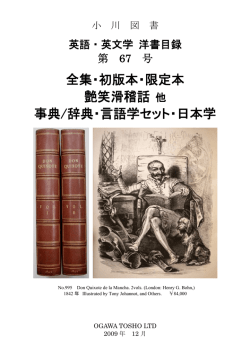
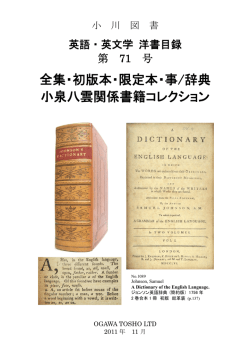
Το άρθρο του µήνα ΥΓΕΙΑ ∆ηµήτρης Παπανδρέου PhD, MS, RD. ∆Ι∆ΑΚΤΩΡ ΙΑΤΡΙΚΗΣ Α.Π.Θ ΠΡΩΤΕΣ ΚΑΜΠΥΛΕΣ ΑΝΑΦΟΡΑΣ ΠΕΡΙΦΕΡΕΙΑΣ ΜΕΣΗΣ ΚΑΙ ΑΝΑΛΟΓΙΑΣ ΠΕΡΙΦΕΡΕΙΑΣ ΜΕΣΗΣ - ΑΝΑΣΤΗΜΑΤΟΣ ΣΕ 607 ΠΑΙ∆ΙΑ ΑΠΟ ΤΗΝ ΘΕΣΣΑΛΟΝΙΚΗ FIRST REFERENCE CURVES OF WAIST CIRCUMFERENCE AND WAIST-TOHEIGHT RATIO OF 607 CHILDREN FROM THESSALONIKI, NORTHERN GREECE Dimitrios Papandreou 2nd Department of Pediatrics, School of Medicine, Aristotle University of Thessaloniki, AHEPA, General Hospital, Thessaloniki, Greece Pavlos Malindretos Nephrology Department, General Hospital of Volos, Volos, Greece, and Israel Rousso 2nd Department of Pediatrics, School of Medicine, Aristotle University of Thessaloniki, AHEPA, General Hospital, Thessaloniki, Greece Το άρθρο δηµοσιεύτηκε στο περιοδικό Nutrition & Food Science Vol. 40 No. 4, 2010 pp. 371-377 Περίληψη Σκοπός – Η περιφέρεια της µέσης (WC) αποτελεί καλύτερο παράγοντα πρόβλεψης κινδύνου καρδιοπάθειας (CVD) από ότι το συνολικό σωµατικό λίπος και πιο ευαίσθητο δείκτη κοιλιακής παχυσαρκίας τόσο για ενήλικες όσο και για παιδιά. Σκοπός της έρευνας είναι να αναφέρει για πρώτη φορά ποσοστιαίες καµπύλες του WC σε παιδιά από την πόλη της Θεσσαλονίκης στην Βόρεια Ελλάδα. Σχεδιασµός/µεθοδολογία/προσέγγιση του προβλήµατος – Συνολικά, συµµετείχαν στην έρευνα 607 παιδιά (324 αγόρια-283 κορίτσια) ηλικίας 7-15 ετών. Υπολογίσθηκαν και παρουσιάστηκαν περιγραφικά στατιστικά για κάθε φύλο και κάθε µία από τις τρεις ηλικιακές κατηγορίες (7-9, 10-12 και 13-15) και οµαλοποιηµένες ποσοστιαίες καµπύλες του WC. Ευρήµατα – Η WC αυξανόταν µε την ηλικία τόσο στα αγόρια όσο και στα κορίτσια. Τα αγόρια είχαν υψηλότερες µέσες τιµές WC στις δύο ηλικιακές οµάδες (10-12 και 13-15 ετών) σε σύγκριση µε τα κορίτσια, ενώ τα κορίτσια είχαν υψηλότερη µέση τιµή στην ηλικιακή οµάδα των 7-9 ετών σε σύγκριση µε τα αγόρια. Τα ποσοστιαία επίπεδα ήταν υψηλότερα για τα κορίτσια άνω του 90ου εκατοστηµορίου των ηλικιακών οµάδων 7-9 και 10-12 ετών. Η WC είχε στενή συσχέτιση µε τον δείκτη σωµατικής µάζας (BMI) (r = 0.90 vs 0.89, για αγόρια και κορίτσια, αντίστοιχα). Παρουσιάστηκαν καµπύλες αναφοράς για την WC για πρώτη φορά. Λαµβάνοντας υπόψη την απουσία τέτοιων τιµών αναφοράς καθώς και την υψηλή συχνότητα παιδιατρικής παχυσαρκίας στα παιδιά στην Βόρεια Ελλάδα, η έρευνα αυτή αποβλέπει να συµβάλλει στον προσδιορισµό και στην πρόληψη των πρώιµων παραγόντων κινδύνου για παιδική παχυσαρκία που σχετίζονται µε υψηλές τιµές WC. Introduction Pediatric obesity is increasing worldwide (Lobstein et al., 2004) and is associated with increased risk of obesity later in life (Reilly et al., 2003). Central obesity in children is related to cardiovascular (CV) risk factors such as hypertension, insulin resistance, diabetes and dyslipidemia (Kelishadi et al., 2007a). Waist circumference (WC) is a specific simple measurement of abdominal obesity in children (Taylor et al., 2000), while body mass index (BMI) may underestimate obesity in youth (McCarthy et al., 2003). Standard WC curves for cardiovascular disease (CVD) have been proposed for adults (WHO, 1998) and are widely used but standards for children have not been presented yet. Age-related references curves for WC have been reported from several countries, such as UK (McCarthy et al., 2001), USA (Fernandez et al., 2004), Cyprus (Savva et al., 2001), Italy (Zannolli and Morgese, 1996) and Turkey (Hatipoglu et al., 2008). However, no other similar studies have been published in northern Greece or other town in the whole Greece. Waist-to height-ratio (WTHR) has been proposed as an alternative method of assessing central fat in children (Taylor et al., 2003). However, WTHR curves have not been reported yet for children because the generality of age and ethnic differences are still questionable. Pediatric obesity in Greece is very high (Krassas et al., 2001). Considering the lack of such reference curves and the need of identifying and preventing obesity in early stage, we now provide for the first time reference curve values of WC and WTHR in a pediatric population from Thessaloniki, northern Greece. Methods A total of 607 children participated in the study (324 boys-283 girls) aged 7-15 years from eight different schools of all areas of Thessaloniki. The children were selected randomly from each school and none of them had any past medical history of any disease or taking any medications. Three age groups were constructed aged 7-9, 10-12 and 13-15. Tanner stage was assessed in all children. This study was approved by the Ethical Committee of Aristotle University of Thessaloniki, Greece. Written, informed consent was also obtained from the parents of each child who participated in the study. Body weight was measured to the nearest of _100 g using a SECA 700 scale model. Subjects were weighted wearing light clothes and without shoes. Height was measured twice using a stadiometer (SECA) to the nearest 0.1 cm. WC was measured using a regular traditional tape (in cm) between the lowest rib and the superior border of the iliac crest to the nearest 0.1 cm. WTHR were calculated by dividing WC by height. BMI was calculated by dividing weight (kg) by height squared (m2). All subjects were classified as normal, overweight and obese according to the international obesity task force (IOTFs) cut off points (Cole et al., 2000). Statistical analysis was performed with SPSS 13.0 (SPSS Inc., Chicago, IL). Smoothed age and gender specific percentiles for WC were constructed by using the LMS method (Cole and Green, 1992). Intercorrelations between BMI and WC and WTHR were assessed using Pearson correlation coefficients. A p-value <0.05 was considered statistically significant. Results A total of 607 children (324 boys and 283 girls) participated in the study. Table I shows all the baseline characteristics of the children. Boys had a higher weight, BMI and WC than girls in two age groups (10-12 and 13-15 years). Table I. Sample sizes, mean and standard deviations for weight, height, BMI, WC and WTHR for 607 Greek children aged 7-15 years Notes: Values are presented as mean_SD; BMI – body mass index; WC – waist circumference; WTHR – waistto-height ratio Smoothed sex and age-specific WC and WTHR percentiles were presented in Tables II and III and Figures 1 and 2. WC increases with age in both boys and girls. Girls had higher percentile values ofWC than boys in two age groups (7-9 and 10-12 years) above the 90th percentile. The values for the 50th and 75th percentile were fairly similar for girls and boys. WTHR decreased with age for the girls, while remained stable for boys. WC and WTHR were strongly correlated with BMI (r Ό 0.90, 0.91 vs 0.89, 0.90 for boys and girls, respectively). Table IV shows a comparison ofWC values of 13 countries for 11 years old boys and girls for the 90th percentile (Schwandt et al., 2008). Discussion Sex and age-specific WC and WTHR percentiles were developed for the first time in a Greek pediatric population aged 7-15 years. As emphasized previously, such reference data may be a useful tool in order to evaluate WC with other possible cardiovascular risk factors since obesity levels in children in northern Greece are very high (Krassas et al., 2001). A comparison of our reference curves with other Mediterranean countries (Italy, Cyprus and Turkey) would be very useful. The 10th, 50th and 90th percentile of our reference curves are higher for both boys and girls compared to other similar percentile curves of Cyprus and Turkey and lower than Italy (data are not shown). A comparison of the 90th percentile of 13 countries shows that 11-year-old Greek girls have the second highest WC values after Italy while boys come in the third position after Italy and Mexico. This should be under serious consideration since dyslipidemia and hypertension in Greek children have been recently growing problems (Magkos et al., 2005). Table II. Age group and sex percentiles of WC for 607 Greek children aged 7-15 years Table III. Age group and sex percentiles of waist circumference/height ratio (WTHR) for 607 Greek children aged 7-15 years Figure 1. Smoothed percentile curves of WC for 607 Greek children aged 7-15 years Children above the 95th and 97th percentile should be under special consideration since it appears to represent extremely obese children. Similar findings are reported from Japan and Iran (Inokuchi et al., 2007; Kelishadi et al., 2007b) The optimal cut off point for WC is varied based on the ethnicity and age-sex specificity. Thus our findings confirm that WC curves may serve as a simple and possible valid epidemiological marker for the assessment of childhood obesity in the area of Thessaloniki, northern Greece. Until now, there is not a universally accepted cut off point of WC related to CVD risk in children. Maffeis et al. (2001) suggested that children above the 90th percentile are more likely to have a multiple CVD risk. WTHR has been now correlated with CVD risk in children (Savva et al., 2000; Hara et al., 2002). Our findings show that WTHR values are independent of age and sex and may be used as a useful additional tool of assessing CVD risk factors. Ashwell et al. (1996) have proposed the use of an age-independent universal cut-off for WTHR of 0.5 which is close to 75th percentile of our study results. However, further studies from Figure 2. Smoothed percentile curves of WC-to-height ratio (WTHR) for 607 Greek children aged 7-15 years Table IV. Comparison of 90th percentile values for WC (cm) of 11-year-old boys and girls from 13 countries comparative correlations with CVD risk in children will be needed in order for WTHR cut off point of 0.5 to become universal. BMI is the most widely used tool index to define if a child is overweight or obese. Our findings thatWC and WTHR are highly correlated with BMI are a little surprising since WC and BMI are increasing with age while WTHR is decreasing with age. Sung et al. (2008) reported that WC correlates with BMI more closely that WTHR. Others have reported that WC and WTHR correlate with CVD in children more strongly than BMI (Savva et al., 2000; Sung et al., 2008). All these differences are probably due to different methods of analysis used by the authors. A limitation of the study is the small number of subjects which did not allow us to have a better picture of percentile curves for each particular age. Nevertheless, it is very interesting to develop a new data and a possible evaluation tool of measuring obesity in the area of Thessaloniki, northern Greece. In conclusion, we presented for the first time WC and WTHR reference curves of children aged 7-15 years from northern Greece were provided. WC remains a simple evaluation tool of measuring central obesity for the prediction of CVD risk in children. WTHR may be used as an additional tool together with WC. Using these reference curves as possible health tool, Greek children from Thessaloniki >90th percentile should be monitored in order to avoid possible disease development later in their life. References Ashwell, M., Lejeune, S. and McPherson, K. (1996), ‘‘Ratio of waist circumference to height may be better indicator of need for weight management’’, BMJ, Vol. 312, p. 377. Cole, J.T. and Green, P.J. (1992), ‘‘Smoothing reference centile curves: the LMS method and penalized likelihood’’, Statistics in Medicine, Vol. 11, pp. 1305-19. Cole, J.T., Bellizzi, C.M., Flegal, K.M. et al. (2000), ‘‘Establishing a standard definition for child overweight and obesity worldwide: international survey’’, BMJ, Vol. 320, pp. 1240-3. Fernandez, J.R., Redden, D.T., Pietrobelli, A. et al. (2004), ‘‘Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents’’, The Journal of Pediatrics, Vol. 145, pp. 439-44. Hara, M., Saitou, E., Iwata, F. et al. (2002), ‘‘Waist-to-height ratio is the best predictor of cardiovascular disease risk factors in Japanese schoolchildren’’, Journal of Atherosclerosis and Thrombosis, Vol. 9, pp. 127-32. Hatipoglu, N., Ozturk, A., Mazicioglu, M.M. et al. (2008), ‘‘Waist circumference percentiles for 7 to 17 years old Turkish children and adolescents’’, European Journal of Pediatrics, Vol. 167, pp. 383-9. Inokuchi, M., Matsuo, N., Anzo, M. et al. (2007), ‘‘Age-dependent percentile for waist circumference for Japanese children based on the 1992-1994 cross-sectional national survey data’’, European Journal of Pediatrics, Vol. 166, pp. 655-61. Kelishadi, R., Gheiratmand, R., Ardalan, G. et al. (2007a), ‘‘CASPIAN Study Group. Association of anthropometric indices with cardiovascular disease risk factors among children and adolescents: CASPIAN Study’’, International Journal of Cardiology, Vol. 117, pp. 340-8. Kelishadi, R., Gouya, M.M., Ardalan, G. et al. (2007b), ‘‘First reference curves of waist and hip circumferences in an Asian population of youths: CASPIAN study’’, Journal of Tropical Pediatrics, Vol. 53, pp. 158-64. Krassas, G.E., Tzotzas, T., Tsametis, C. et al. (2001), ‘‘Prevalence and trends in overweight and obesity among children and adolescents in Thessaloniki, Greece’’, Journal of Pediatric Endocrinology and Metabolism, Vol. 14, pp. 1319-26. Lobstein, T., Baur, L. and Uauy, R. (2004), ‘‘IASO International Obesity TaskForce. Obesity in children and young people: a crisis in public health’’, Obesity Reviews 5, Vol. 1, pp. 4-104. McCarthy, H.D., Ellis, S.M. and Cole, T.J. (2003), ‘‘Central overweight and obesity in British youth aged 11-16 years: cross-sectional surveys of waist circumference’’,BMJ, Vol. 326, pp. 624-27. McCarthy, H.D., Jarrett, K.V. and Crawley, H.F. (2001), ‘‘The development of waist circumference percentiles in British children aged 5.0-16.9 y’’, European Journal of Clinical Nutrition, Vol. 55, pp. 902-7. Maffeis, C., Grezzani, A., Pietrobelli, A. et al. (2001), ‘‘Waist circumference and cardiovascular risk factors in prepubertal children’’, Obesity Research, Vol. 9, pp. 179-87. Magkos, F., Manios, Y., Christakis, G. and Kafatos, A.G. (2005), ‘‘Secular trends in cardiovascular risk factors among school-aged boys from Crete, Greece, 1982-2002’’, European Journal of Clinical Nutrition, Vol. 59 No. 1, pp. 1-7. Reilly, J.J., Methven, E., McDowell, Z.C. et al. (2003), ‘‘Health consequences of obesity’’, Archives of Disease in Childhood, Vol. 88, pp. 748-52. Savva, S.C., Kourides, Y., Tornaritis, M. et al. (2001), ‘‘Reference growth curves for Cypriot children 6 to 17 years of age’’, Obesity Research, Vol. 9, pp. 754-62. Savva, S.C., Tornaritis, M., Savva, M.E. et al. (2000), ‘‘Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index’’, International Journal of Obesity and Related Metabolic Disorders, Vol. 24, pp. 1453-8. Schwandt, P., Kelishadi, R. and Haas, G.M. (2008), ‘‘First reference curves of waist circumference for German children in comparison with international values: the PEP Family Heart Study’’, World Journal of Pediatrics, Vol. 4, pp. 259-66. Sung, R.Y.T., So, H.K., Choi, K.C. et al. (2008), ‘‘Waist circumference and waist-to height ratio of Hong Kong Chinese children’’, BMC Public Health, Vol. 8, pp. 324-31. Taylor, R.W., Jones, I.E., Williams, S.M. and Goulding, A. (2003), ‘‘Evaluation of waist circumference, waist-tohip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3-19 y’’, American Journal of Clinical Nutrition, Vol. 72 No. 2, pp. 490-5. Taylor, R.W., Jones, I.E.,Williams, S.M. et al. (2000), ‘‘Evaluation of waist circumference, waist-tohip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual-energy X-ray absorptiometry, in children aged 3-19 years’’, American Journal of Clinical Nutrition, Vol. 72, pp. 490-5. World Health Organization (1998), ‘‘Preventing and managing the global epidemic. Report of a WHO consultation on obesity’’, WHO/NUT/NCD/98.1,World Health Organization, Geneva. Zannolli, R., and Morgese, G. (1996), ‘‘Waist percentiles: a simple test for atherogenic disease?’’, Acta Paediatrica, Vol. 85, pp. 1368-9.
© Copyright 2025 Paperzz