients,
those with complicated
ill. Among
the states having the
identified
(37.5%),
exhaustive
on Demand,
on “The
27-3 1, 1995.
The Times
delivery
has been positive
California
as having
Maryland
(36.2%),
series took seven
Order
No.
the
Arizona
months
of
401 5, for $8 plus
$3
1-800-440-3441.
fax
to Mary
Return
Submission
Ward
APA
Submissions
Psychiatric
Resource
Services
Center
1400 K Street, NW
Washington,
Fax:
Psychiatric
Deadlines
DC
November
6237;
fax
Mary
202/682-6348
Services
Contact
Submissions
20005
1995
for the
1995.
Vol.
Ward,
46
APA’s
1996
Almost
Institute
Office
Here
on Psychiatric
to Coordinate
Services
the Annual
are
due November
Meetings,
phone
January
5, 1995.
15,
202-682-
202-682-6345.
for the H&CP
phone
No.
11
Achievement
202-682-6173;
Awards
are due
Contact
fax 202-682-6348.
1201
© Copyright 2025 Paperzz